explain the conductive system
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Here is a complete explanation of the cardiac conduction system, drawn from Ganong's Review of Medical Physiology, Harrison's Principles of Internal Medicine 22E, and Robbins Pathologic Basis of Disease.
The Cardiac Conduction System
The conduction system is a network of specialized myocytes that generates and propagates electrical impulses to coordinate the orderly contraction of the heart - atria first, then ventricles.
Anatomy and Components
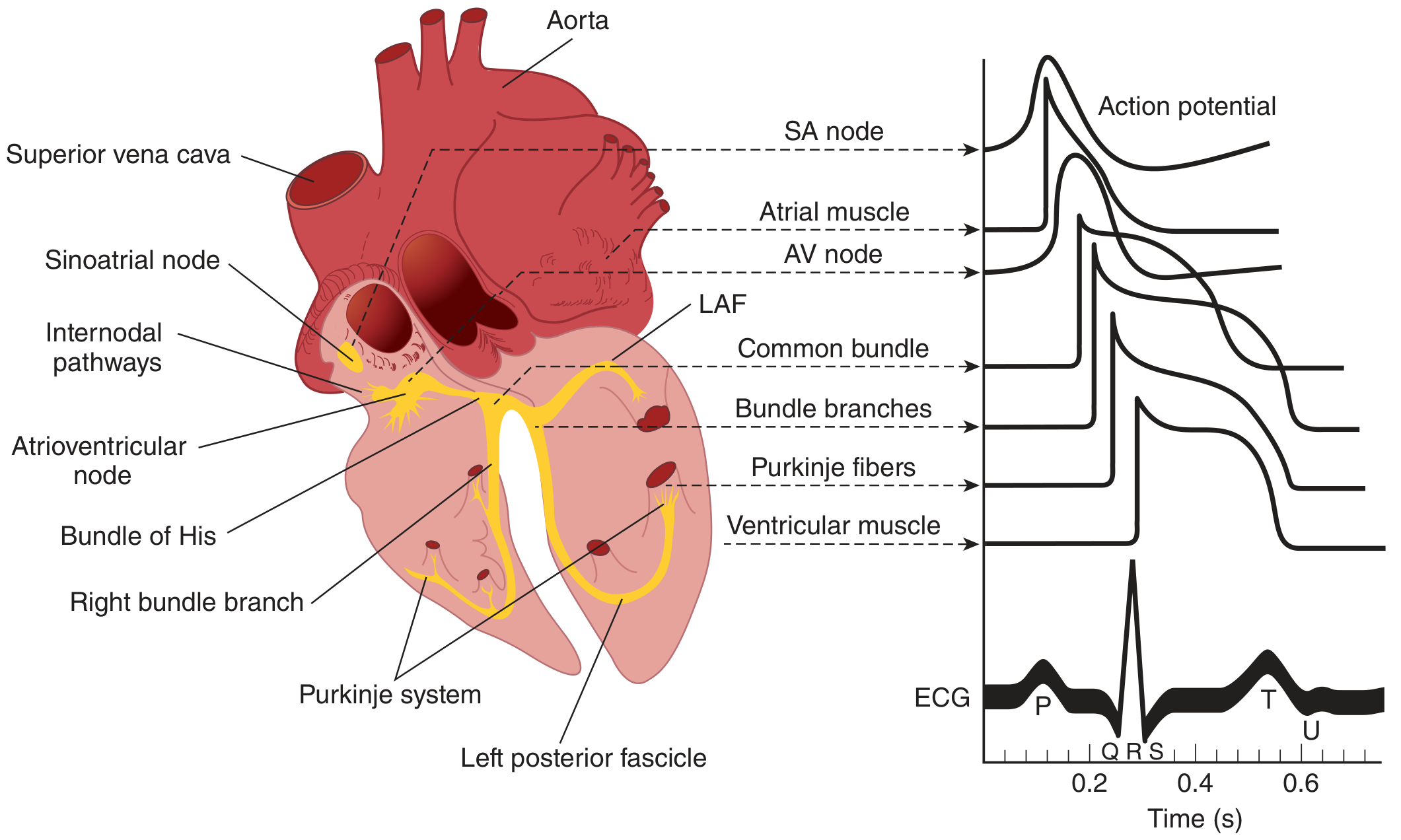
Figure: Conducting system anatomy (left) with corresponding action potentials of each tissue and the surface ECG (right). - Ganong's Review of Medical Physiology, 26th Ed.
