What is dosage in pharmacology?
Reading File
Finding Sources
Searching the Web
dosage pharmacology definition types dose-response
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Here is a thorough explanation of dosage in pharmacology, drawn from Lippincott's Illustrated Reviews: Pharmacology and Katzung's Basic and Clinical Pharmacology (16th Edition):
Dosage in Pharmacology
Definition
Dosage refers to the administration of a drug in prescribed amounts as part of a medication regimen. It encompasses not just how much of a drug is given, but also how often and by what route. The key terms are:
| Term | Meaning |
|---|---|
| Dose | The amount of drug taken at any one time (e.g., 500 mg) |
| Dosage regimen | The frequency at which doses are given (e.g., 500 mg every 8 hours) |
| Total daily dose | Dose x number of times per day |
| Dosage form | Physical form of the drug (tablet, capsule, liquid, injection) |
| Strength | Amount of drug per unit (e.g., 250 mg/5 mL) |
| Route of administration | How the drug enters the body (oral, IV, topical, etc.) |
Designing a Dosage Regimen
To initiate drug therapy, the clinician must select the appropriate route of administration, dosage, and dosing interval. Selection depends on patient and drug factors, including how quickly therapeutic levels must be achieved.
1. Single Dose
Some drugs are given just once - for example, a sleep-inducing agent like zolpidem.
2. Repeated / Continuous Dosing
More commonly, drugs are given repeatedly (e.g., "one tablet every 4 hours") or as a continuous IV infusion. This leads to drug accumulation until a steady state is reached - where the rate of elimination equals the rate of administration.
Steady-state concentration (C_ss) is directly proportional to the infusion rate, and inversely proportional to drug clearance.
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
Key Types of Doses
Maintenance Dose
The maintenance dose keeps the drug at a steady therapeutic level - the amount given replaces what was eliminated since the last dose. It is calculated using:
Maintenance Dose = Dosing Rate x Dosing Interval Dosing Rate = Clearance (CL) x Target Concentration (TC)
Clearance is the most important pharmacokinetic parameter for designing a maintenance regimen.
Loading Dose
When a rapid therapeutic effect is needed, a loading dose is given upfront to quickly achieve target plasma concentrations. It is calculated based on the volume of distribution (Vd):
Loading Dose = Target Concentration x Volume of Distribution (Vd)
The Target Concentration Approach
A rational dosage regimen is built around the idea of a target concentration - the plasma level that produces the desired therapeutic effect without toxicity. By accounting for pharmacokinetic parameters (clearance, Vd, bioavailability), the dose can be individualized.
For example, digoxin for atrial fibrillation may require a target of 2 ng/mL, while heart failure is managed at 1 ng/mL - the same drug, but different dosage goals for different conditions.
Factors That Require Dose Adjustment
Dosage must be adjusted when the drug's half-life changes due to:
- Decreased renal/hepatic blood flow (e.g., heart failure, shock) - longer half-life, lower dose needed
- Renal disease - reduced drug extraction from plasma
- Drug interactions - enzyme inhibitors raise plasma levels
- Hepatic insufficiency (e.g., cirrhosis) - decreased metabolism
- Increased metabolism - shorter half-life, higher dose may be needed
"Patients who may have an increase in drug half-life...may require a decrease in dosage or less frequent dosing intervals."
- Lippincott's Illustrated Reviews: Pharmacology
Summary
| Concept | Key Point |
|---|---|
| Dose | Amount per administration |
| Dosing interval | Time between doses |
| Maintenance dose | Keeps drug at steady state; driven by clearance |
| Loading dose | Achieves rapid effect; driven by volume of distribution |
| Steady state | When elimination rate = administration rate |
| Dose adjustment | Required in renal/hepatic impairment, drug interactions, age extremes |
Getting dosage right is the core challenge in pharmacotherapy - too little fails to treat, too much causes toxicity. The therapeutic window (the range between minimum effective concentration and minimum toxic concentration) guides dosage selection.
Sources: Lippincott's Illustrated Reviews: Pharmacology | Katzung's Basic and Clinical Pharmacology, 16th Edition
Route of Drug Administration in Pharmacology.
Finding Sources
Searching the Web
routes of drug administration pharmacology enteral parenteral overview
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, textbook-grounded overview of Routes of Drug Administration in Pharmacology.
Routes of Drug Administration in Pharmacology
The route of administration is determined by two key factors:
- Properties of the drug - water/lipid solubility, stability in the GI tract, ionization
- Therapeutic objectives - need for rapid onset, long-term treatment, or local effect
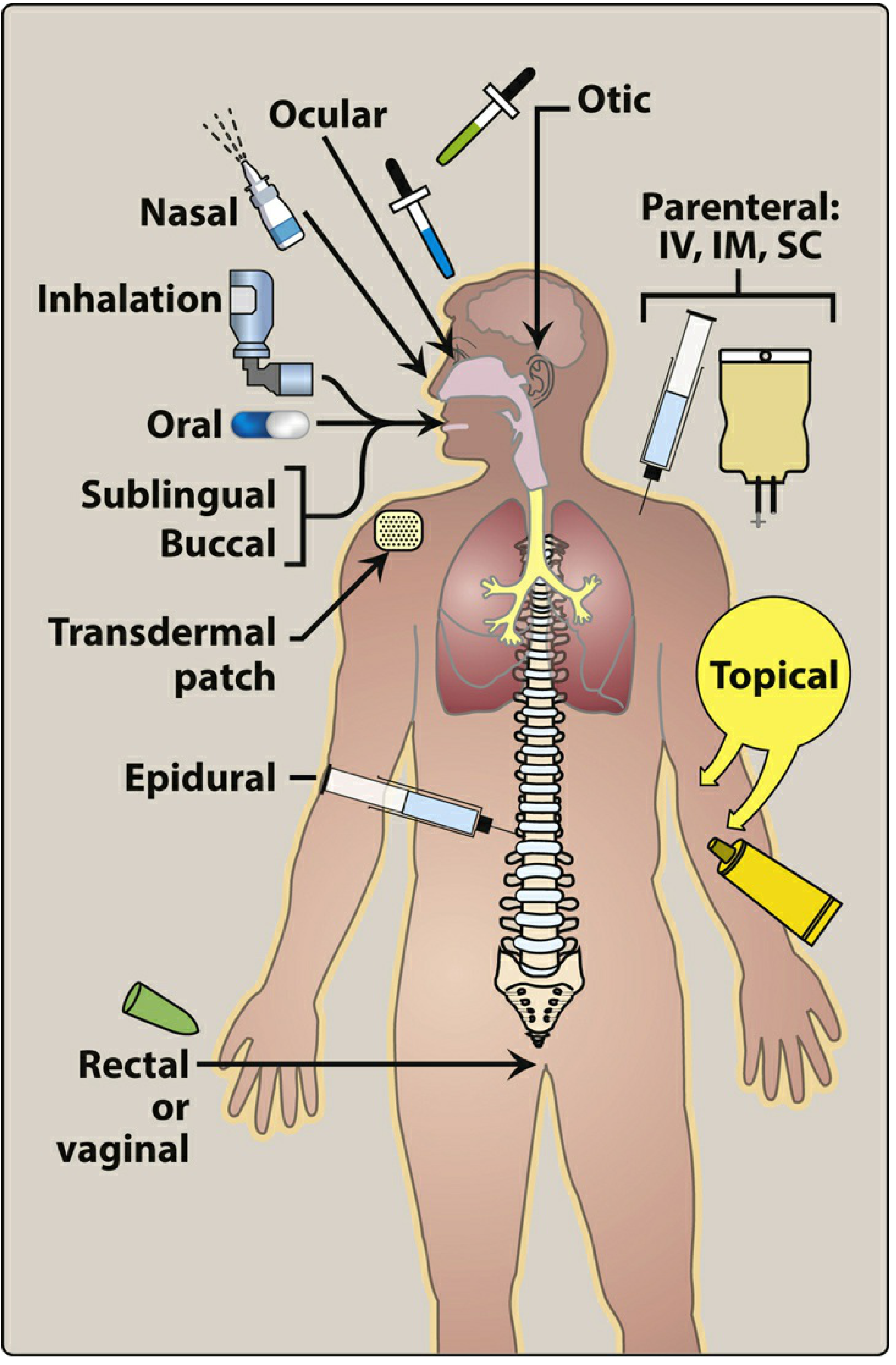
The major categories are: Enteral, Parenteral, and Other (topical, inhalation, transdermal, etc.)
