Dengue
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
dengue fever management guidelines
Searching the Web
dengue fever 2024 2025 WHO guidelines management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full response.
Dengue - Comprehensive Overview
Etiology
Dengue is caused by four antigenically distinct RNA flaviviruses: DENV-1, DENV-2, DENV-3, and DENV-4. All four are transmitted primarily by Aedes aegypti mosquitoes, and less commonly by Aedes albopictus and Aedes polynesiensis.
- Family: Flaviviridae; genus Flavivirus
- Single-stranded, positive-sense RNA virus
- Infection with one serotype confers lifelong immunity to that serotype and transient cross-protection (1-3 years) against the other three
- A person may have up to four lifetime dengue infections
- Sherris & Ryan's Medical Microbiology, 8th Ed.
Epidemiology
- Infects an estimated 400 million people per year, 100 million symptomatic, ~40,000 deaths from severe dengue
- Endemic in South and Central America, Mexico, Africa, Asia, the Caribbean, and Pacific islands
- In 2025, >3.6 million reported infections across nearly 100 countries
- Vector mosquitoes breed in peridomestic standing water; strongly associated with poor sanitation, crowding, and tropical climate
- Incubation period: 3-14 days (intrinsic); mosquito extrinsic incubation 8-12 days
- Viremic persons (symptomatic or asymptomatic) can infect mosquitoes 1-2 days before symptoms and throughout ~7-day viremia
- Red Book 2021; Robbins & Cotran Pathologic Basis of Disease
Pathophysiology
Primary Infection
Infection elicits serotype-specific neutralizing antibodies and cross-reactive non-neutralizing antibodies.
Antibody-Dependent Enhancement (ADE)
The key mechanism explaining severe disease on secondary infection:
- Cross-reactive antibodies from the first serotype cannot neutralize the second serotype
- Instead, these non-neutralizing IgG antibodies bind the new virus and facilitate entry into macrophages via Fc receptors, amplifying viral replication
- Higher viral load drives cytokine storm, endothelial dysfunction, and massive plasma leakage
- Severe dengue is most likely with secondary DENV-2 infection
- Same mechanism explains severe dengue in infants born to dengue-immune mothers (maternally acquired antibodies)
Plasma Leakage Mechanism
Endothelial dysfunction leads to increased vascular permeability → fluid shifts from intravascular to extravascular compartments → hemoconcentration, pleural effusion, ascites, and (if severe) hypovolemic shock.
