A 68 yrs old patient with a history of 30 yrs of smoking complains of severe cough and sob. What are the test required
Reading File
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent — I now have comprehensive, textbook-backed content. Let me compile the full answer.
Investigations for a 68-Year-Old Smoker with Severe Cough & Shortness of Breath
Given the clinical profile — 68 years old, 30 pack-year smoking history, severe cough, and shortness of breath (SOB) — the top differential diagnoses are:
- COPD (most likely)
- Lung cancer (must not miss in a heavy smoker)
- Heart failure (can mimic COPD)
- Pulmonary hypertension
- Pulmonary embolism / Interstitial lung disease (must exclude)
A structured, layered investigation approach is required:
1. Pulmonary Function Tests (PFTs) — Cornerstone
| Test | What it Detects |
|---|---|
| Spirometry (FEV₁/FVC ratio) | Obstructive pattern — ratio <0.7 confirms COPD |
| Post-bronchodilator FEV₁ | Grades COPD severity (mild ≥80%, moderate 50–79%, severe 30–49%, very severe <30%) |
| Diffusing Capacity (DLCO) | Reduced in emphysema, interstitial lung disease |
| Inspiratory/Expiratory pressures | Assesses respiratory muscle weakness |
Spirometry with a post-bronchodilator FEV₁/FVC <0.7 is required to confirm COPD. The FEV₁ percentage of predicted then grades severity. — Tintinalli's Emergency Medicine, p. 509
2. Chest Imaging
| Test | Findings |
|---|---|
| Chest X-ray (PA view) | Hyperinflation, flattened diaphragms, bullous changes (emphysema); masses/nodules (lung cancer); cardiomegaly/pleural effusion (heart failure) |
| High-Resolution CT Chest (HRCT) | Emphysematous changes not visible on X-ray; lung masses; interstitial lung disease; lymphadenopathy; pulmonary embolism (with CT-PA) |
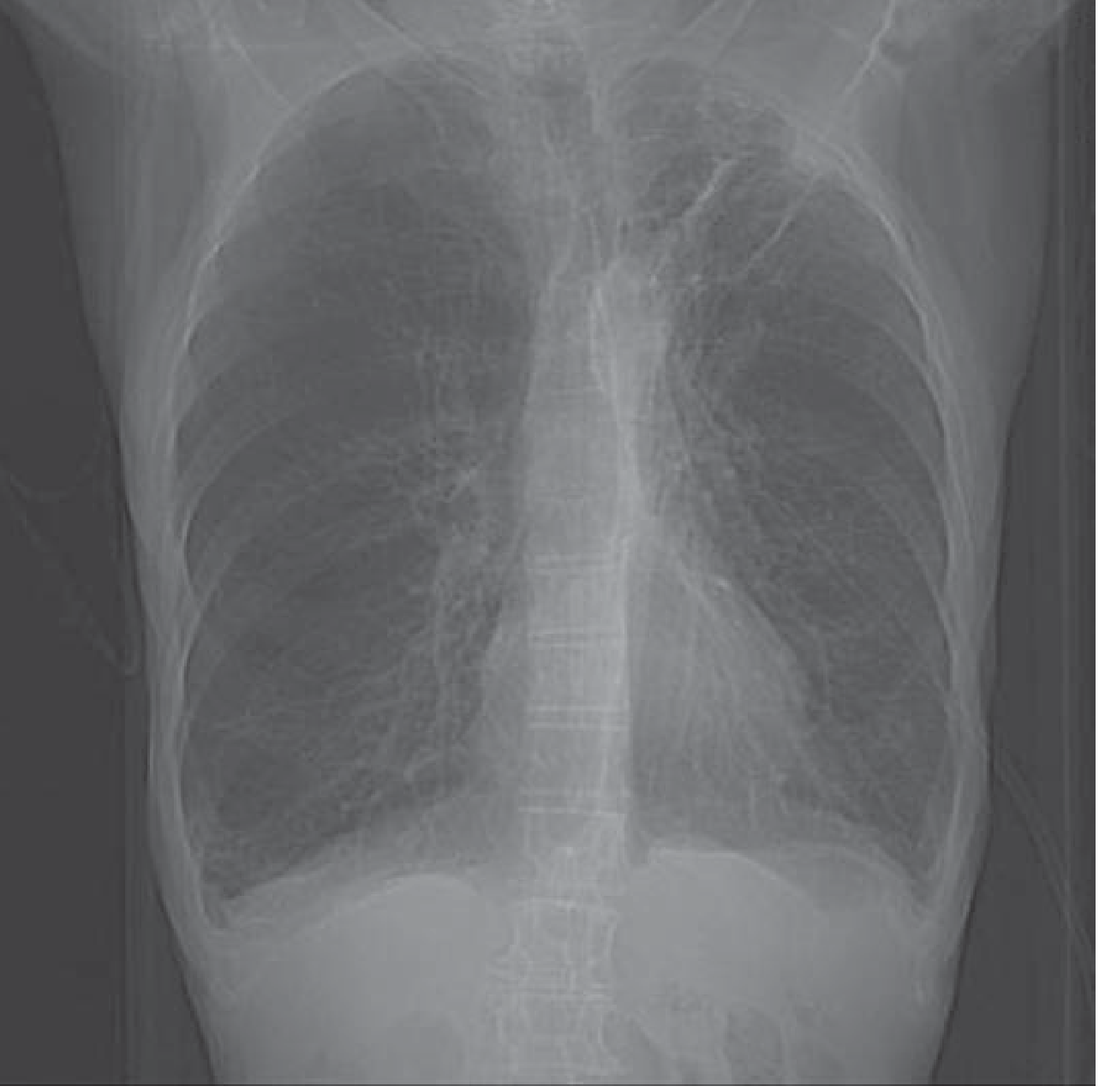
A plain chest radiograph is useful in demonstrating changes suggestive of COPD (hyperinflation, bullous changes). CT of the chest may reveal emphysema or an interstitial process not suggested by plain radiographs. — Fishman's Pulmonary Diseases and Disorders, p. 439
3. Arterial Blood Gas (ABG)
- Detects hypoxemia (PaO₂ ↓) and hypercapnia (PaCO₂ ↑)
- In early COPD: mild to moderate hypoxemia without hypercapnia
- In advanced COPD: progressive hypercapnia and respiratory acidosis
- Guides need for oxygen therapy: criterion = PaO₂ ≤55 mmHg or SaO₂ ≤88%
4. Blood Tests
| Test | Purpose |
|---|---|
| CBC (Full Blood Count) | Polycythemia (secondary to chronic hypoxia); anemia; infection (elevated WBC) |
| CRP / ESR | Acute exacerbation or infection |