A. ENTERAL ROUTES
Enteral administration means placing a drug in the gastrointestinal tract. It is the most common, convenient, and economical method.
1. Oral (PO - Per Os)
Drug is swallowed and absorbed through the GI tract.
| Absorption | Variable - affected by gastric pH, food, motility |
| Advantages | Self-administered, safe, economical, can use activated charcoal for overdose |
| Disadvantages | First-pass metabolism, destroyed by gastric acid, slow onset, cannot use in unconscious patients |
| Examples | Acetaminophen, Amoxicillin |
Special oral preparations:
- Enteric-coated: Chemical coating protects acid-labile or stomach-irritating drugs (e.g., omeprazole, aspirin) - dissolves only in the intestine
- Extended-release (ER/XR/SR/CR): Slower absorption, prolonged duration, fewer daily doses, better compliance. Example: oral morphine ER (2x/day instead of 6x/day)
2. Sublingual / Buccal
- Sublingual: Drug placed under the tongue
- Buccal: Drug placed between cheek and gum
- Both allow direct absorption into the bloodstream via the oral mucosa
- Key advantage: Bypass first-pass metabolism and stomach acid destruction
- Example: Nitroglycerin (rapid onset in angina)
3. Rectal
- About 50% of rectal drainage bypasses the portal circulation, reducing first-pass metabolism
- Useful when patient is vomiting, unconscious, or the drug causes nausea orally
- Disadvantage: Absorption is often erratic and incomplete; may irritate rectal mucosa
B. PARENTERAL ROUTES
Parenteral routes introduce drugs directly into the systemic circulation, bypassing the GI tract. Used when:
- Drug is poorly/not absorbed orally (e.g., heparin)
- Drug is unstable in the GI tract (e.g., insulin)
- Patient is unconscious
- Rapid onset is required
"Parenteral administration provides the most control over the dose of drug delivered to the body. However, this route is irreversible and may cause pain, fear, local tissue damage, and infections."
- Lippincott's Illustrated Reviews: Pharmacology
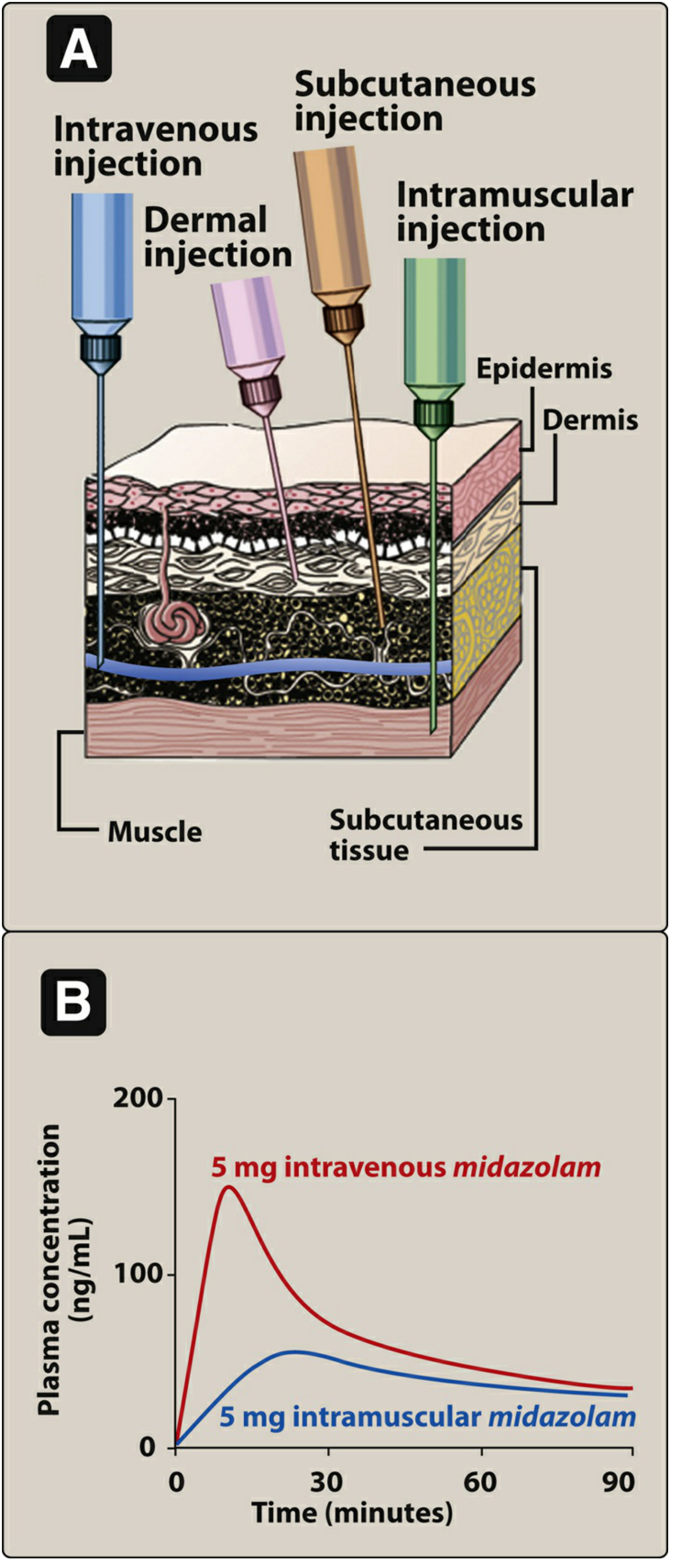
1. Intravenous (IV)
- Drug delivered directly into a vein - highest bioavailability (100%)
- Fastest onset - nearly immediate effect
- IV bolus: Full dose delivered almost instantly
- IV infusion: Drug given over time - lower peak, longer duration
- Used for: rocuronium, many antibiotics, emergency drugs
2. Intramuscular (IM)
- Drug injected into muscle tissue
- Aqueous solutions: Absorbed rapidly
- Depot preparations (oil or polyethylene glycol vehicle): Drug precipitates at injection site, dissolves slowly - provides sustained effect over days/weeks (e.g., benzathine penicillin G, long-acting antipsychotics)
3. Subcutaneous (SC)
- Injection into the tissue just beneath the skin
- Absorption by simple diffusion - slower than IV but more sustained
- Minimizes risk of hemolysis or thrombosis
- Avoid in drugs that cause tissue irritation (risk of necrosis)
- Examples: insulin, heparin, vaccines
4. Intradermal (ID)
- Injection into the dermis (just below epidermis)
- Used for diagnostic tests (e.g., tuberculin skin test) and desensitization
- Small volumes only
C. OTHER ROUTES
5. Inhalation
- Drug delivered as gas or aerosol directly to the pulmonary epithelium
- Onset nearly as fast as IV bolus due to the large surface area and rich blood supply
- Ideal for respiratory diseases (asthma, COPD) - drug acts at site of disease, minimizing systemic side effects
- Examples: salbutamol inhaler, inhaled anesthetics (gases)
6. Nasal
- Drug applied to nasal mucosa
- Used for allergic rhinitis, and for systemic delivery of some peptides
- Examples: intranasal corticosteroids, desmopressin
7. Transdermal