- Robbins & Cotran, 10th Ed.; Harrison's Principles, 22nd Ed. (2025)
Clinical Phases
Dengue has three distinct phases:
Phase 1: Febrile Phase (Days 1-3)
- Abrupt high fever (39-40°C), lasting 2-7 days ("saddleback" pattern possible)
- Severe headache, retro-orbital pain, myalgia, arthralgia ("breakbone fever")
- Facial flushing, pharyngeal injection, conjunctival suffusion
- Macular or maculopapular rash
- Nausea/vomiting
- Petechiae, mild hemorrhagic manifestations
- Labs: leukopenia, thrombocytopenia beginning
Phase 2: Critical Phase (Days 3-7, around defervescence)
- Temperature drops - this is the danger window
- Plasma leakage due to increased vascular permeability (lasts 24-48 hours)
- Rising hematocrit (hemoconcentration) is a key marker
- Rapid drop in platelet count
- Warning signs (requiring hospitalization):
- Abdominal pain or tenderness
- Persistent vomiting
- Clinical fluid accumulation (ascites, pleural effusion)
- Mucosal bleeding
- Lethargy or restlessness
- Liver enlargement >2 cm
- Rising hematocrit with rapid platelet decline
Phase 3: Recovery/Convalescent Phase (Days 7-10+)
- Reabsorption of leaked fluids
- Risk of fluid overload if IV fluids not reduced
- Bradycardia, confluent rash with islets of normal skin ("white islands in a sea of red")
- Improving platelet count
- Red Book 2021; Park's Textbook of Preventive and Social Medicine
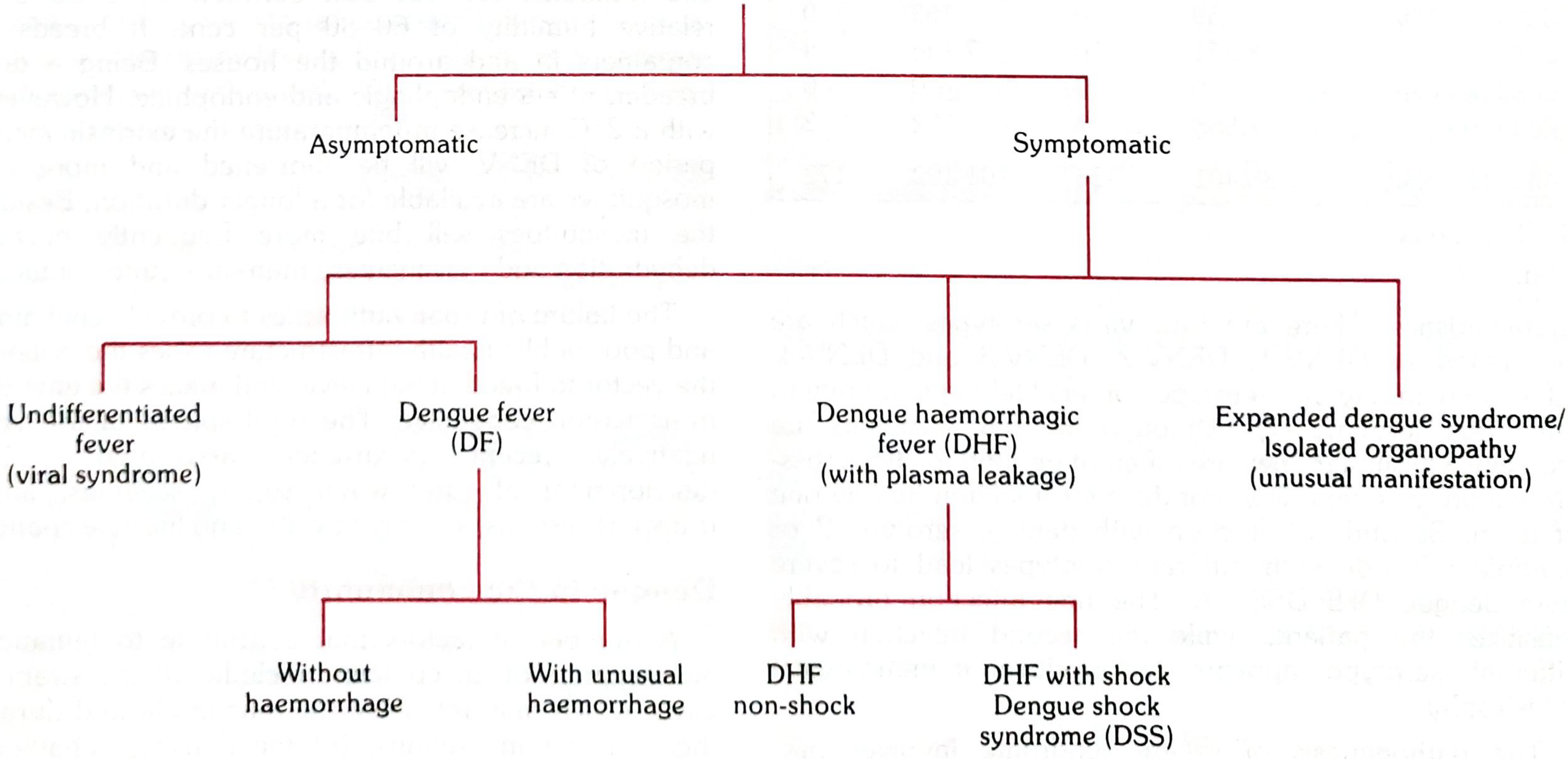
WHO Classification
2009 WHO Classification (Current)
| Category | Definition |
|---|---|
| Dengue without warning signs | Fever + ≥2 of: nausea/vomiting, rash, aches, leukopenia, positive tourniquet test |
| Dengue with warning signs | Above + any: abdominal pain, persistent vomiting, fluid accumulation, mucosal bleeding, lethargy, liver enlargement >2 cm |
| Severe dengue | Severe plasma leakage with shock or respiratory distress; severe bleeding; severe organ impairment (AST/ALT ≥1000 IU/L, impaired consciousness, heart failure, organ failure) |
Classical DHF Grading (WHO 1997 - Still Used)
| Grade | Features | Labs |
|---|---|---|
| DF | Fever + 2 symptoms; no plasma leakage | WBC ≤5000; platelets <150,000; Hct rise 5-10% |
| DHF I | DF + plasma leakage + positive tourniquet test | Platelets <100,000; Hct rise ≥20% |
| DHF II | Grade I + spontaneous bleeding (petechiae, epistaxis, GI bleed) | Platelets <100,000; Hct rise ≥20% |
| DHF III | Grade II + circulatory failure (weak rapid pulse, pulse pressure ≤20 mmHg, cold clammy skin, restlessness) | Same |
