Asprin
Reading File
Finding Sources
Searching the Web
aspirin pharmacology mechanism uses clinical indications 2025
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Here is a comprehensive overview of Aspirin (Acetylsalicylic Acid):
Aspirin (Acetylsalicylic Acid)
Drug Class
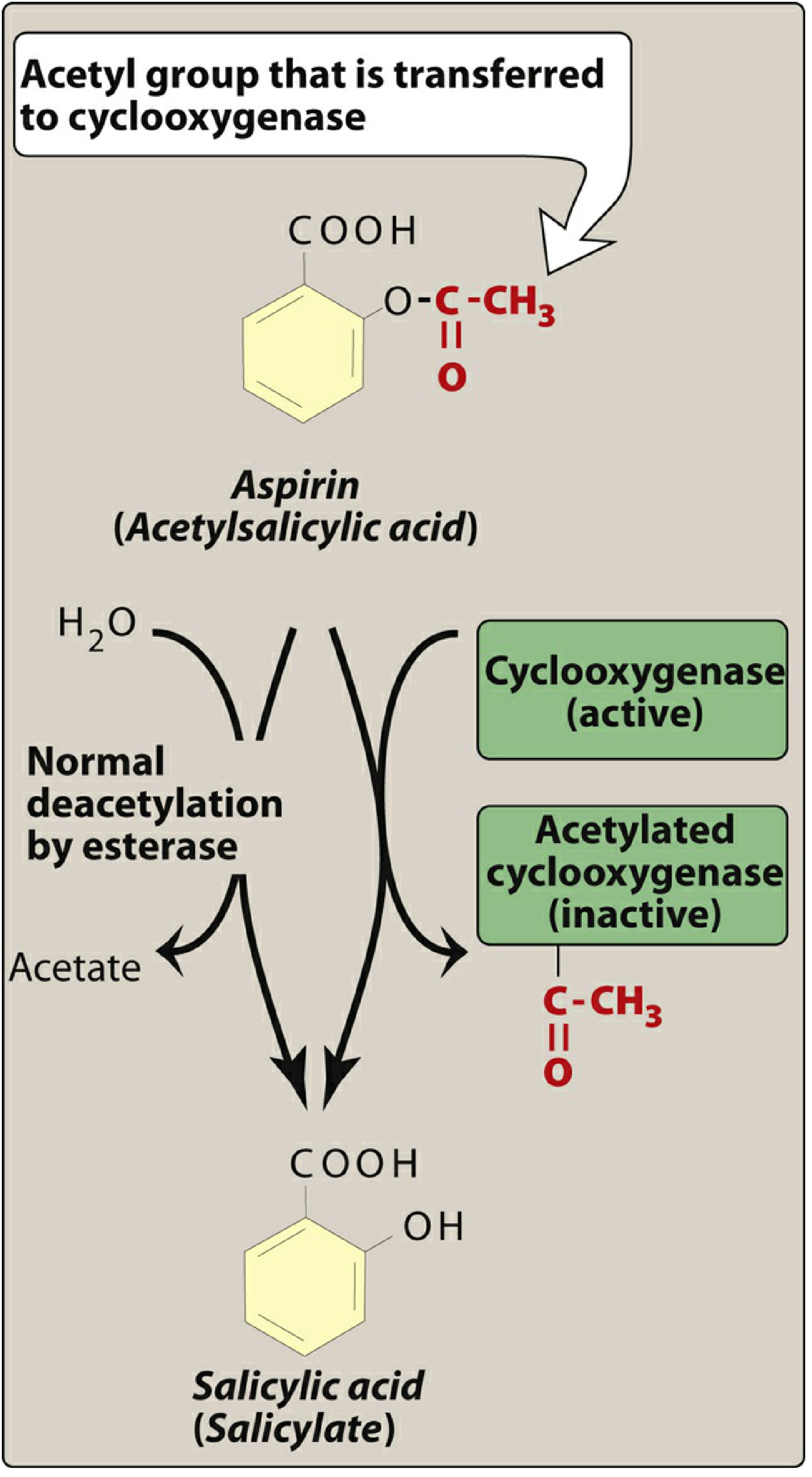
Aspirin belongs to the salicylate subclass of NSAIDs (Non-Steroidal Anti-Inflammatory Drugs). Unlike other NSAIDs, it is an irreversible inhibitor of cyclooxygenase — this distinction is clinically critical.