- Drug applied to skin surface (usually via a patch) for systemic absorption
- Absorption depends on lipid solubility of the drug and skin characteristics at the site
- Provides slow, sustained delivery - avoids first-pass metabolism
- Examples: nitroglycerin patch, nicotine patch, fentanyl patch
8. Topical
- Applied to skin or mucous membrane for a local effect
- Examples: antifungal creams, eye drops, ear drops
9. Intrathecal / Intraventricular
- Drug injected directly into cerebrospinal fluid (CSF)
- Used when the blood-brain barrier prevents adequate CNS drug levels
- Used for: spinal anesthesia, intrathecal chemotherapy (e.g., methotrexate)
Summary Comparison Table
| Route | Onset | Bioavailability | First-Pass? | Key Use |
|---|---|---|---|---|
| Oral | Slow (30-90 min) | Variable | Yes | Most drugs |
| Sublingual | Fast (2-5 min) | High | No | Nitroglycerin |
| Rectal | Moderate | Partial | Partial | Vomiting/unconscious patients |
| IV | Immediate | 100% | No | Emergencies, precise dosing |
| IM | Moderate-fast | High | No | Vaccines, depot drugs |
| SC | Slow-moderate | Good | No | Insulin, heparin |
| Inhalation | Very fast | High (lungs) | No | Asthma, anesthesia |
| Transdermal | Slow | Variable | No | Long-acting systemic drugs |
| Topical | Local | Minimal systemic | No | Skin/eye/ear conditions |
| Intrathecal | Immediate (CNS) | Direct CNS | N/A | CNS infections, anesthesia |
"The most efficient and straightforward means of administering a drug into the systemic circulation is by intravenous injection of a bolus."
- Goldman-Cecil Medicine, International Edition
Sources: Lippincott's Illustrated Reviews: Pharmacology | Goldman-Cecil Medicine, International Edition
Efficacy in Pharmacology
Finding Sources
Searching the Web
efficacy pharmacology definition intrinsic activity potency maximal effect
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Excellent - I now have all the textbook content and diagrams needed for a comprehensive answer.
Efficacy in Pharmacology
Definition
Efficacy (also called maximal efficacy or E_max) is the maximum effect a drug can produce, regardless of how high the dose is increased. It reflects the intrinsic ability of a drug-receptor complex to generate a biological response - not just how well a drug binds, but how powerfully it activates what it binds to.
"The maximal efficacy of a drug is obviously crucial for making clinical decisions when a large response is needed. It may be determined by the drug's mode of interactions with receptors (as with partial agonists), or by characteristics of the receptor-effector system involved."
- Katzung's Basic and Clinical Pharmacology, 16th Edition
Efficacy vs. Potency - A Critical Distinction
These two terms are frequently confused but describe completely different properties:
| Property | Definition | Measured by | Clinical relevance |
|---|---|---|---|
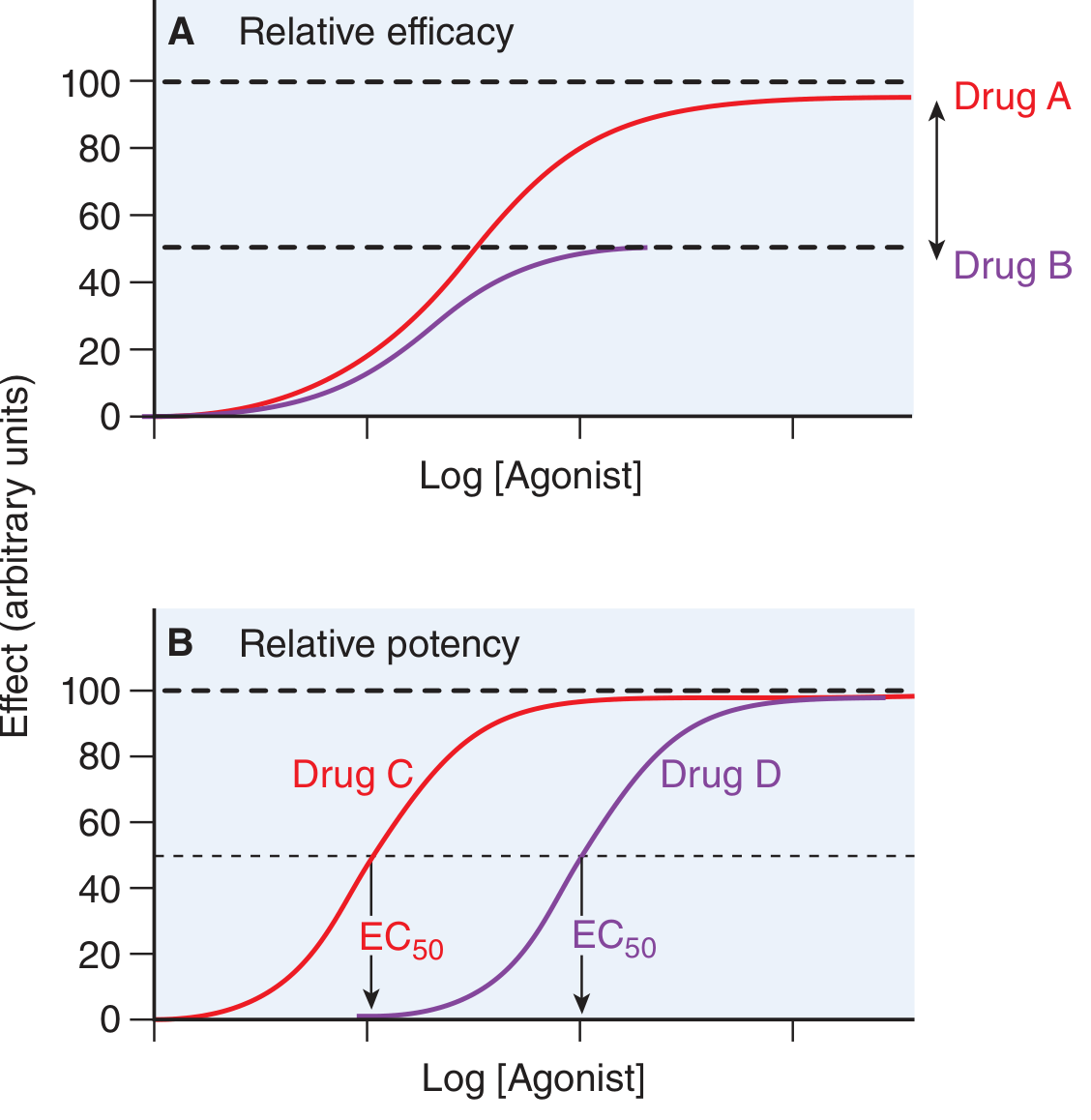
| Efficacy (E_max) | The maximum effect a drug can produce | Height of the dose-response curve | Determines whether a drug can produce a strong enough effect |
| Potency | The dose/concentration needed to produce 50% of the maximal effect | EC50 or ED50 (position on the x-axis) | Determines how much drug you need to give |
A drug can be highly potent but have low efficacy (e.g., a partial agonist that works at low concentrations but can never reach a full response). Conversely, a drug can have low potency but high efficacy (needs a large dose, but at that dose achieves a full response).
Intrinsic Activity and Efficacy
Intrinsic activity is the drug's ability to fully or partially activate receptors once bound. It determines where a drug falls on the efficacy spectrum:
"The intrinsic activity of a drug further determines its ability to fully or partially activate the receptors."
- Lippincott's Illustrated Reviews: Pharmacology
1. Full Agonists (Intrinsic Activity = 1)
- Bind to a receptor and produce the maximum possible biological response - equal to that of the endogenous ligand
- Stabilize the receptor in its active state (R)*
- All full agonists at the same receptor produce the same E_max
- Example: Phenylephrine is a full agonist at α1-adrenoceptors, producing the same E_max as the endogenous ligand norepinephrine
2. Partial Agonists (0 < Intrinsic Activity < 1)
- Even when all receptors are occupied, cannot produce the same E_max as a full agonist
- Can act as both agonist and antagonist - in the presence of a full agonist, a partial agonist reduces the full agonist's effect (by competing for receptor occupancy)
- Example: Aripiprazole (atypical antipsychotic) is a partial agonist at dopamine receptors - it inhibits overactive dopaminergic pathways while stimulating underactive ones
3. Inverse Agonists (Intrinsic Activity < 0)
- Some receptors show spontaneous activity even without a drug (constitutive activity)
- Inverse agonists stabilize the inactive receptor state (R), reducing baseline receptor activity below the level seen with no drug at all
- They produce the opposite pharmacological effect of agonists
4. Antagonists (Intrinsic Activity = 0)
- Bind with high affinity but produce no biological response on their own
- Block agonist access/activation:
- Competitive antagonists: Shift the agonist dose-response curve to the right (increase EC50) - but E_max is preserved because more agonist can overcome the block
- Noncompetitive (irreversible/allosteric) antagonists: Cause a downward shift of E_max (reduce efficacy) without changing EC50

Clinical Importance of Efficacy
- Drug selection: When a strong effect is needed (e.g., severe pain, acute heart failure), a drug with high efficacy is required. A partial agonist may not be enough.
- Ceiling effect: Efficacy sets the maximum achievable response - increasing the dose beyond E_max produces no additional benefit, only more side effects.
- Practical limitations: Even if a drug has high theoretical efficacy, its practical efficacy may be limited by toxicity at doses needed to achieve it (e.g., a drug that causes fatal arrhythmia before it can maximally increase cardiac contractility).
- Partial agonists in therapy: Their dual agonist/antagonist nature can be therapeutically useful - e.g., aripiprazole in schizophrenia, buprenorphine in opioid dependence.
Summary
| Drug Type | Intrinsic Activity | E_max | Clinical Example |
|---|---|---|---|
| Full agonist | 1 | Maximum (=endogenous ligand) | Morphine, phenylephrine |
| Partial agonist | 0 to 1 | Submaximal | Aripiprazole, buprenorphine |
| Inverse agonist | < 0 | Below baseline | Some antihistamines |
| Competitive antagonist | 0 | No effect alone; reduces potency of agonist | Terazosin, naloxone |
| Noncompetitive antagonist | 0 | No effect alone; reduces efficacy of agonist | Phenoxybenzamine, picrotoxin |
Sources: Lippincott's Illustrated Reviews: Pharmacology | Katzung's Basic and Clinical Pharmacology, 16th Edition
Drug in Pharmacology
Finding Sources
Searching the Web
drug definition pharmacology classification types sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have rich, authoritative content from Katzung's Basic and Clinical Pharmacology (16th Edition) to deliver a comprehensive answer.
Drug in Pharmacology
Definition
"In the most general sense, a drug may be defined as any substance that brings about a change in biologic function through its chemical actions."
