
image.jpg
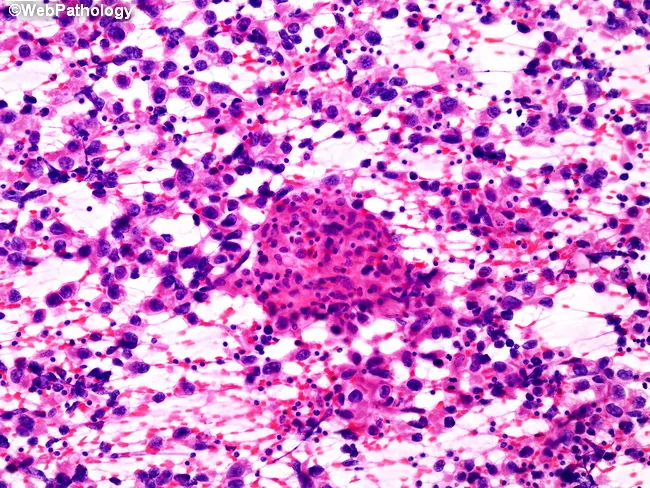
This is fnac smear of lesion (soft to firm, immobile, non tender at a pole of testes with nodeule over scrotum.
Reading File
Finding Sources
Finding Sources
Searching PubMed
testicular FNAC cytology diagnosis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
testicular seminoma FNAC cytology smear
Finding Sources
Loading Image
Reading File
Loading Image
Based on the FNAC smear image and the clinical details, here is a comprehensive cytopathological analysis:
FNAC Smear Interpretation — Testicular / Paratesticular Lesion
Clinical Summary
- Soft to firm, immobile, non-tender mass at a pole of the testis with a nodule over the scrotum
- Stain: H&E, 20× magnification
Cytomorphological Findings on the Smear
Looking at the image carefully:
-
Dense cellular aggregate (lower left) — a large, tightly cohesive cluster of cells with:
- Hyperchromatic, closely-packed nuclei
- High nuclear-to-cytoplasmic ratio
- Ill-defined cell borders within the cluster
- Darkly staining, consistent with malignant epithelial/germ cell proliferation
-
Dispersed cells in the background (right half) — scattered discohesive cells with:
- Large round-to-oval nuclei with prominent nucleoli
- Pale to clear cytoplasm (some with "fried egg" appearance)
- A prominent lymphocytic background — numerous small dark lymphocytes scattered throughout
-
No obvious necrosis, no giant cells visible at this magnification
-
The combination of large cells with pale/clear cytoplasm + lymphocyte-rich background + discohesive pattern is the hallmark of SEMINOMA on cytology
Most Likely Cytological Diagnosis
SEMINOMA (Classic)
This is the most consistent interpretation, supported by:
| Feature | Present in Smear | Seminoma Hallmark |
|---|---|---|
| Large polygonal cells, clear/pale cytoplasm | ✅ (dispersed background cells) | Classic |
| Prominent nucleoli | ✅ | Classic |
| Dense lymphocytic background | ✅ | Classic |
| Cohesive tumor cell clusters | ✅ | Seen in aspirates |
| Single-file discohesive cells | ✅ | Classic FNAC pattern |
Comparison image — touch imprint cytology of seminoma with granulomatous reaction (note similar large pale cells + lymphocyte-rich background):
Differential Diagnosis
| Diagnosis | For | Against |
|---|---|---|
| Seminoma | Large pale cells, lymphocytes, pole of testis, 40–50y peak | — |
| Embryonal carcinoma | Malignant cells | Cells more pleomorphic, papillary; no lymphocytes |
| Spermatocytic tumor | Testicular, older age | Triphasic cell pattern (small/medium/large); NO lymphocytes |
| Lymphoma | Lymphocytes abundant | Would show pure lymphoid infiltrate, no large germ cells |
| Granulomatous orchitis | Non-tender | No epithelioid granulomas or necrosis seen here |
| Metastatic carcinoma | Rare | Glandular/squamoid features expected |
Pathological Context (Robbins)
"Seminoma: Sheets of uniform polygonal cells with clear cytoplasm; lymphocytes in the stroma. Peak age 40–50 years." — Robbins & Kumar Basic Pathology
Seminoma accounts for 40–50% of all testicular germ cell tumors and is the most common single histologic type. It is exquisitely radiosensitive with an excellent prognosis when confined to the testis. 10% have elevated β-hCG; AFP is not elevated (AFP elevation points to non-seminomatous GCT).
Recommended Next Steps
- Radical inguinal orchiectomy — the definitive diagnostic AND therapeutic first step (transscrotal biopsy is contraindicated as it alters lymphatic drainage)
- Tumor markers: β-hCG, AFP, LDH
- CT abdomen/pelvis — staging (retroperitoneal lymph nodes)
- Histopathology of the orchiectomy specimen for definitive classification
- Immunohistochemistry if needed: PLAP, OCT3/4, CD117 (c-Kit) positive in seminoma; AFP/CD30 negative
⚠️ Important: FNAC of testicular masses is generally not recommended as a routine diagnostic step per most guidelines (risk of seeding, altered staging). The smear here is being interpreted in context of the clinical question. Radical inguinal orchiectomy remains the standard initial approach.
Recent evidence: A 2024 systematic review (PMID 39295546) on FNAC in paratesticular neoplasms confirms FNAC has a role in paratesticular (extratesticular) lesions — notably the scrotal nodule component — where cytology can guide management without the seeding risk associated with intra-testicular aspiration.
This is a shared conversation. Sign in to Orris to start your own chat.