| DHF IV (DSS) | Profound shock, undetectable BP/pulse | Same |
DHF Grades III & IV = Dengue Shock Syndrome (DSS)
- Park's Textbook; Red Book 2021
Diagnosis
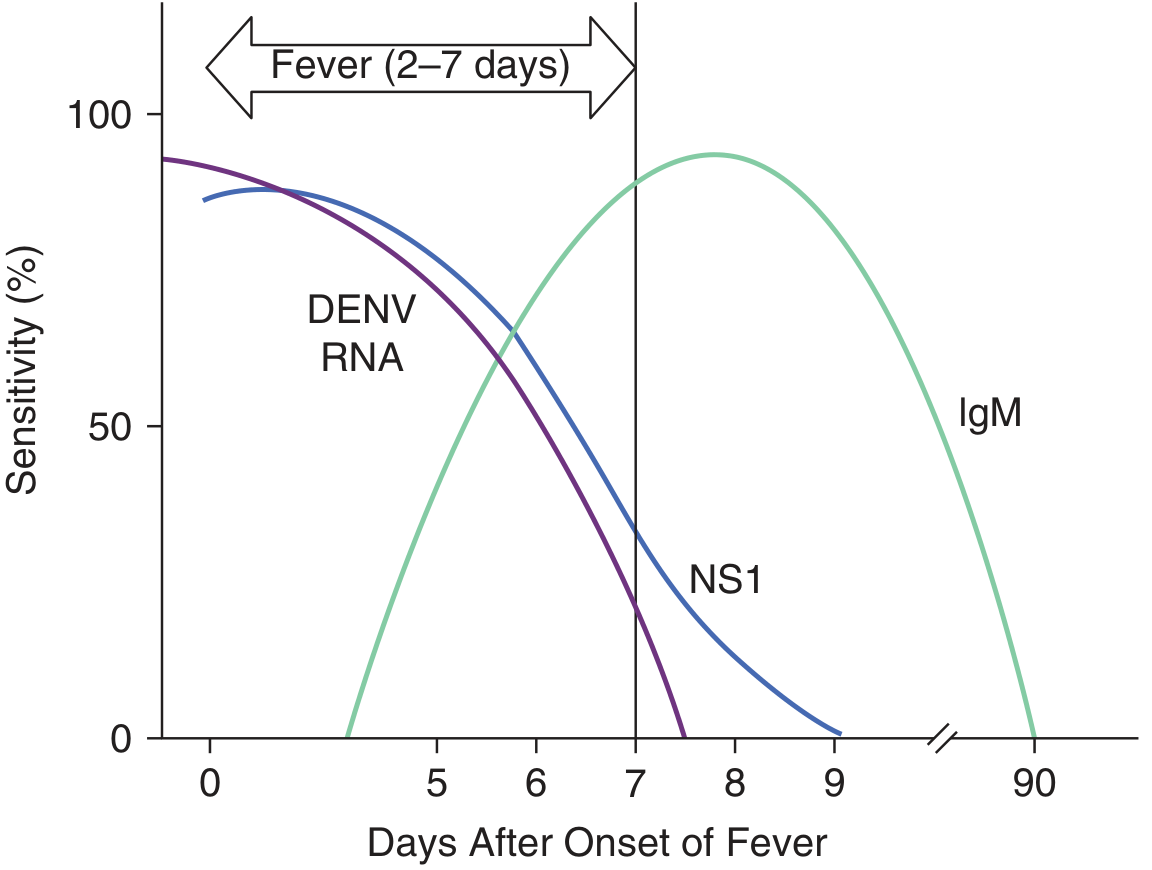
Timing-Based Approach
| Test | Window | Notes |
|---|---|---|
| RT-PCR | Days 1-7 (viremic phase) | Gold standard for early diagnosis |
| NS1 Antigen (ELISA or rapid) | Days 1-9 | Rapid tests available (minutes); less sensitive in secondary infection |
| IgM antibody (MAC-ELISA) | From Day 3-5 onwards; peaks ~2 weeks | Cross-reacts with Zika and other flaviviruses |
| IgG antibody | Secondary infection: rises sharply in acute phase | Lifelong persistence; a fourfold rise between acute and convalescent confirms recent infection |
- Testing a single specimen in the first 10 days for both NS1 antigen AND IgM detects ≥90% of cases
- RT-PCR or NS1: preferred in first 5 days
- IgM: preferred after Day 5
- FBC findings: leukopenia, thrombocytopenia, elevated hematocrit, raised liver enzymes
- Red Book 2021; Park's Textbook
Tourniquet (Rumpel-Leede) Test
Inflate BP cuff to midpoint between systolic and diastolic for 5 minutes. Positive = ≥10 petechiae per square inch (2.5 cm²) in the cubital fossa. Indicates increased capillary fragility.
Management
No specific antiviral exists. Treatment is entirely supportive.
Dengue without Warning Signs (Outpatient)
- Oral rehydration (ORS, fruit juices, electrolyte solutions)
- Paracetamol for fever (≥6-hour intervals); keep temp <39°C
- Avoid NSAIDs (ibuprofen), aspirin, corticosteroids - increase bleeding risk
- Return immediately if warning signs develop
- Monitor: daily FBC, hematocrit, platelet count, fluid balance
Dengue with Warning Signs (Hospital Admission)
- IV crystalloids (isotonic saline or Ringer's lactate)
- Titrate fluid rate based on clinical status and hematocrit
- Monitor urine output (target ≥0.5 mL/kg/hr)
- Watch for plasma reabsorption in convalescence - reduce fluids to avoid overload
Severe Dengue / DSS (ICU-Level Care)
- Aggressive IV fluid resuscitation - crystalloids first; colloids or blood products if refractory
- Monitoring: serial hematocrit, blood pressure, pulse, urine output
- Platelet transfusion: only for severe bleeding or pre-procedural, not prophylactic
- Vasopressors for refractory shock
- With early recognition and aggressive supportive care, CFR drops from 5-10% to <1%
- Red Book 2021; Park's Textbook; Brenner & Rector's The Kidney
Complications
