Intertrochanteric fracture documentation as in orthopedic exam
Reading File
Finding Sources
Searching the Web
intertrochanteric fracture orthopedic examination documentation clinical findings
Searching PubMed
"intertrochanteric fracture" classification management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content from Campbell's Operative Orthopaedics 15th ed (2026), Rockwood & Green's 10th ed (2025), Tintinalli's, Rosen's, Pfenninger's, and Gray's Anatomy. I have enough to write a thorough orthopedic exam documentation. Let me compile the complete answer:
Intertrochanteric Fracture - Orthopedic Examination Documentation
Definition and Anatomy
An intertrochanteric fracture is an extracapsular, extra-articular fracture of the proximal femur occurring along a line between the greater and lesser trochanters. Because the fracture line extends through cancellous bone with an ample blood supply, avascular necrosis of the femoral head is uncommon - in contrast to intracapsular femoral neck fractures. The femoral neck and its blood supply are preserved.
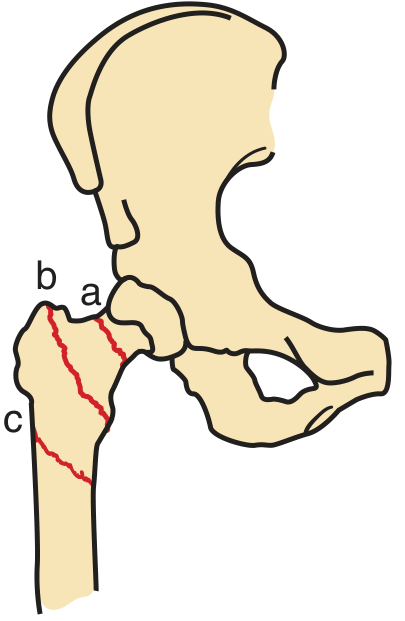
Fractures of the proximal femur: Neck (a); intertrochanteric (b); subtrochanteric (c). - Pfenninger & Fowler's Procedures for Primary Care
Patient Identification
| Field | Detail |
|---|---|
| Name | |
| Age / DOB | |
| Sex | |
| Side affected | Right / Left |
| Date of injury | |
| Mechanism of injury | |
| Date of examination | |
| Examiner |
History
Chief Complaint: Hip pain and inability to bear weight following [fall / trauma].
Mechanism of Injury:
- Low-energy fall (most common in elderly): tripping over carpet, pet, or step; slipping on floor
- High-energy trauma: motor vehicle accident (younger patients)
- Pathologic: consider if isolated lesser trochanter fracture in adult (commonly a malignant deposit)
Onset: Acute
Associated Symptoms:
- Pain: localized to the hip/groin/proximal thigh, worsened with any movement
- Inability to ambulate / bear weight
- Visible deformity of lower extremity
Relevant History:
- Prior hip fractures or falls
- Osteoporosis / osteopenia (DEXA T-score: _____)
- Medications: bisphosphonates, corticosteroids, diuretics (chronic diuretic use contributes to dehydration)
- Nutritional status / decreased oral intake
- Functional baseline: ambulatory status before injury (community ambulator / indoor ambulator / non-ambulator)
- Comorbidities: ASA classification (ASA III-IV increases mortality)
- Nursing home or institutionalized patient?
Physical Examination
General
- Patient appears in distress / comfortable
- Supine on stretcher / gurney
Inspection
- Limb position: The affected lower extremity is characteristically shortened and externally rotated (the strong action of the iliopsoas muscle on the lesser trochanter, and the short external rotators attached to the distal fragment, produce this deformity)
- Shortening: Clinically apparent limb length discrepancy
- Swelling / bruising over the lateral hip and proximal thigh
- Skin integrity: Abrasions, lacerations at the site of impact
Palpation
- Point tenderness: Over the intertrochanteric region / greater trochanter
- Crepitus: May be elicited on passive motion (use carefully)
- Pulse assessment: Dorsalis pedis and posterior tibial pulses (document if present/intact)
- Compartment assessment: Tense thigh compartment is rare but should be noted
Range of Motion (ROM)
- Active ROM: Markedly limited / absent due to pain
- Passive ROM: Painful with any movement of the hip - do not force motion
- Log-roll test: external/internal rotation of the leg in extension - painful
- Axial load / impact test: Gentle axial load through heel causes hip pain (positive in fracture)
Neurovascular Assessment
- Sensation: intact / impaired over the distribution of the femoral, obturator, sciatic nerves
- Motor: document distal motor function (ankle dorsiflexion, plantarflexion, EHL)
- Vascular: capillary refill, pedal pulses
Skin and Soft Tissue
- Pressure areas / existing skin breakdown (important pre-operatively)
- Pre-existing deformity or scarring from previous surgery
Limb Length Assessment
| Measurement | Right | Left |
|---|---|---|
| Apparent leg length (umbilicus to medial malleolus) | ||
| True leg length (ASIS to medial malleolus) | ||
| Shortening documented |
Classification
AO/OTA Classification (Current Standard)
The AO/OTA classification is the most useful and widely adopted system, incorporated into national hip fracture guidelines in Europe and the United States. The three main groups have acceptable intra- and interobserver variation; the subdivisions are less reliable.