The system has five main components, in order of impulse flow:
1. Sinoatrial (SA) Node - The Pacemaker
- Located at the junction of the right atrial appendage and superior vena cava
- Spontaneously depolarizes at 60-100 beats/min - the fastest of any conduction tissue
- Because it fires fastest, it "overdrive suppresses" all other potential pacemakers, making it the dominant pacemaker
- Innervated primarily by the right vagus (parasympathetic) and right stellate ganglion (sympathetic)
- Conduction speed within the SA node: 0.05 m/s (very slow)
2. Internodal Atrial Pathways
- Three bundles carry the impulse from SA to AV node: the anterior, middle (Wenckebach), and posterior (Thorel) tracts
- Bachmann's bundle is a branch of the anterior internodal tract connecting the right and left atria
- Conduction through these pathways: 1 m/s
- Atrial depolarization is complete in about 0.1 second, generating the P wave on the ECG
3. Atrioventricular (AV) Node
- Located in the right posterior portion of the interatrial septum (right atrium along the interatrial septum)
- Conduction speed: 0.05 m/s - deliberately slow
- This creates the AV nodal delay of ~0.1 s, which ensures atrial contraction is complete before ventricular filling ends and systole begins - the AV node acts as a "gatekeeper"
- The AV node is continuous with the Bundle of His; together they form the AV junction
- Innervated primarily by the left vagus and left stellate ganglion
4. Bundle of His (AV Bundle) and Bundle Branches
- The Bundle of His exits the AV node and enters the interventricular septum
- At the top of the septum it bifurcates into:
- Right bundle branch - descends along the right side of the septum
- Left bundle branch - divides further into:
- Left anterior fascicle (LAF)
- Left posterior fascicle
- Conduction speed: 1 m/s
- The atrial and ventricular myocardium are separated by a fibrous ring; the Bundle of His is normally the only electrical bridge between them
5. Purkinje System
- The bundle branches arborize into the Purkinje fiber network, spreading subendocardially across both ventricles
- Purkinje fibers are large cells, fewer mitochondria, less striated, and highly specialized for rapid conduction
- Conduction speed: 4 m/s - the fastest in the heart
- This rapid spread activates both ventricles synchronously in 0.08-0.1 s, generating the QRS complex
Conduction Speeds (Summary Table)
| Tissue | Conduction Rate |
|---|---|
| SA node | 0.05 m/s |
| Atrial pathways | 1 m/s |
| AV node | 0.05 m/s |
| Bundle of His | 1 m/s |
| Purkinje system | 4 m/s |
| Ventricular muscle | 1 m/s |
- Ganong's Review of Medical Physiology, 26th Ed., Table 29-1
Sequence of Excitation
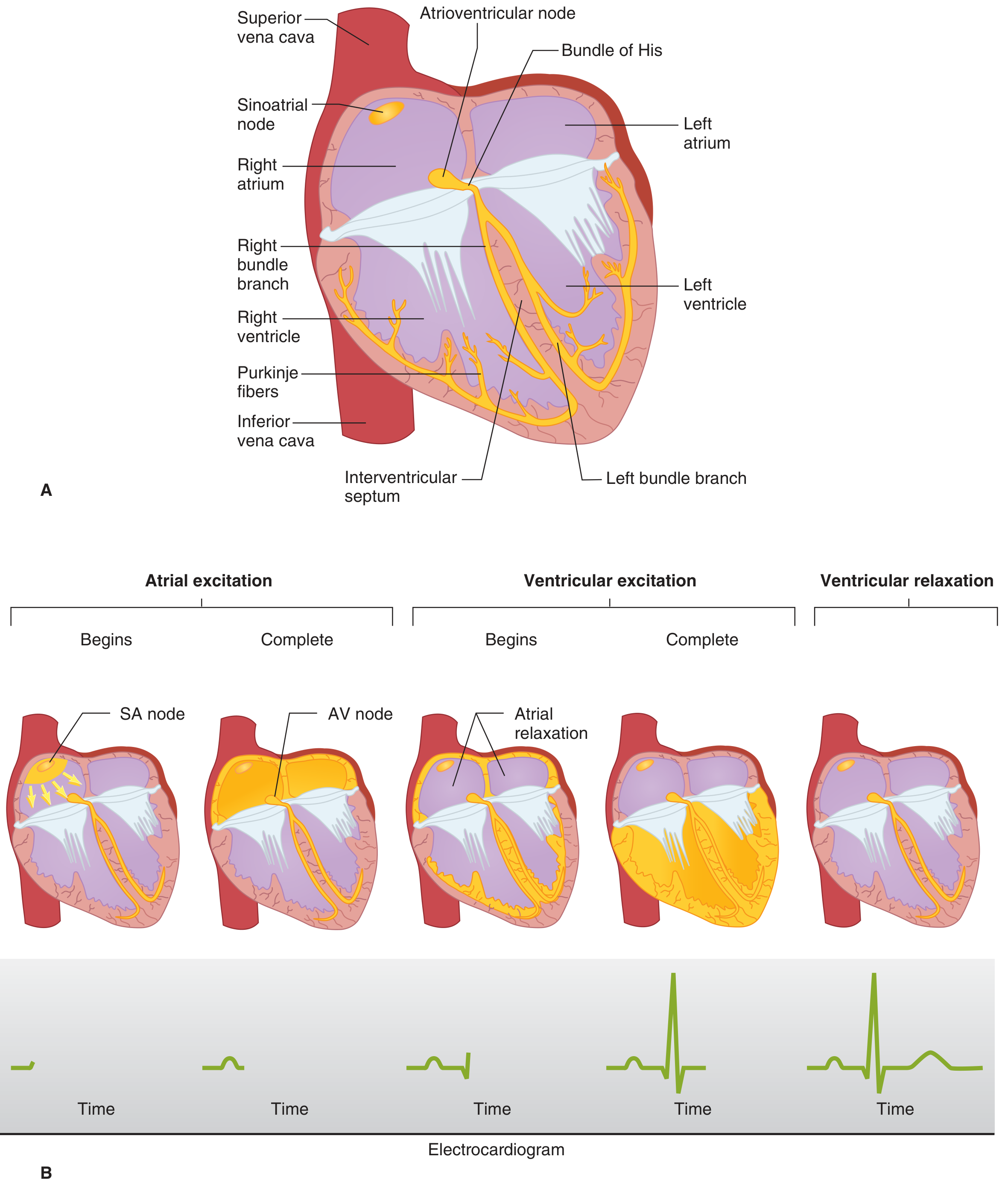