| Complication | Notes |
|---|---|
| Dengue Shock Syndrome (DSS) | Grades III-IV DHF; most common cause of dengue death |
| Severe hemorrhage | GI bleed, hemoptysis, intracranial hemorrhage |
| Acute hepatitis / liver failure | AST/ALT >1000 IU/L |
| Myocarditis | Arrhythmia, heart failure |
| Acute encephalitis/meningoencephalitis | Direct viral invasion or immune-mediated |
| Post-dengue ADEM | Demyelinating; delayed |
| Hemophagocytic lymphohistiocytosis | Rare, severe |
| Acute kidney injury | Plasma leakage, hypoperfusion |
| Pancreatitis | Uncommon |
| Fluid overload | Iatrogenic, during convalescence |
- Red Book 2021
High-Risk Groups for Severe Disease
- Infants (maternal antibodies - ADE)
- Pregnant women
- Second (heterologous) dengue infection
- Patients with chronic diseases: asthma, sickle cell, diabetes mellitus
Vaccination
- Dengvaxia (CYD-TDV) - chimeric live-attenuated tetravalent vaccine; approved in several countries but only recommended for seropositive individuals - risk of severe dengue on first natural infection post-vaccination in seronegative recipients (paradoxically acts like a "first infection")
- TAK-003 (Qdenga) - live-attenuated tetravalent; approved in multiple countries; trial (TIDES) showed ~80% efficacy for symptomatic dengue and ~90% for hospitalization; can be given regardless of prior serostatus, though most benefit in seropositive
- WHO 2025 updated guidelines on arboviral disease management (including dengue) were published in July 2025, emphasizing against corticosteroid use in non-severe dengue (conditional recommendation, low certainty evidence)
Key Points Summary
| Feature | Detail |
|---|---|
| Virus | 4 serotypes of Flavivirus (DENV 1-4) |
| Vector | Aedes aegypti (primary) |
| Pathogenesis | ADE on secondary heterologous infection |
| Incubation | 3-14 days |
| Classic triad | Fever + retro-orbital headache + rash |
| Critical window | Defervescence (days 3-7) |
| Key marker | Rising hematocrit + falling platelets |
| Early test | RT-PCR / NS1 antigen (days 1-7) |
| Late test | IgM (from day 5) |
| Avoid | Aspirin, NSAIDs, corticosteroids |
| Treat | Supportive: fluids, paracetamol, monitoring |
| CFR (treated) | <1% |
2025 Note: WHO issued updated clinical management guidelines for dengue and other arboviral diseases in July 2025, recommending against corticosteroid use in non-severe dengue. In 2025, dengue surged globally with >3.6 million reported cases across ~100 countries - the highest burden in recent years.
