I now have all the information needed to compose a thorough, well-structured answer. Here is the complete case analysis:
CASE B - Full Case Analysis: Upper GI Bleeding / Peptic Ulcer Disease
1. DIAGNOSIS
Primary Diagnosis: Upper Gastrointestinal Bleeding (UGIB) secondary to Peptic Ulcer Disease (PUD)
This patient has a bleeding peptic ulcer, most likely a duodenal or gastric ulcer, on a background of NSAID/aspirin use, chronic alcohol consumption, and cigarette smoking. The black, sticky, malodorous (tarry) stools (melena), chronic epigastric burning refractory to antacids, and multiple mucosal risk factors point directly to this diagnosis.
2. DIFFERENTIAL DIAGNOSIS AND BASIS
Most Likely
| Condition | Supporting Evidence |
|---|
| Bleeding peptic ulcer (gastric or duodenal) | Chronic epigastric burning, NSAID/aspirin use, smoking, alcohol, melena, epigastric tenderness |
| Gastritis / erosive gastropathy | Same risk factors; NSAID/alcohol-induced mucosal erosions |
Other Causes of UGIB to Consider
| Condition | Why Considered / Why Less Likely |
|---|
| Esophageal/gastric varices | Alcohol use raises concern; however, no hepatomegaly, no jaundice, no ascites, PT/PTT normal - against cirrhosis |
| Mallory-Weiss tear | No history of retching or vomiting preceding bleed |
| Esophagitis | Chronic reflux symptoms possible; however, typically causes less hemodynamic instability |
| Gastric malignancy | No weight loss, good appetite; less likely but should be excluded endoscopically |
| Dieulafoy lesion | Can present with massive sudden UGIB, but less common |
Peptic ulcer is the most common cause of severe UGIB, accounting for approximately 35-40% of cases in large endoscopy databases. - Sleisenger and Fordtran's Gastrointestinal and Liver Disease
3. PHYSICAL EXAMINATION FINDINGS EXPLAINED
Vital Signs - Orthostatic Hypotension + Tachycardia
- Supine BP 120/80, Standing BP 90/60 (drop of ≥20 mmHg systolic), HR 110 = Orthostatic (postural) hypotension with compensatory tachycardia
- This indicates significant intravascular volume depletion. A drop in BP of ≥20 mmHg systolic and/or ≥10 mmHg diastolic upon standing, accompanied by tachycardia, signifies loss of approximately 15-20% of total blood volume (roughly 750-1000 mL)
- How to identify: Measure BP and HR supine, then have patient sit or stand for 1-3 minutes, remeasure. Tachycardia and tachypnea are the first clinical signs of significant bleeding, followed by orthostatic changes. - Tintinalli's Emergency Medicine
Pale Palpebral Conjunctiva
- Reflects anemia (Hgb 9 g/dL). The inner lower eyelid is everted; pallor rather than the normal pink-red color indicates reduced hemoglobin in the submucosal vessels
- A reliable bedside indicator of anemia, especially when Hgb falls below 9-10 g/dL
Cool Extremities + Rapid/Weak Peripheral Pulses