- Katzung's Basic and Clinical Pharmacology, 16th Edition
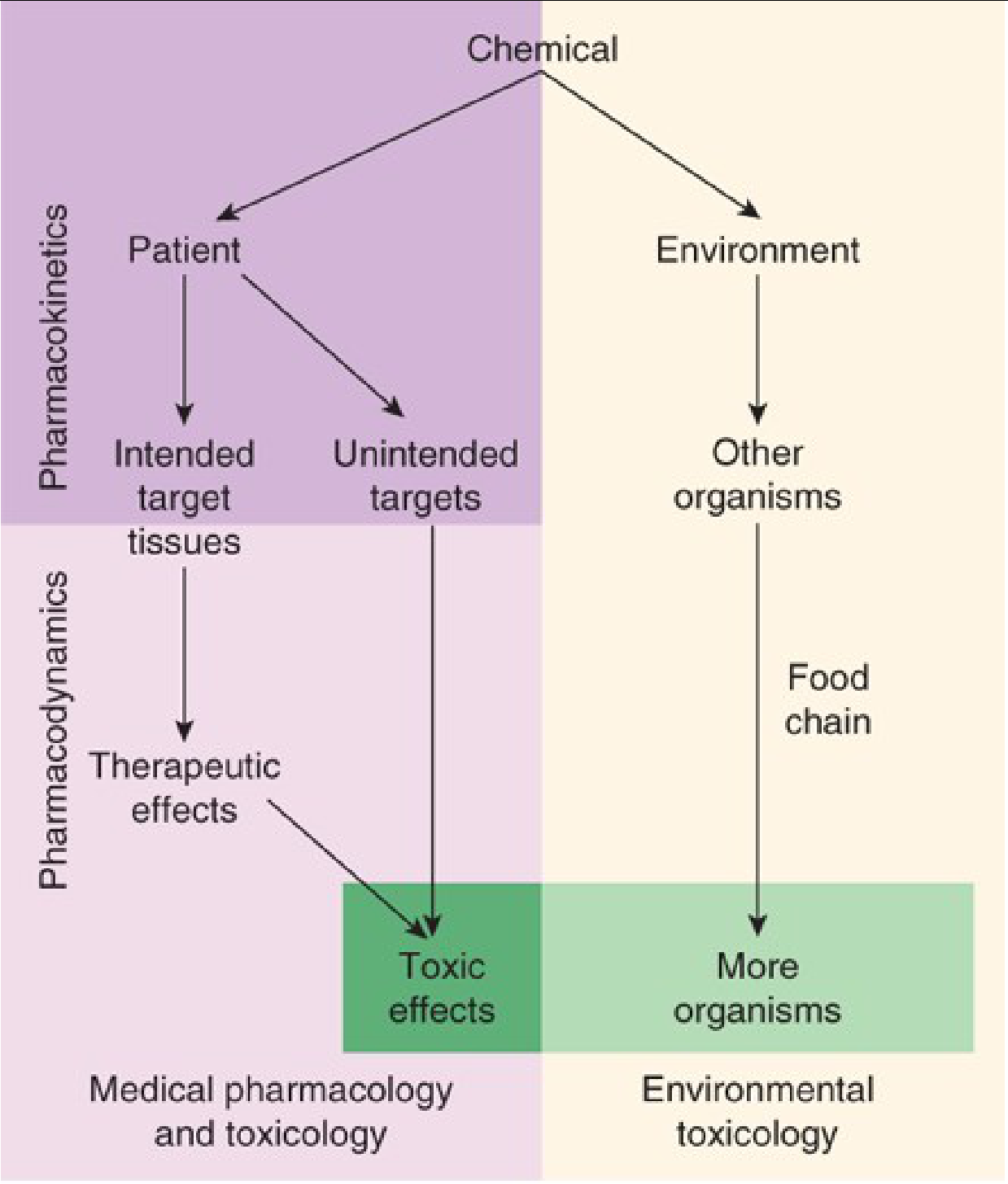
More formally, pharmacology is the study of substances that interact with living systems through chemical processes - typically by binding to regulatory molecules and activating or inhibiting normal body processes.
Medical pharmacology is defined as the science of substances used to prevent, diagnose, and treat disease.
Toxicology is the branch of pharmacology dealing with the undesirable effects of chemicals on living systems.
How Drugs Work
In most cases, a drug molecule interacts with a receptor - a specific target molecule that plays a regulatory role in the biological system - either as:
- An agonist (activator) - turns the receptor on
- An antagonist (inhibitor) - blocks the receptor
Some newer large molecule drugs (biologicals) act like receptors themselves and bind endogenous molecules. A few drugs (e.g., osmotic agents like mannitol) work almost exclusively with water molecules.
Types of Drugs by Origin
| Type | Description | Examples |
|---|---|---|
| Endogenous | Synthesized within the body | Hormones (insulin, adrenaline) |
| Xenobiotics | Chemicals not made in the patient's body | Most synthetic drugs |
| Poisons | Drugs with almost exclusively harmful effects | Arsenic, cyanide |
| Toxins | Poisons of biological origin (from plants or animals) | Botulinum toxin, snake venom |
"Paracelsus (1493-1541) famously stated that 'the dose makes the poison,' meaning that any substance can be harmful if taken in the wrong dosage."
- Katzung's Basic and Clinical Pharmacology
The Physical Nature of a Drug
For a drug to interact with its receptor and be therapeutically useful, it must have:
1. Appropriate Size
- Drug molecular weights range from very small (lithium ion, MW = 7) to very large (alteplase/t-PA, MW = 59,050; antibodies >145,000)
- Most drugs fall between MW 100 and 1000
- Too small: not specific enough to bind only one receptor type
- Too large: cannot diffuse freely between body compartments (very large drugs must be injected directly)
2. Appropriate Physical State
Drugs may be:
- Solid at room temperature (e.g., aspirin, atropine)
- Liquid (e.g., nicotine, ethanol)
- Gaseous (e.g., nitrous oxide, isoflurane, xenon)
This determines the best route of administration.
3. Chemical Character
- Many drugs are weak acids or bases - the degree of ionization in different body compartments (due to pH differences) affects their absorption, distribution, and excretion
- Inorganic elements like lithium, iron, fluoride are both useful and dangerous drugs
- Drugs span all classes of organic compounds: carbohydrates, proteins, lipids, and small molecules
4. Chirality (Shape)
- More than half of all useful drugs are chiral molecules (they exist as mirror-image pairs called enantiomers)
- The more active enantiomer typically has a better fit to the receptor - like a left hand fitting a left-handed glove
- Example: Carvedilol - the (S)-isomer is a potent β-blocker; the (R)-isomer is 100-fold weaker at β-receptors
- Example: Ketamine - the racemic mix is used as an anesthetic; the (S)-enantiomer is approved as a nasal spray antidepressant (esketamine)
Two Core Branches of Pharmacology
| Branch | What it studies | Key Question |
|---|---|---|
| Pharmacokinetics | What the body does to the drug (Absorption, Distribution, Metabolism, Excretion - ADME) | How does the drug reach its target? |
| Pharmacodynamics | What the drug does to the body (mechanism of action, dose-response, efficacy, potency) | What does the drug do once it gets there? |
Why New Drugs Are Needed
New drugs are continuously being developed because of:
- Increasing resistance by bacteria and other parasites
- Discovery of new disease targets - processes not previously treatable
- Recognition of new diseases
- Growth of large molecule drugs - especially monoclonal antibodies (MAbs), which rose from ~2% of new drug approvals in 2000 to ~16% by 2020
General Principles About Drugs
- All substances can be toxic under certain circumstances - it is always a matter of dose
- Chemicals in botanicals (herbs/nutraceuticals) are no different from chemicals in manufactured drugs, except for a higher proportion of impurities
- All health-promoting substances should meet the same standards of efficacy and safety as conventional drugs - ideally tested in randomized controlled trials (RCTs)
Source: Katzung's Basic and Clinical Pharmacology, 16th Edition (Todd W. Vanderah & Bertram G. Katzung)
Potency in Pharmacology
Finding Sources
Searching the Web
potency pharmacology EC50 ED50 definition dose response curve
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
All the key content and diagrams are in hand. Here is the full, authoritative answer.