Sources: Red Book 2021 (AAP); Harrison's Principles 22nd Ed. (2025); Robbins & Cotran Pathologic Basis of Disease, 10th Ed.; Park's Textbook of Preventive and Social Medicine; WHO arboviral guidelines 2025
Dengue virus in microbiology
Finding Sources
Searching the Web
dengue virus microbiology structure replication genome 2024
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I have everything needed for a thorough, microbiology-focused response. Let me compile the comprehensive answer now.
Dengue Virus - Microbiology
1. Classification & Taxonomy
| Property | Detail |
|---|---|
| Family | Flaviviridae |
| Genus | Flavivirus |
| Serotypes | 4 (DENV-1, DENV-2, DENV-3, DENV-4) |
| Genome | Single-stranded, positive-sense (+ssRNA) |
| Size | 40-60 nm in diameter |
| Envelope | Yes - lipid envelope with 2 glycoproteins |
Dengue virus was originally classified in the togavirus family as a "Group B arbovirus" but was reclassified into the distinct family Flaviviridae based on differences in viral genome organization. Other important members of Flaviviridae include Yellow fever virus, West Nile virus, Japanese encephalitis virus, Zika virus, and Hepatitis C virus (the last having no arthropod vector).
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.
2. Viral Structure
Dengue virus is a spherical, enveloped virus (40-60 nm):
- Lipid envelope - derived from host cell membrane during budding; contains two surface glycoproteins:
- Envelope (E) protein - the major surface glycoprotein; mediates receptor binding and membrane fusion; primary target for neutralizing antibodies; varies by 30-40% among the four serotypes - this divergence underlies non-neutralizing cross-reactive antibody formation
- Membrane (M) protein (mature form of prM) - present in mature virions; prM is the precursor form in immature virions
- Nucleocapsid - the E and M proteins surround an icosahedral nucleocapsid
- Capsid (C) protein - encloses the +ssRNA genome
Genome Organization
The ~11 kb positive-sense ssRNA genome encodes a single open reading frame (ORF) that is translated as one large polyprotein, which is then cleaved by host and viral proteases into 10 proteins:
3 Structural proteins:
| Protein | Function |
|---|---|
| C (Capsid) | Nucleocapsid formation; RNA packaging |
| prM/M (pre-Membrane/Membrane) | Chaperones E protein folding in ER; cleaved during maturation to yield M |
| E (Envelope) | Receptor binding (binds heparan sulfate, DC-SIGN, and other receptors); membrane fusion; major neutralization antigen; determines serotype specificity |
7 Non-structural (NS) proteins:
| Protein | Function |
|---|---|
| NS1 | Secreted glycoprotein; complement evasion; assists in RNA replication; target of IgM diagnostic tests |
| NS2A | Membrane rearrangement; replication complex scaffolding |
| NS2B | Cofactor for NS3 protease |
| NS3 | Bifunctional: serine protease (with NS2B cofactor) + RNA helicase/NTPase - processes polyprotein and unwinds RNA |
| NS4A | Membrane remodeling; induces autophagy |
| NS4B | Interferon antagonist; replication complex membrane anchor |
| NS5 | Largest NS protein; bifunctional: methyltransferase (5' RNA cap) + RNA-dependent RNA polymerase (RdRp) - the key enzyme driving genome replication |
- Goldman-Cecil Medicine International Edition; PMC (dengue pathogenesis review)
3. Replication Cycle
The dengue replication cycle occurs entirely in the cytoplasm of infected cells:
-
Attachment - E protein binds host cell receptors (heparan sulfate proteoglycans, DC-SIGN/CD209, TIM-1, AXL, etc.) on monocytes, macrophages, dendritic cells, and endothelial cells
-