- Consequence of compensatory peripheral vasoconstriction. In response to reduced cardiac output from hypovolemia, catecholamine release causes peripheral arteriolar constriction, shunting blood to core organs. This reduces skin perfusion (cool, clammy extremities) and reduces pulse volume (weak, thready pulses) despite tachycardia
- Indicates the patient is in compensated hypovolemic shock
Epigastric Tenderness + LUQ Tenderness
- Direct tenderness (tenderness on direct palpation, without rebound) in the epigastrium reflects inflammation and ulceration of the gastric or duodenal mucosa
- No guarding or rebound = no peritonitis, meaning the ulcer has NOT perforated
- Hyperactive bowel sounds: blood in the GI lumen acts as a cathartic - the iron and protein content of blood stimulates intestinal motility
Anxious and Restless Appearance
- Reflects early cerebral hypoperfusion and catecholamine excess due to hypovolemia. The brain begins to receive inadequate oxygen delivery, producing anxiety and agitation
Anicteric Sclera
- Normal white sclera (no jaundice) argues against liver failure or biliary disease as a cause
Rectal Exam - Black Tarry Stool (Melena)
- Melena is defined as black, tarry, sticky, malodorous stool resulting from degradation of hemoglobin to hematin by intestinal bacteria. It generally requires at least 50-100 mL of blood from a source proximal to the ileocecal valve. - Sleisenger and Fordtran's
4. LABORATORY FINDINGS EXPLAINED
| Finding | Value | Interpretation |
|---|
| Hemoglobin 9 g/dL | Low (Normal: 13.5-17.5 g/dL in males) | Significant blood loss. Note: in acute bleeding, Hgb may underestimate true loss initially because hemodilution takes hours to equilibrate |
| Hematocrit 27% | Low (Normal: 41-53% in males) | Consistent with moderate-severe anemia from blood loss |
| MCV 90 fL | Normal (normocytic) | Suggests acute blood loss anemia (not chronic iron deficiency, which gives microcytic anemia with low MCV). Confirms this is an acute bleed on possibly a chronic background |
| WBC 13,000 | Mildly elevated | Stress leukocytosis - a physiologic response to acute hemorrhage; also, digested blood proteins can stimulate WBC production |
| BUN 45 mg/dL | Elevated | Key finding: Digested blood in the small intestine is absorbed as urea, raising BUN. BUN:Creatinine ratio = 45:1.0 = 45 - a ratio >30 strongly suggests an upper GI source. - Frameworks for Internal Medicine; Sabiston Textbook of Surgery |
| Creatinine 1.0 mg/dL | Normal | Confirms the elevated BUN is from protein digestion (blood), NOT from renal failure. If creatinine were elevated, BUN:Cr ratio would be less discriminating |
| PT/PTT Normal | Normal | No coagulopathy; bleeding is from a structural/mucosal lesion, not a clotting defect |
| Chest X-ray Normal | Normal | Rules out free air under the diaphragm (which would indicate ulcer perforation) |
| KUB Normal | Normal | No free air, no obstruction, no perforation |
BUN:Creatinine ratio >30 has sensitivity 39%, specificity 94%, LR+ 7.5 for upper GI source of bleeding. - Symptom to Diagnosis, 4th Edition