Potency in Pharmacology
Definition
"Potency refers to the concentration (EC50) or dose (ED50) of a drug required to produce 50% of that drug's maximal effect."
- Katzung's Basic and Clinical Pharmacology, 16th Edition
More precisely, potency is an expression of the activity of a drug in terms of the concentration or amount required to produce a defined effect. The lower the dose or concentration needed to produce that effect, the more potent the drug.
- A drug whose dose-response curve lies to the left on the dose axis is more potent
- A drug requiring higher doses to produce the same effect is less potent
"Potency does not refer to the maximum effect attainable."
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
Key Measures of Potency
| Term | Full Name | Definition |
|---|---|---|
| EC50 | Effective Concentration 50 | Concentration producing 50% of maximal effect in a single patient or tissue |
| ED50 | Effective Dose 50 | Dose producing a specified effect in 50% of a population |
| TD50 | Toxic Dose 50 | Dose producing a toxic effect in 50% of a population |
| LD50 | Lethal Dose 50 | Dose causing death in 50% of a population |
A lower EC50 / ED50 = higher potency (the drug works at smaller amounts).
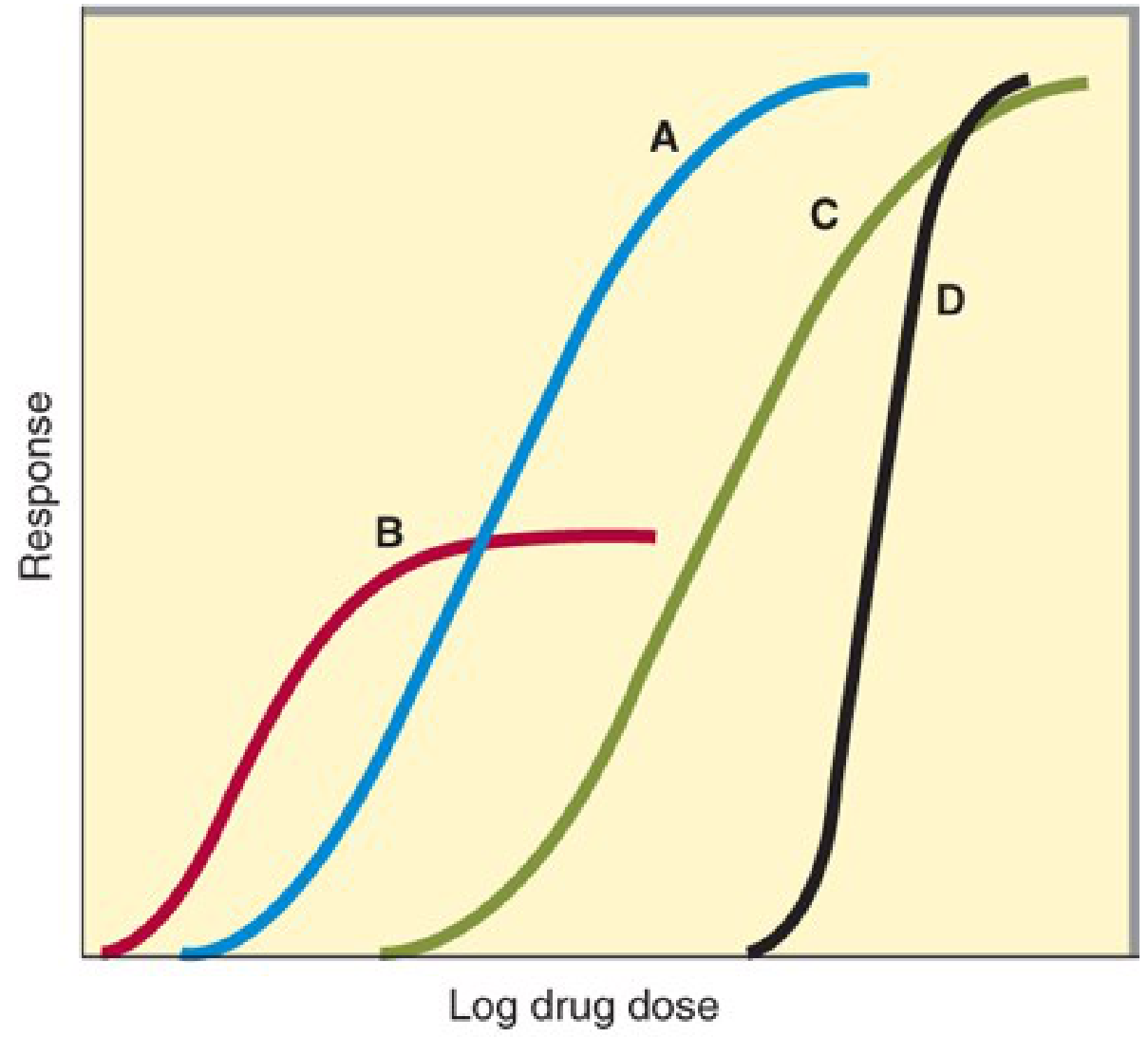
The Dose-Response Curve and Potency
When drug response is plotted against log drug dose, a characteristic sigmoid (S-shaped) curve results. The position of this curve along the horizontal (dose) axis reflects potency:
What Determines Potency?
Potency depends on two factors:
- Affinity (Ka) - how strongly the drug binds to its receptor. Higher affinity = lower concentration needed to occupy receptors = higher potency
- Coupling efficiency - how efficiently drug-receptor binding is translated into a biological response (signal transduction efficiency)
Potency vs. Efficacy - The Critical Distinction
| Property | What it measures | On the dose-response curve | Clinical importance |
|---|---|---|---|
| Potency | How much drug is needed | Position along the X-axis (EC50) | Determines the dose size required |
| Efficacy | How strong the maximum effect is | Height of the plateau (E_max) | Determines whether the drug can produce a sufficient therapeutic response |
Key clinical insight: A drug can be more potent but less efficacious than another drug:
- Drug B (partial agonist) may have a lower EC50 (more potent) than Drug A, yet Drug A still achieves a larger maximum response (higher efficacy)
- Some doses of Drug A can produce larger effects than any dose of Drug B, despite Drug B being pharmacologically more potent
Quantal Dose-Effect Curves and Population Potency
When measuring potency across a population (rather than a single patient), a quantal dose-effect curve is used - showing the cumulative percentage of individuals who respond at each dose level.