Entry - Receptor-mediated endocytosis; the E protein undergoes acid-triggered conformational change in the endosome → membrane fusion → release of nucleocapsid into cytoplasm
-
Translation - Positive-sense RNA acts directly as mRNA → ribosomes on the rough ER translate the single polyprotein
-
Polyprotein processing - NS2B/NS3 protease (viral) + host signal peptidase cleave the polyprotein into the 10 individual proteins
-
RNA replication - NS proteins (particularly NS3 helicase + NS5 RdRp) assemble a replication complex on ER-derived membranes; the +ssRNA is copied to a -ssRNA intermediate, then to new +ssRNA genomes
-
Assembly - New +ssRNA genomes packaged with C protein to form nucleocapsids → bud into the lumen of the ER acquiring prM and E glycoproteins; produces immature virions
-
Maturation - In the trans-Golgi, low pH causes conformational change → host furin protease cleaves prM to M → produces mature infectious virions
-
Release - Exocytosis via secretory vesicles; mature virions released into the extracellular space
- Jawetz Medical Microbiology, 28th Ed.; Reactome (dengue replication complex)
4. Antigenic Properties & Serotypes
- Four serotypes exist: DENV-1, DENV-2, DENV-3, DENV-4
- Distinguished by neutralization tests and molecular assays (RT-PCR serotyping)
- The envelope (E) protein diverges by 30-40% between serotypes - sufficient to prevent cross-neutralization
- All four serotypes are antigenically related (cross-reactive IgG) but require distinct serotype-specific antibodies for neutralization
- DENV-2 is most commonly associated with severe dengue disease
- Goldman-Cecil Medicine; Jawetz Medical Microbiology
5. Immune Response & Antibody-Dependent Enhancement (ADE)
Primary Infection
- Stimulates serotype-specific neutralizing antibodies (lifelong protection against that serotype)
- Also stimulates cross-reactive, non-neutralizing IgG against other serotypes
- Cross-protection against other serotypes lasts 1-3 years only
Secondary Infection (Different Serotype)
This is the mechanistic basis of severe dengue:
- Pre-existing non-neutralizing cross-reactive antibodies from the first infection bind the new serotype
- These sub-neutralizing antibody-virus complexes enter Fc receptor-bearing cells (monocytes, macrophages, dendritic cells) at dramatically higher rates than viral entry without antibody
- This ADE results in:
- Higher viral load in mononuclear phagocytes
- Massive release of cytokines and vasoactive mediators (TNF-α, IL-6, IL-10)
- Activation of procoagulants → DIC component
- Endothelial dysfunction → plasma leakage
- Cross-reactive CD4+ and CD8+ T cells (original antigenic sin) may also amplify immunopathology in secondary infection
The same mechanism explains severe dengue in infants of dengue-immune mothers - maternally acquired IgG mediates ADE upon their first natural infection.
- Jawetz Medical Microbiology; Goldman-Cecil Medicine
6. Vector Biology
| Feature | Detail |
|---|---|
| Primary vector | Aedes aegypti (domestic, daytime-biting) |
| Secondary vectors | Aedes albopictus, Aedes polynesiensis |
| Transmission | Female mosquito feeds on viremic human → virus replicates in mosquito midgut → travels to salivary glands |
| Extrinsic incubation | 8-14 days (in mosquito) |
| Infectivity | Mosquito remains infectious for life (1-3 months) |
| Breeding | Stagnant fresh water (containers, tires, flower pots, tree holes) near human dwellings |
| Activity | Daytime biting; urban/peridomestic |
A. albopictus differs importantly from A. aegypti: it can overwinter in temperate climates, increasing the geographic range of dengue risk. It was first detected in Texas in 1985 and spread throughout the southeastern United States by 1989.