| Type | Description | Stability |
|---|---|---|
| 31-A1 | Simple 2-part fracture; single fracture line extending medially; lateral wall intact | Relatively stable |
| 31-A2 | Comminuted fracture; increasing comminution; separate lesser trochanter fragment (3-4 parts); lateral wall essentially intact | More unstable |
| 31-A3 | Reverse obliquity, transverse, or subtrochanteric extension; lateral wall compromised; fracture line from lesser trochanter to lateral cortex | Most unstable |
A3 note: The reverse oblique fracture line may extend into the subtrochanteric region. CT or traction-table fluoroscopy may be needed to recognize this pattern. This type is the most challenging to treat.
Boyd and Griffin Classification (Historical)
| Type | Description |
|---|---|
| Type 1 | Fractures along the intertrochanteric line |
| Type 2 | Comminuted with main fracture line along intertrochanteric line; multiple secondary lines including possible coronal line on lateral view |
| Type 3 | Extends to or distal to the lesser trochanter |
| Type 4 | Fractures in the trochanteric region and proximal shaft; fractures in at least two planes |
Stability Assessment
- Stable: Intact posteromedial cortex; 2-part pattern (A1); lateral wall intact
- Unstable: Comminuted, reverse oblique, loss of lateral wall, subtrochanteric extension (A2, A3)
Imaging
Plain Radiographs (First-Line)
- AP pelvis and hip (bilateral for comparison)
- Lateral hip (cross-table lateral preferred to avoid moving the limb)
- Assess: fracture line direction, displacement, comminution, number of fragments, lesser trochanter involvement, lateral wall integrity, subtrochanteric extension
Additional Imaging
- CT scan: For operative planning; better assessment of lateral wall morphology; evaluation of occult or comminuted patterns; identifies A3-type fractures
- MRI: Preferred for occult fractures (nearly 100% sensitive); indicated when pain is severe, weight-bearing is impossible, but plain films are negative. Protocol: AP T1 + STIR sequences. Also identifies pathologic lesions, bone cysts, metastasis
- Bone scan: Alternative if MRI unavailable and pain/non-weight-bearing persists despite normal X-rays
Important note from Grainger & Allison's Radiology: Approximately 1% of fractures are initially occult on plain radiographs. If weight-bearing remains limited at 24 hours with no fracture on X-ray, further investigation is mandatory. Air trapped in a skin crease may mimic or mask a fracture.

Comminuted intertrochanteric fracture on the left - Grainger & Allison's Diagnostic Radiology
Documentation of Fracture Characteristics (Operative Planning Checklist)
| Feature | Finding |
|---|---|
| Side | Right / Left |
| Displaced / Non-displaced | |
| Stable / Unstable | |
| Number of fragments | 2-part / 3-part / 4-part / comminuted |
| Lesser trochanter attached / detached | |
| Lateral wall: intact / compromised | |
| Posteromedial cortex: intact / disrupted | |
| Reverse obliquity component | Yes / No |
| Subtrochanteric extension | Yes / No |
| Pathologic features | Yes / No (if yes, biopsy before fixation) |
| Associated fractures |
Associated Injuries
Intertrochanteric fractures are frequently associated with other distant fractures from the same fall that may be overlooked because the femoral fracture distracts attention. Always evaluate:
- Distal radius fracture
- Proximal humerus fracture
- Rib fractures
- Lumbar and thoracic spine fractures
Management Summary