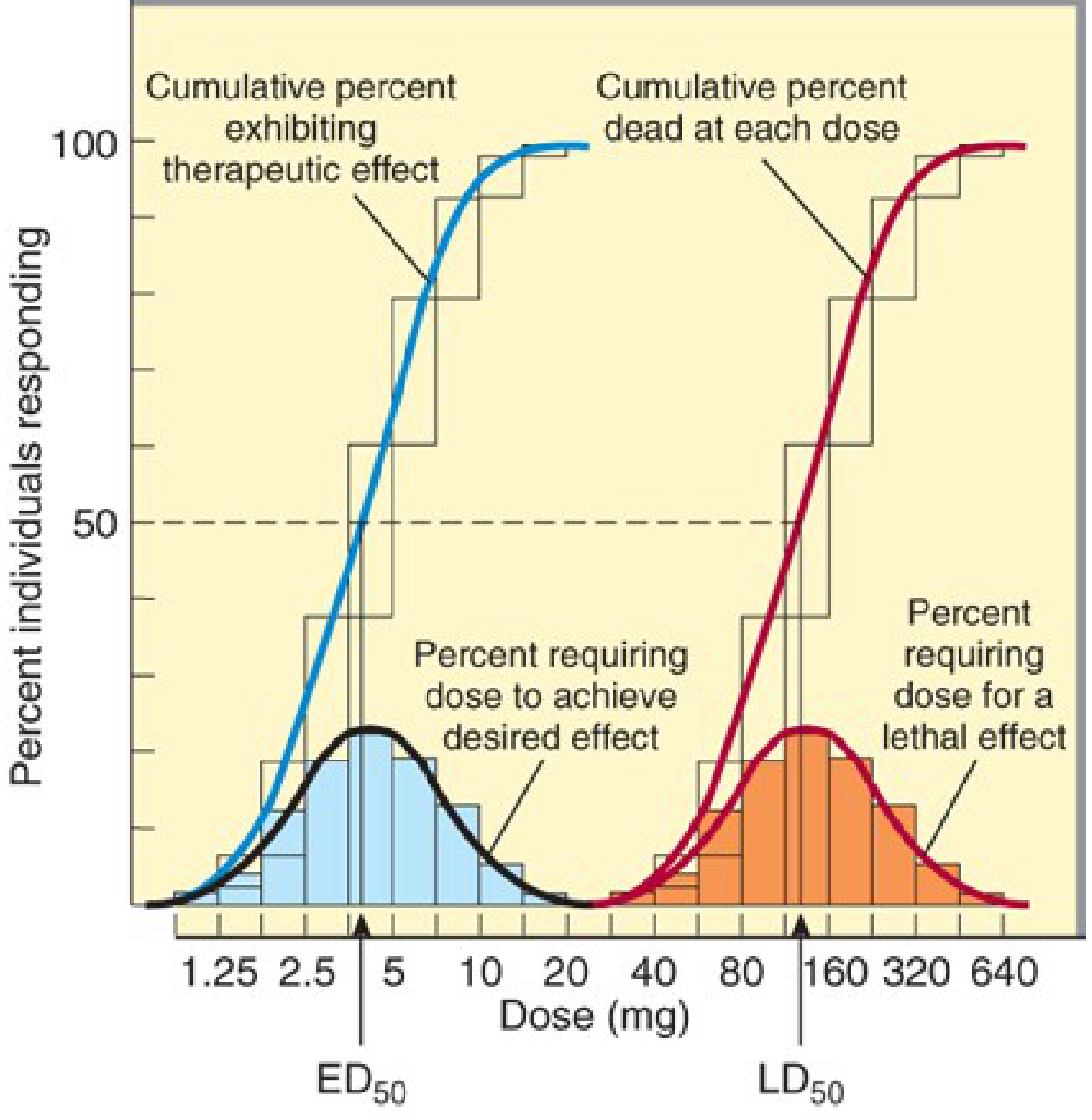
"If the ED50s of two drugs for producing a specified quantal effect are 5 and 500 mg respectively, then the first drug can be said to be 100 times more potent than the second for that particular effect."
- Katzung's Basic and Clinical Pharmacology, 16th Edition
Therapeutic Index - Potency and Safety
The therapeutic index (TI) is a related concept linking potency for benefit versus potency for harm:
Therapeutic Index = TD50 / ED50 (in animals) or LD50 / ED50
- A high TI = wide margin between therapeutic and toxic doses = safer drug
- A low TI = narrow therapeutic window = requires careful dose monitoring (e.g., warfarin, digoxin, lithium)
The range between the minimum toxic dose and the minimum therapeutic dose is called the therapeutic window - the most practically useful concept for dosing individual patients.
Shape of the Dose-Response Curve
- Gentle slope: Drug concentration can vary considerably without large changes in effect - easier to manage clinically
- Steep slope (e.g., Curve D in Katzung Figure 2-15): Small dose changes produce large effect changes - clinically dangerous if upper part of curve represents toxic effects (e.g., coma from a sedative-hypnotic)
Clinical Relevance of Potency
- Drug comparison: Potency is stated in dosage units for a specific endpoint (e.g., "50 mg for mild sedation")
- Relative potency: Ratio of equi-effective doses used to compare two drugs (e.g., Drug X is 10x more potent than Drug Y)
- Selectivity: Comparing ED50 values for two different effects of the same drug reveals selectivity (e.g., cough suppression vs. sedation for opioids)
- High potency is not always better: A highly potent but low-efficacy drug (partial agonist) may be unsuitable when a strong effect is needed
Sources: Katzung's Basic and Clinical Pharmacology, 16th Edition | Goodman & Gilman's The Pharmacological Basis of Therapeutics
Side effects, therapeutic effects, adverse effects in Pharmacology
Finding Sources
Searching the Web
therapeutic effects side effects adverse drug reactions pharmacology definitions types
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Excellent content gathered from multiple authoritative textbooks. Here is the comprehensive answer.
Side Effects, Therapeutic Effects & Adverse Effects in Pharmacology
1. Therapeutic Effects
Therapeutic effects are the intended, beneficial outcomes of drug administration - the reason the drug was prescribed in the first place.
Benefits of drug therapy fall into three broad categories:
| Category | Description | Example |
|---|---|---|
| Alleviation of symptoms | Relief of pain, fever, nausea, etc. | Paracetamol for headache |
| Prevention of progression/complications | Stopping disease from worsening | Antihypertensives preventing stroke |
| Prolonged life | Extending survival | Antiretrovirals in HIV, chemotherapy in cancer |
"It is self-evident that the benefits of drug therapy should outweigh the risks. Benefits fall into broad categories: alleviation of symptoms, prevention of disease progression or complications, and prolonged life."
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Establishing the exact balance between benefit and risk for an individual patient can be complex - drugs that provide symptomatic benefits but shorten life (e.g., in severe heart failure or cancer) may still be appropriate if chosen carefully.
2. Side Effects
Side effects are unintended drug effects that occur at normal therapeutic doses. They are an unavoidable risk of medication treatment. The term is widely used but somewhat imprecise - it generally refers to unintended effects within the therapeutic dose range that may or may not be harmful.
"Side effects are an unavoidable risk of medication treatment. Although it is impossible to have an encyclopedic knowledge of all possible adverse drug effects, prescribing clinicians should be familiar with the more common adverse effects, as well as those with serious medical consequences."
