What is klinefelter's syndrome
Reading File
Finding Sources
Searching PubMed
Klinefelter syndrome
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of Klinefelter syndrome based on authoritative medical textbooks.
Klinefelter Syndrome
Definition & Genetics
Klinefelter syndrome (KS) is defined as male hypogonadism occurring in an individual with two or more X chromosomes and at least one Y chromosome. It is one of the most common sex chromosome disorders and the most common genetic cause of male hypogonadism, occurring in approximately 1 in 660 live male births — though this is likely an underestimate, as mild cases often go undiagnosed.
Karyotypes:
| Type | Karyotype | Frequency |
|---|---|---|
| Classic | 47,XXY | ~90% |
| Mosaic | 46,XY / 47,XXY | ~15% (overlap with classic) |
| Variants | 48,XXXY; 48,XXYY; 49,XXXXY | Rare |
The extra X chromosome arises from nondisjunction during meiosis — maternal and paternal contributions are roughly equal. Advanced maternal age (>40 years) is a risk factor. In mosaics, the presence of a 46,XY cell line is associated with a milder phenotype.
Pathogenesis
Two key mechanisms explain the features of KS:
-
Escape from X-inactivation (Lyonization): Although all but one X chromosome undergoes inactivation, ~35% of X-linked genes escape this inactivation. The resulting "overdose" of these genes — including the SHOX gene (Short-stature Homeobox gene) on the pseudoautosomal region of Xp — drives tall stature and long legs. Genes upregulated also affect autosomes.
-
Androgen receptor CAG repeats: The androgen receptor gene on the X chromosome contains polymorphic CAG trinucleotide repeats. Shorter repeats = greater androgen sensitivity. In KS, the X chromosome with the shortest CAG repeat is preferentially inactivated, leaving receptors with long (less sensitive) CAG repeats, which worsens hypogonadism.
Clinical Features
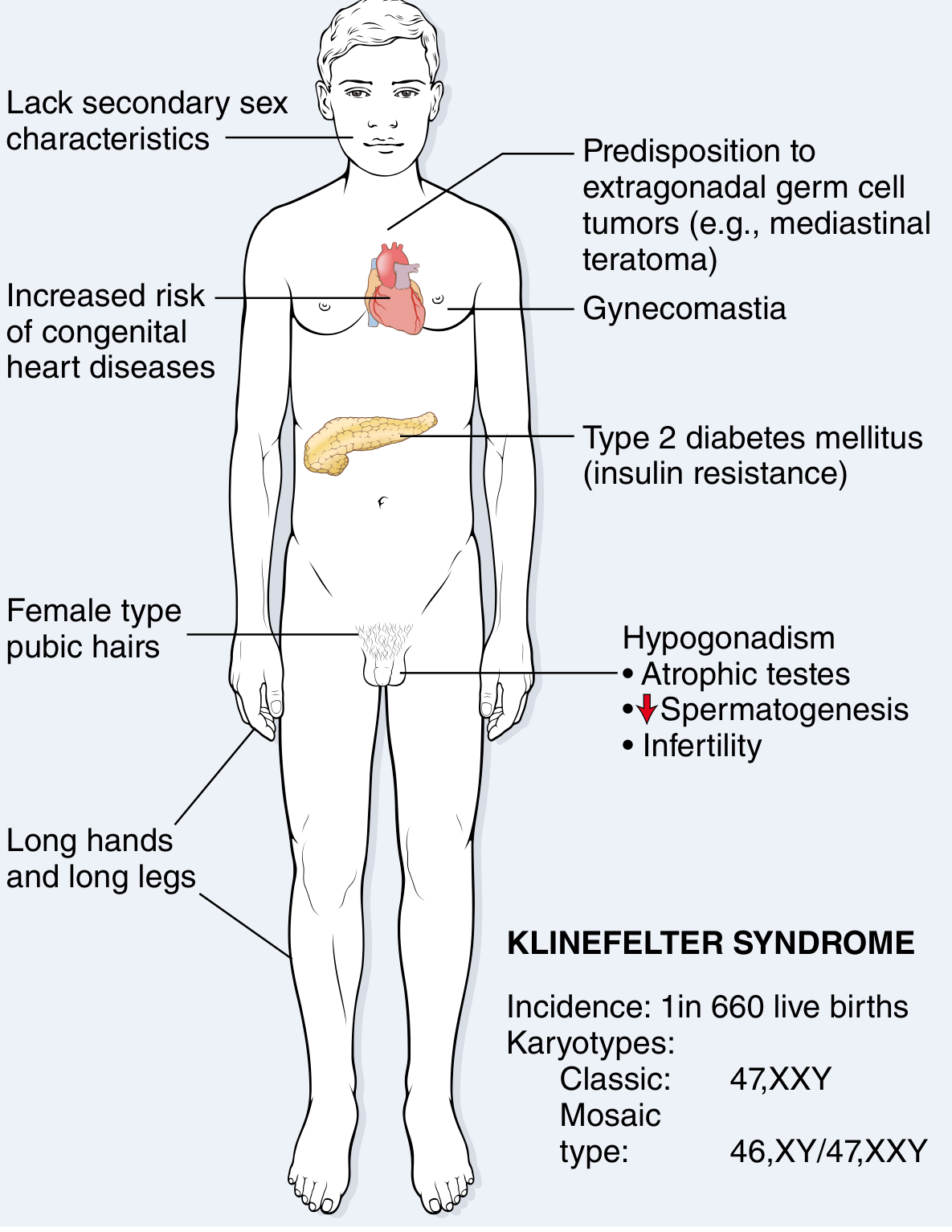
The only universal finding is hypogonadism. Other features are variable:
Body Habitus
- Tall stature with disproportionately long legs (increased sole-to-pubic bone distance)
- Long hands and feet
- Eunuchoid body proportions
Reproductive/Sexual
- Small, atrophic testes (sometimes as small as 2 cm)