Mechanism of Action
Aspirin is a weak organic acid that irreversibly acetylates a serine residue near the active site of cyclooxygenase (COX), rendering the enzyme permanently inactive:
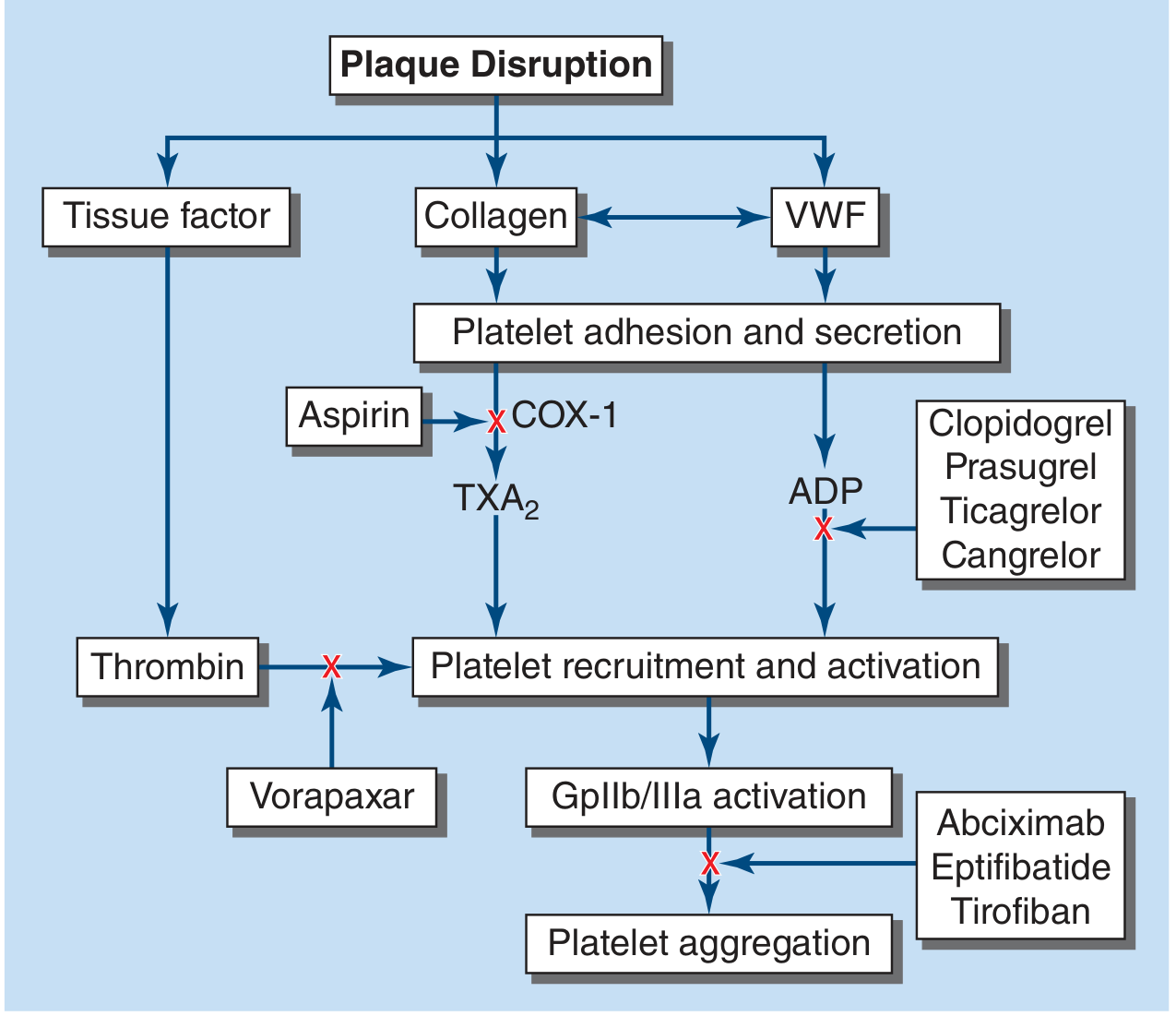
- COX-1 inhibition (low doses): Blocks thromboxane A₂ (TXA₂) synthesis in platelets → inhibits platelet aggregation and vasoconstriction. Because platelets are anucleate and cannot synthesize new COX, this effect lasts 7–10 days (the entire platelet lifespan).