- Kaplan & Sadock's Synopsis of Psychiatry
How Side Effects Arise
Side effects arise through two main mechanisms:
a) Extensions of the drug's therapeutic mechanism
When the side effect is a direct consequence of the same pharmacological action that produces the therapeutic effect - these are often unavoidable:
| Drug/Class | Therapeutic Action | Side Effect from Same Mechanism |
|---|---|---|
| SSRIs (e.g., fluoxetine) | Serotonin reuptake inhibition | Nausea, sexual dysfunction |
| Antipsychotics | Dopamine D2 receptor blockade | Extrapyramidal side effects |
| Benzodiazepines | GABA-A receptor agonism | Sedation, ataxia |
b) Unrelated pharmacological properties
Side effects caused by receptor actions that have nothing to do with the intended use:
- Tricyclic antidepressants (TCAs) cause dry mouth, urinary retention, constipation - from muscarinic ACh receptor blockade (not related to antidepressant action)
- TCAs also cause sedation - from histamine H1 receptor blockade
Time Course of Side Effects
| Timing | Description | Examples |
|---|---|---|
| Early, time-limited | Appear at start, then fade | Nausea with SSRIs, sedation with mirtazapine |
| Early, persistent | Appear at start and stay | Dry mouth with noradrenergic drugs |
| Late-appearing | Only emerge over time | Weight gain with SSRIs (reversal of early weight loss) |
Severity of Side Effects
- Mild/tolerable: Dry mouth, nausea - may not require stopping therapy
- Serious/life-threatening (examples from psychiatry):
- Agranulocytosis - clozapine
- Stevens-Johnson syndrome - lamotrigine
- Hepatic failure - nefazodone
- Heart block - thioridazine
- Stroke - phenelzine (MAOI)
Drugs carrying serious risks carry a black box warning and require closer monitoring.
3. Adverse Drug Reactions (ADRs)
Adverse drug reactions (ADRs) are the broader, more formal clinical term for harmful, unintended drug responses.
The WHO/ICH definition (cited in StatPearls/NCBI):
"A response to a drug which is noxious and unintended, and which occurs at doses normally used for prophylaxis, diagnosis, or therapy of disease or the modification of physiologic function."
Key distinctions:
- An ADR has a causal connection to the drug
- An adverse drug event (ADE) is any untoward medical occurrence during treatment, but may not have a proven causal link to the drug
"Some adverse effects are so common and so readily associated with drug therapy that they are identified very early during clinical use of a drug. By contrast, serious ADRs may be sufficiently uncommon that they escape detection for many years after a drug begins to be widely used."
- Harrison's Principles of Internal Medicine, 22nd Edition
Epidemiological Impact
- 3-6% of hospital admissions in the USA are due to ADRs
- 2.5-10.6% of admissions in Europe are ADR-related
- Over 29 million ADRs were reported in the USA through the FDA Adverse Events Reporting System (FAERS) from 2011-2024
4. The Therapeutic Ratio: Where They All Meet
The relationship between therapeutic effects and adverse effects is captured graphically by the therapeutic ratio (therapeutic index/therapeutic window):
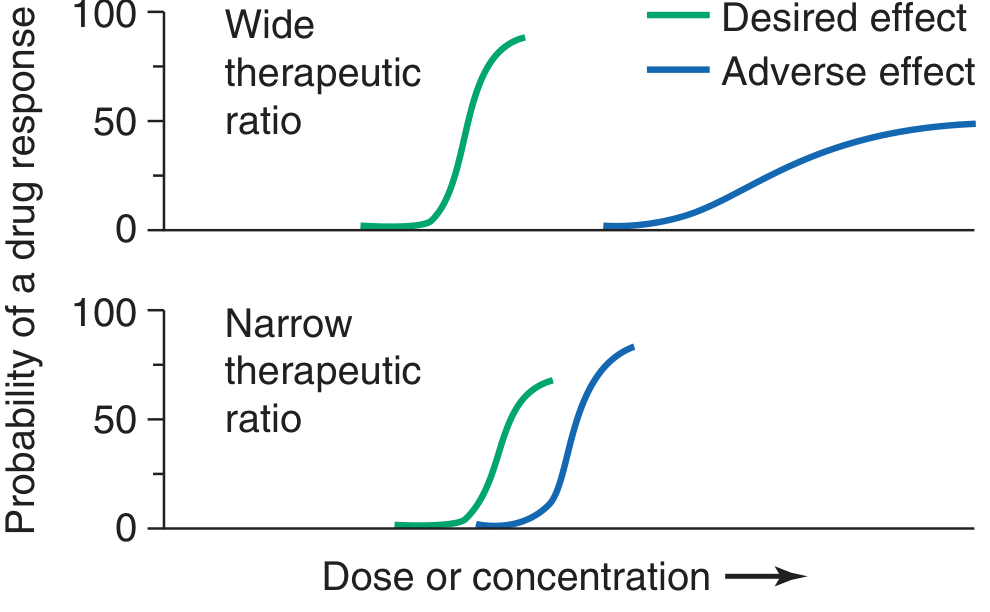
"A steep dose-response curve for adverse effects is especially undesirable, as it implies that even small dosage increments may sharply increase the likelihood of toxicity."
- Harrison's Principles of Internal Medicine, 22nd Edition
Drugs with narrow therapeutic windows (e.g., warfarin, digoxin, lithium, phenytoin) require therapeutic drug monitoring (TDM) to keep plasma levels within the safe therapeutic range.
5. Side Effects That Become Therapeutic Effects
An important concept: some side effects of one drug become the therapeutic rationale for using that drug in a different condition:
| Original Use | "Side Effect" | Now Used As |
|---|---|---|
| Antihistamine (diphenhydramine) | Sedation | Sleep aid |
| Minoxidil (antihypertensive) | Hair growth | Alopecia treatment |
| Sildenafil (pulmonary hypertension) | Penile erection | Erectile dysfunction (Viagra) |
| Thalidomide (sedative) | Anti-inflammatory | Multiple myeloma, erythema nodosum leprosum |
Summary Comparison
| Feature | Therapeutic Effect | Side Effect | Adverse Drug Reaction |
|---|---|---|---|
| Intent | Intended | Unintended | Unintended |
| Harm | Beneficial | May or may not be harmful | Harmful / noxious |
| Dose dependency | Yes | Usually yes | Not always (some are dose-independent) |
| Causal link to drug | Yes | Yes | Yes (by definition) |
| Reversibility | N/A | Usually reversible | Variable |
| Example | Aspirin relieves pain | Aspirin causes GI irritation | Aspirin causes GI bleeding (serious ADR) |
Sources: Harrison's Principles of Internal Medicine, 22nd Edition (2025) | Kaplan & Sadock's Synopsis of Psychiatry | Katzung's Basic and Clinical Pharmacology, 16th Edition | WHO/ICH ADR Definition via StatPearls/NCBI
This is a shared conversation. Sign in to Orris to start your own chat.