| BNP / NT-proBNP | BNP <100 pg/mL supports COPD; >500 pg/mL suggests heart failure |
| Serum Electrolytes & Creatinine | Metabolic acidosis, renal dysfunction |
| α₁-Antitrypsin level | If early-onset or family history of COPD (accounts for <1% of cases) |
| Sputum Culture & Sensitivity | If infective exacerbation suspected — identify organism |
5. Cardiac Investigations
| Test | Purpose |
|---|---|
| ECG | Detects dysrhythmias, right ventricular hypertrophy (P pulmonale), ischemia |
| Echocardiography | Pulmonary arterial pressure (PASP ≥35 mmHg = pulmonary hypertension); right ventricular function; left heart failure |
The ECG detects dysrhythmias or ischemia but does not accurately assess the severity of pulmonary hypertension. BNP helps differentiate COPD from acute heart failure. — Tintinalli's Emergency Medicine, p. 509
6. Bronchoscopy (if lung cancer is suspected)
- Indicated if CT shows a lung mass, nodule, or unexplained hilar lymphadenopathy
- Allows direct visualization, biopsy, and BAL
- Endobronchial ultrasound (EBUS) bronchoscopy for mediastinal staging
CT and PET scans help exclude malignancy in smokers; endobronchial ultrasound bronchoscopy is used for investigation of pulmonary nodules or masses. — Harrison's Principles of Internal Medicine, 22E
7. Additional Tests (if cause remains unclear)
| Test | Indication |
|---|---|
| Cardiopulmonary Exercise Test (CPET) | Differentiates cardiac vs. respiratory cause of dyspnea |
| V/Q Scan or CT-PA | If pulmonary embolism is suspected |
| 6-Minute Walk Test | Functional status and oxygen desaturation on exertion |
| Sleep Study (Polysomnography) | If overlap syndrome (COPD + OSA) suspected |
| Pulse Oximetry | Baseline oxygen saturation monitoring |
Summary: Priority Order of Tests
| Priority | Test |
|---|---|
| First-line | Chest X-ray, Spirometry/PFTs, ABG, CBC, CRP, BNP, ECG |
| Second-line | CT Chest (HRCT or CT-PA), Echocardiography, Sputum culture |
| Third-line / specialist | Bronchoscopy (EBUS), CPET, Right heart catheterization, Lung biopsy |
Clinical Bottom Line: In a 68-year-old with a 30-year smoking history, spirometry is mandatory to confirm COPD, and CT chest is essential to exclude an underlying lung malignancy. BNP helps differentiate from heart failure, and ABG quantifies the severity of respiratory impairment. Minor hemoptysis in a COPD patient should always raise suspicion for lung cancer and prompt urgent CT/bronchoscopy.
Sources: Tintinalli's Emergency Medicine; Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's Textbook of Respiratory Medicine; Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.