A 50 year has tongue cancer and on active chemotherapy has develop acute swelling under chin right side , swelling is hard in nature and fix , no any other symptoms
Reading File
Finding Sources
Finding Sources
Searching PubMed
"tongue cancer" AND "neck metastasis" AND chemotherapy
Finding Sources
Finding Sources
Searching PubMed
"oral tongue" AND "cervical lymph node" AND metastasis
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Now I have all the information needed for a thorough clinical answer.
Clinical Assessment: Hard, Fixed Submental Swelling in a Tongue Cancer Patient on Chemotherapy
Most Likely Diagnosis: Nodal Metastasis (Level IA - Submental lymph node)
The clinical picture here is highly suspicious for regional lymph node metastasis, specifically to the submental (Level IA) lymph node, representing either:
- New nodal metastasis during chemotherapy (disease progression/chemotherapy failure), or
- Progression of a previously existing occult nodal deposit that is now clinically apparent
The hallmarks pointing squarely toward malignant nodal disease are:
- Hard consistency - metastatic nodes are typically firm to hard (as opposed to soft, fluctuant nodes seen in abscess or reactive lymphadenitis)
- Fixed nature - fixation indicates extracapsular spread (ECS) with invasion into surrounding soft tissue, a particularly ominous sign
- No other symptoms - no fever, no local warmth/redness that would suggest infection
Anatomy - Why Submental (Level I) for Tongue Cancer?
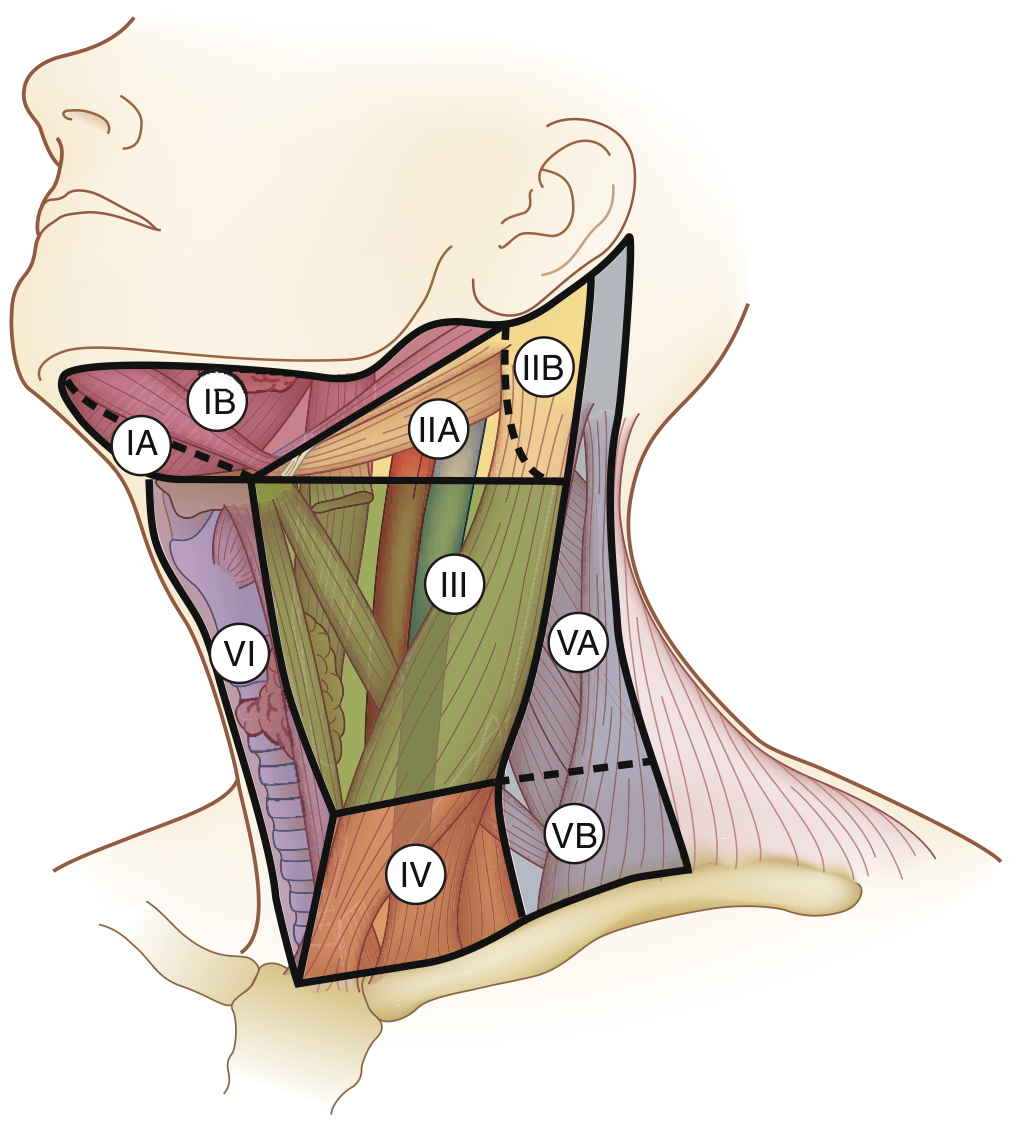
- Level I (submental + submandibular) is the first-echelon drainage for the anterior oral tongue, floor of mouth, and buccal mucosa
- Oral cavity cancers classically metastasize to Levels I, II, and III
- Anterior tongue cancer in particular drains to Level IA (submental) and can even involve the contralateral neck
Per Cummings Otolaryngology: "The nodes in the submandibular triangle are frequently involved in patients with carcinoma of the floor of the mouth, anterior oral tongue, and buccal mucosa."