Operative (Indicated in Nearly All Ambulatory Patients)
- Brings rapid mobilization, decreased hospital stay, reduced mortality, improved function
- Timing: urgent, not emergent - patient should be fully resuscitated first
- Early surgery within 24-48 hours improves 1-year mortality; operating on the day of injury (without resuscitation) increases mortality risk
Surgical Options by Fracture Type:
| Fracture Type | Preferred Fixation |
|---|---|
| Stable (31-A1) | Dynamic hip screw (DHS) / sliding screw-side plate |
| Unstable (31-A2, A3) | Cephalomedullary intramedullary nail (short or long, depending on subtrochanteric extension) |
| Non-ambulatory/poor surgical candidate | Non-operative: Buck's traction (pain relief); mobilize to sitting in 2-3 days |
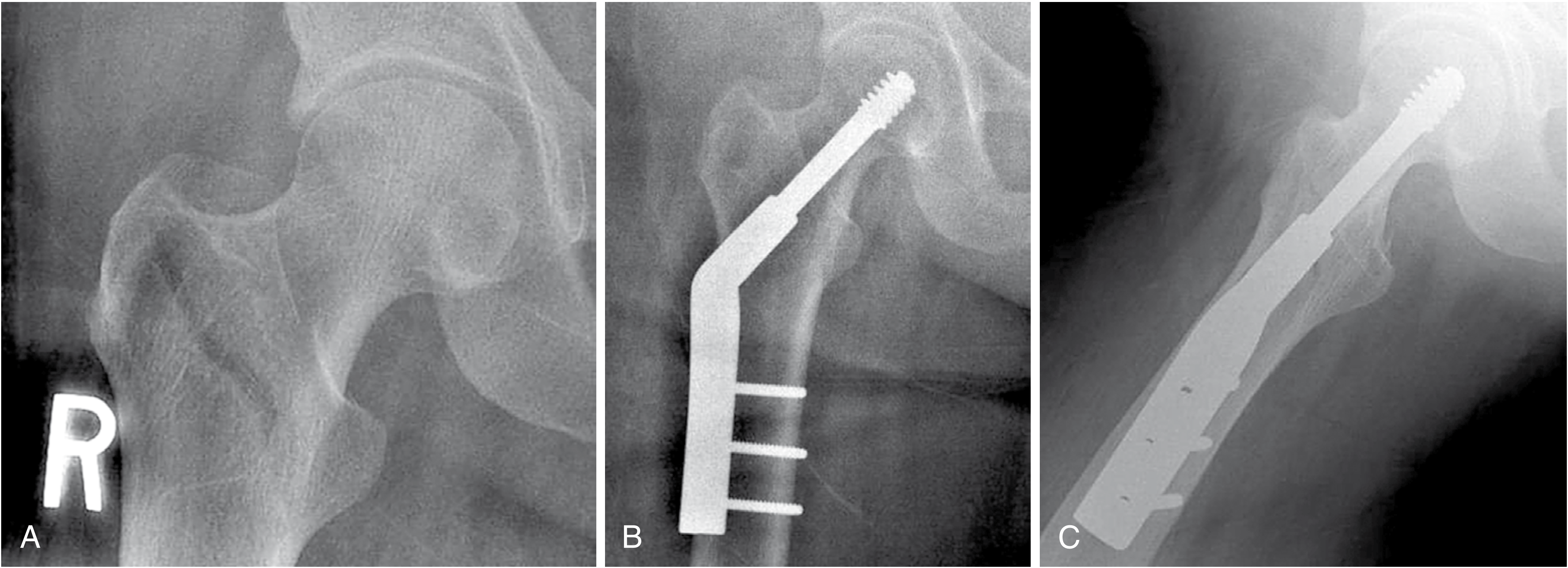
Fixation of intertrochanteric fracture: (A) Preoperative AP, (B) After DHS fixation, (C) Lateral view after fixation - Campbell's Operative Orthopaedics 15th Ed 2026
Non-Operative (Selected Cases)
- Non-ambulatory patients (e.g., nursing home residents) where pain control can be achieved without surgery
- Buck's traction intermittently for pain relief
- Mobilize to sitting within 2-3 days
Caution: Even non-displaced intertrochanteric fractures are at high risk for displacement with minor activities such as rolling in bed. Traction of any form is contraindicated as a definitive treatment for fracture reduction.
Complications and Prognosis
| Complication | Notes |
|---|---|
| Mortality | 20-30% at 1 year; males > females; age >85, ASA III-IV, ≥2 comorbidities increase risk |
| DVT / PE | Prophylaxis mandatory (all patients at bed rest) |
| Implant failure / cut-out | More common in unstable fractures, poor reduction (tip-apex distance >25 mm is a risk factor) |
| Nonunion | Uncommon; more common with inadequate reduction |
| Avascular necrosis | Uncommon (extracapsular fracture; blood supply preserved) |
| Infection | Post-surgical risk |
| Blood loss | Significant; crystalloid/transfusion may be required |
| Functional outcome | Approximately 50% regain pre-injury ambulatory level |
Secondary fracture prevention: Yearly zoledronic acid infusion starting within 90 days of repair reduces new fractures and decreases overall mortality.
ICD-10-CM Coding Reference
| Code | Description |
|---|---|
| S72.141A | Displaced intertrochanteric fracture, right femur, initial encounter |
| S72.142A | Displaced intertrochanteric fracture, left femur, initial encounter |
| S72.143A | Displaced intertrochanteric fracture, unspecified femur, initial encounter |
| S72.141D | Subsequent encounter, routine healing |
| S72.141K | Subsequent encounter, nonunion |
| S72.141G | Subsequent encounter, delayed healing |
Always specify: displaced vs. non-displaced, laterality, and encounter type.
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapter 60 - Intertrochanteric Femoral Fractures
- Rockwood and Green's Fractures in Adults 10th Ed 2025, Chapter 54 - Trochanteric Hip Fractures
- Tintinalli's Emergency Medicine, Chapter 273 - Intertrochanteric Fractures
- Rosen's Emergency Medicine, Chapter 47 - Intertrochanteric Fractures
- Pfenninger & Fowler's Procedures for Primary Care, 3rd Ed - Intertrochanteric Femur Fracture
- Gray's Anatomy for Students - Intertrochanteric Fractures
- Grainger & Allison's Diagnostic Radiology - Intertrochanteric and Subtrochanteric Fractures
This is a shared conversation. Sign in to Orris to start your own chat.