- Jawetz Medical Microbiology, 28th Ed.
7. Laboratory Diagnosis (Microbiology Perspective)
Specimen: Acute-phase serum
| Method | Detects | Window | Notes |
|---|---|---|---|
| RT-PCR | DENV RNA | Days 1-7 (viremic phase) | Gold standard for early diagnosis AND serotyping; most specific |
| NS1 Antigen ELISA | NS1 glycoprotein | Days 1-9 | High sensitivity early; rapid tests available (minutes); sensitivity reduced in secondary infection |
| NS1 Rapid Test | NS1 glycoprotein | Days 1-9 | Bedside; minutes |
| IgM ELISA (MAC-ELISA) | Anti-dengue IgM | From Day 3-5; peaks ~2 weeks; detectable up to 3 months | Cross-reacts with Zika, WNV, JEV, YFV |
| IgG ELISA / HI test | Anti-dengue IgG | Lifelong; rapidly high in secondary infection | 4-fold rise in paired sera = active infection |
| Viral isolation | Live virus | Days 1-7 | Inoculation of mosquito cell lines (C6/36); slow (1 week+); rarely used clinically |
| Plaque reduction neutralization test (PRNT) | Serotype-specific antibodies | Convalescent | Gold standard serology; labor-intensive; used for confirmation and serotyping |
Key Diagnostic Principle
- Days 1-7: RT-PCR + NS1 antigen (combined gives ≥90% sensitivity for primary + secondary cases)
- After Day 5: IgM ELISA becomes the preferred test
- Serologic cross-reactivity with other flaviviruses (Zika, WNV, JEV, YFV, and vaccines) complicates IgG/IgM interpretation - always correlate with travel and vaccination history
- Jawetz Medical Microbiology, 28th Ed.; Goldman-Cecil Medicine; Red Book 2021
8. Manifestations of Dengue Virus Infection (Classification Tree)
9. Immunity & Infection Ratios
- Ratio of inapparent to apparent infections: approximately 15:1 in primary infections; lower in secondary infections (more symptomatic)
- Approximately 75% of dengue infections are asymptomatic
- Risk of DHF: ~0.2% in primary infection; at least 10-fold higher in secondary infection with a different serotype
- CFR of DHF/DSS: up to 15% untreated; <1% with proper fluid management
- Jawetz Medical Microbiology, 28th Ed.
10. Inactivation & Physical Properties
Like all flaviviruses, dengue virus is inactivated by:
- Acid pH
- Heat
- Lipid solvents (ether, chloroform)
- Detergents
- Bleach
- Phenol
- 70% alcohol
- Formaldehyde
Many flaviviruses (including dengue) exhibit hemagglutinating ability - used in the hemagglutination inhibition (HI) test for serology.
11. Quick Microbiology Summary Card
| Feature | Dengue Virus |
|---|---|
| Family | Flaviviridae |
| Genome | +ssRNA, ~11 kb, single ORF |
| Size | 40-60 nm |
| Envelope | Yes (E + M glycoproteins) |
| Serotypes | 4 (DENV 1-4) |
| Vector | Aedes aegypti (primary) |
| Key structural protein | E (envelope) - serotype specificity + neutralization target |
| Key NS proteins | NS3 (protease + helicase), NS5 (RdRp + methyltransferase), NS1 (diagnostic target) |
| Replication site | Cytoplasm (ER-derived membranes) |
| Maturation | prM → M cleavage by furin in trans-Golgi |
| Pathogenesis mechanism | Antibody-dependent enhancement (ADE) |
| Early diagnostic test | RT-PCR / NS1 Ag (days 1-7) |
| Late diagnostic test | IgM ELISA (from day 5) |
| Serology pitfall | Cross-reactivity with other flaviviruses |
Sources: Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed. | Goldman-Cecil Medicine | Sherris & Ryan's Medical Microbiology, 8th Ed. | Red Book 2021 | Park's Textbook of Preventive and Social Medicine
This is a shared conversation. Sign in to Orris to start your own chat.