- Small penis
- Reduced or absent facial, body, and pubic hair (female-type pubic hair distribution)
- Gynecomastia
- Decreased libido
Endocrine & Lab Findings
- Low or low-normal testosterone
- Elevated FSH (consistently high — reflects testicular failure)
- Elevated estradiol (mechanism unclear; determines degree of feminization)
Fertility
- Azoospermia or severe oligospermia in most cases
- Infertility is the rule; fertility is only occasionally seen in mosaics with a large 46,XY cell population
- Histology: hyalinization/ghost tubules, apparent Leydig cell prominence
Cognitive & Neurological
- Cognitive abilities range from average to below average
- Modest deficits in verbal skills, reading, and language comprehension
- Increased rates of anxiety, speech delay
Associated Comorbidities
| System | Complication |
|---|---|
| Cardiovascular | Mitral valve prolapse (~50% of adults), atrial/ventricular septal defects |
| Metabolic | Type 2 diabetes mellitus, metabolic syndrome, insulin resistance |
| Bones | Osteoporosis and fractures (due to sex hormone imbalance) |
| Malignancy | 20–30× increased risk of extragonadal germ cell tumors (especially mediastinal teratomas); increased breast cancer risk |
| Autoimmune | Systemic lupus erythematosus and other autoimmune diseases |
| Vascular | Thromboembolic disease, varicose veins |
| Endocrine | Hypothyroidism |
Diagnosis
- Karyotyping is confirmatory
- Rarely diagnosed before puberty (features appear at early puberty)
- Hormonal profile: ↑FSH, ↑LH, ↓/normal testosterone, ↑estradiol
Management
- Testosterone replacement therapy — initiated at puberty; improves virilization, libido, bone density, and mood; does not restore fertility
- Assisted reproduction — testicular sperm extraction (TESE) is possible in some patients (especially mosaics) for intracytoplasmic sperm injection (ICSI)
- Growth, endocrine function, and bone mineral density monitoring, especially from adolescence
- Educational and psychological support
- Screening and surveillance for comorbidities (diabetes, cardiac, osteoporosis, malignancy)
Sources: Robbins, Cotran & Kumar — Pathologic Basis of Disease; Robbins & Kumar Basic Pathology; Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.