Per Sabiston Textbook of Surgery: "Oral cavity cancers commonly metastasize to levels I-III... Lymphadenopathy seen in distant levels, such as level V, may suggest a more advanced degree of spread and thus a poorer prognosis."
Differential Diagnosis
| Diagnosis | For | Against |
|---|---|---|
| Nodal metastasis (most likely) | Hard, fixed, known tongue cancer, Level I location, on chemo (may suggest resistance) | - |
| Reactive lymphadenopathy | Known malignancy present | Soft/mobile nodes; hard & fixed favors malignancy |
| Abscess/infected node | Immunocompromised on chemo | No fever, not fluctuant, hard not soft, no erythema |
| Ludwig's angina | Submandibular/submental area | Hard fixed, no sepsis signs, floor of mouth not indurated |
| Salivary gland pathology | Submental region | Unilateral, fixed, no glandular symptoms |
| Second primary | Patient has known cancer | Less likely acutely |
Clinical Significance of "Fixed" Node
A fixed lymph node in the context of malignancy implies extracapsular extension (ECE), which:
- Upstages the nodal disease (changes N1 to N3b in AJCC 8th edition for H&N)
- Makes surgical resection more complex
- Mandates adjuvant radiotherapy ± chemotherapy post-surgery
- Carries a significantly worse prognosis
Immediate Workup Required
-
Imaging (CECT neck, chest, abdomen-pelvis)
- Assess the node: size, internal necrosis, extracapsular spread, relation to adjacent vessels (carotid, IJV)
- Rule out distant metastases
- MRI preferred for soft-tissue detail when feasible
-
FNAC or Core Biopsy of the node
- Confirm metastatic SCC vs. other pathology
- Assess for HPV/p16 status if not already done
-
PET-CT (if available)
- Full-body staging to rule out systemic disease
- Assess true extent of nodal involvement
-
Review of primary tumor - is the tongue primary also progressing?
-
Reassess chemotherapy regimen - new nodal disease while on active chemo signals possible chemotherapy failure/resistance
Management Implications
Since this patient is already on active chemotherapy and has developed a new fixed nodal mass, this is a red flag for treatment failure:
- If confirmed as nodal progression: the current chemotherapy regimen is likely ineffective
- Per Goldman-Cecil Medicine: In recurrent/metastatic HNSCC, pembrolizumab (anti-PD-1), either as monotherapy or combined with platinum + 5-FU, is the standard salvage systemic therapy
- For platinum-refractory disease: nivolumab or pembrolizumab improves survival
- Multidisciplinary team (surgical oncology, radiation oncology, medical oncology) review is essential
- If disease is resectable: salvage surgery + post-op radiotherapy may be considered
- Palliative/supportive care discussion if disease is unresectable
Key Points Summary
- A hard, fixed submental swelling in a known tongue cancer patient = metastatic lymph node (Level IA) until proven otherwise
- The fixed nature suggests extracapsular spread - this is not a benign reactive node
- The fact that it appeared during active chemotherapy raises serious concern for chemotherapy resistance/progression
- Urgent imaging + biopsy is needed
- Refer promptly to the treating oncology/ENT team for multidisciplinary reassessment and likely regimen change
Sources: Cummings Otolaryngology Head and Neck Surgery, p.2298; Sabiston Textbook of Surgery, p.938; Goldman-Cecil Medicine, p.2017
This is a shared conversation. Sign in to Orris to start your own chat.