Figure: (A) Conducting system anatomy. (B) Step-by-step spread of excitation from SA node to atria, through AV node, down bundle branches to ventricles, with the corresponding ECG building up at each stage. - Ganong's Review of Medical Physiology, 26th Ed.
- SA node fires → impulse spreads radially through atria via internodal pathways → P wave on ECG
- AV nodal delay (~0.1 s) → PR interval on ECG; sympathetic stimulation shortens this, vagal stimulation lengthens it
- Impulse enters Bundle of His, splits into right and left bundle branches
- Purkinje system rapidly activates ventricular endocardium
- Depolarization spreads from endocardium to epicardium, starting at the left side of the interventricular septum, moving right across the septum mid-portion, then down to the apex, then up the ventricular walls → QRS complex
- Last areas to depolarize: posterobasal left ventricle, pulmonary conus, uppermost septum
- Ventricular repolarization → T wave (and sometimes U wave)
Automaticity and Escape Rhythms
All conduction tissue cells can depolarize spontaneously (automaticity), but each has a different intrinsic rate:
| Site | Intrinsic Rate |
|---|---|
| SA node | 60-100 bpm |
| AV junction | 40-60 bpm |
| Purkinje / ventricular | 20-40 bpm |
If the SA node fails or is suppressed, the next fastest tissue takes over as an escape pacemaker. This is why AV junctional and ventricular escape rhythms are always slower than sinus rhythm. If any site fires faster than the SA node (enhanced automaticity), it becomes an ectopic pacemaker and can cause tachyarrhythmias.
Autonomic Regulation
| Input | Effect on SA Node | Effect on AV Node |
|---|---|---|
| Parasympathetic (vagal) | Decreases automaticity (slows rate) | Slows conduction (lengthens PR) |
| Sympathetic | Increases automaticity (speeds rate) | Speeds conduction (shortens PR) |
Acetylcholine also acts presynaptically to reduce norepinephrine release from sympathetic terminals, and neuropeptide Y from adrenergic endings can inhibit acetylcholine release - these reciprocal interactions fine-tune moment-to-moment heart rate.
Clinical Relevance
- SA node dysfunction (sick sinus syndrome): bradycardia, sinus pauses, tachy-brady syndrome
- AV block: 1st degree (prolonged PR), 2nd degree (Mobitz I/II - some impulses don't get through), 3rd degree (complete block - atria and ventricles beat independently)
- Bundle branch block: right (RBBB) or left (LBBB) bundle branch block widens the QRS as one ventricle activates late
- Accessory pathways (e.g., Bundle of Kent in WPW syndrome): bypass the AV node, causing pre-excitation and re-entrant tachycardias
- Hyperkalemia: can block conduction entirely by depolarizing the resting membrane potential
Sources: Ganong's Review of Medical Physiology 26th Ed. | Harrison's Principles of Internal Medicine 22E (2025) | Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.