- COX-2 inhibition (high doses, ~1 g/day): Also inhibits COX-2 in endothelial cells → reduces prostacyclin (PGI₂) synthesis, which normally acts as a vasodilator and platelet inhibitor. This partially offsets the antiplatelet benefit at high doses.
Pharmacological Effects
| Effect | Mechanism |
|---|---|
| Antiplatelet | COX-1 inhibition → ↓ TXA₂ → ↓ platelet aggregation |
| Analgesic | ↓ PG synthesis → ↓ peripheral sensitization |
| Antipyretic | ↓ PGE₂ in hypothalamus → ↓ fever |
| Anti-inflammatory | ↓ prostaglandins/prostacyclin (only at high doses) |
Site of Action in Platelet Cascade
Clinical Indications
Cardiovascular (Primary Use at Low Doses: 75–325 mg/day)
- Secondary prevention of cardiovascular events in patients with established coronary artery disease, cerebrovascular disease, or peripheral arterial disease — produces a ~25% reduction in cardiovascular death, MI, or stroke vs. placebo.
- Acute MI / ACS: Initial dose of ≥160 mg for rapid platelet inhibition.
- Post-PCI / stent: Often combined with a P2Y12 inhibitor (clopidogrel, ticagrelor) as dual antiplatelet therapy (DAPT).
- Primary prevention: No longer routinely recommended. May be considered only in adults aged 40–59 with ≥10% 10-year CVD risk and low bleeding risk, as hemorrhagic risks outweigh benefits in lower-risk individuals.
Analgesic / Antipyretic / Anti-inflammatory
- Headache, musculoskeletal pain, fever (at higher doses of 325–650 mg q4–6h)
- Rheumatic diseases (at high doses 3–6 g/day, rarely used now)
Other
- Kawasaki disease: High-dose aspirin is standard of care
- Pericarditis: Used as anti-inflammatory
- Pre-eclampsia prevention: Low-dose aspirin in high-risk pregnancies
Dosing
| Indication | Dose |
|---|---|
| Antiplatelet (maintenance) | 75–100 mg/day |
| Antiplatelet (loading) | ≥160 mg stat |
| Analgesic/antipyretic | 325–650 mg q4–6h |
| Anti-inflammatory | 3–6 g/day (high-dose, rarely used) |
Higher doses are not more effective for cardiovascular protection and increase bleeding risk.
Adverse Effects
| Effect | Notes |
|---|---|
| GI: dyspepsia, erosive gastritis, peptic ulcer, GI bleeding | Dose-related; enteric coating does NOT eliminate risk |
| Bleeding | Overall ~1–3% major bleeding/year; 2–3× higher with dual antiplatelet or anticoagulant combinations |
| Aspirin hypersensitivity | Bronchospasm in ~0.3% general population; higher in asthmatics with nasal polyps or chronic rhinitis |
| Reye's syndrome | Avoid in children with viral illness (encephalopathy + liver failure risk) |
| Hepatic/renal toxicity | With overdose/high chronic doses |
Salicylate Toxicity (Overdose)
- Classically causes a mixed respiratory alkalosis + metabolic acidosis
- Serum acidosis promotes drug entry into CNS (increases toxicity)
- Urinary alkalinization (sodium bicarbonate) is a key treatment to trap salicylate in urine and enhance excretion
Contraindications / Cautions
- Active peptic ulcer disease
- Bleeding disorders
- Aspirin allergy / NSAID hypersensitivity
- Children with viral infections (Reye's syndrome risk)
- Last trimester of pregnancy (premature closure of ductus arteriosus)
Aspirin Resistance
Failure to inhibit platelet TXA₂ production or aggregation. Causes include poor compliance, reduced absorption, drug interaction with ibuprofen (which competitively blocks COX-1 access), and COX-2 overexpression. Testing for resistance is not yet standardized for clinical use.
Sources: Harrison's Principles of Internal Medicine 22e (2025); Lippincott Illustrated Reviews: Pharmacology; Katzung's Basic & Clinical Pharmacology 16e; Braunwald's Heart Disease; Goodman & Gilman's Pharmacological Basis of Therapeutics
Explain
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.