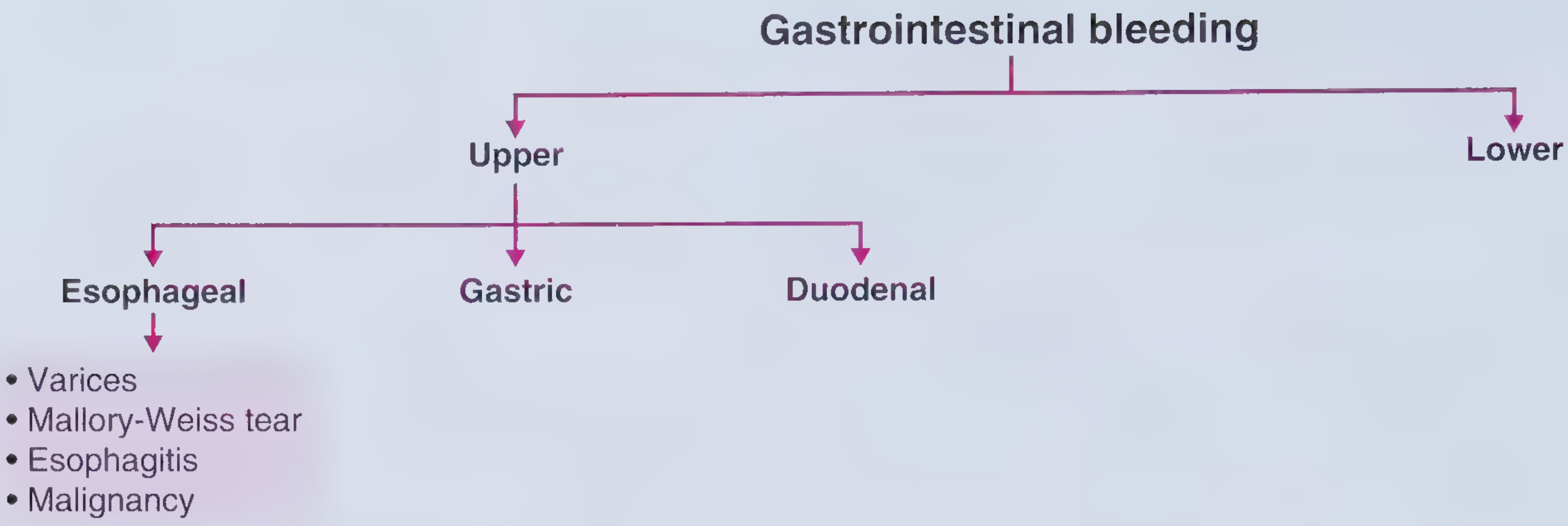
5. TYPES OF GASTROINTESTINAL BLEEDING
GI bleeding is classified anatomically and by presentation:
A. By Location
Upper GI Bleeding (UGIB) - source proximal to the ligament of Treitz (esophagus, stomach, duodenum)
- Presents as hematemesis (vomiting blood or coffee grounds) and/or melena (black tarry stools)
- Subcategories: esophageal, gastric, duodenal
Lower GI Bleeding (LGIB) - source distal to the ligament of Treitz (small bowel, colon, anorectum)
- Presents as hematochezia (bright red or maroon blood per rectum)
- Note: massive UGIB can also cause hematochezia in 10-15% of cases
Small Bowel Bleeding - between ligament of Treitz and ileocecal valve (a distinct intermediate category, often "obscure GI bleeding")
B. By Clinical Presentation
| Type | Description |
|---|
| Overt bleeding | Visible - hematemesis, melena, hematochezia |
| Occult bleeding | Not visible to naked eye; detected only by fecal occult blood test (FOBT) or iron-deficiency anemia |
| Obscure bleeding | Persistent or recurrent bleeding with no source found after EGD and colonoscopy |
C. By Severity
- Mild: No hemodynamic compromise, Hgb >10
- Moderate: Orthostatic changes, Hgb 7-10
- Severe: Shock, requires ICU, Hgb <7
This patient has overt, moderate-to-severe UGIB.
6. CAUSES OF UPPER GI BLEEDING (the type in this patient)
The following table shows the frequency of causes in a large endoscopic database:
| Cause | Frequency |
|---|
| Peptic ulcer | 35.2% (most common) |
| Esophageal or gastric varices | 21.9% |
| Portal hypertension-related lesions | 4.6% |
| Esophagitis | 4.6% |
| Angioectasia | 4.0% |
| Mallory-Weiss tear | 4.0% |
| Dieulafoy lesion | 3.2% |
| UGI tract neoplasm | 3.1% |
| Epistaxis (swallowed blood) | 2.2% |
| Erosions | 1.2% |
| Other / No cause found | ~16% |
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease (UCLA CURE Database, n=968)
7. PATHOPHYSIOLOGY OF PEPTIC ULCER DISEASE WITH BLEEDING
Normal Mucosal Defense
The gastric mucosa is protected by a balance of:
- Defensive factors: mucus-bicarbonate layer, mucosal blood flow, epithelial renewal, prostaglandins (PGE2, PGI2)
- Aggressive factors: hydrochloric acid, pepsin
How Ulcers Form in This Patient
Step 1 - NSAIDs and Aspirin disrupt mucosal defense:
- NSAIDs (including aspirin) inhibit cyclooxygenase (COX-1 and COX-2) enzymes
- COX-1 is constitutively expressed in the gastric mucosa and produces protective prostaglandins (PGE2, PGI2)
- Prostaglandins stimulate mucus secretion, bicarbonate secretion, mucosal blood flow, and epithelial cell proliferation
- COX-1 inhibition by NSAIDs → reduced prostaglandin synthesis → decreased mucus/bicarbonate → mucosal vulnerability to acid
- Aspirin also has a direct topical irritant effect (acid trapping in epithelial cells)
Step 2 - Alcohol:
- Ethanol is directly toxic to gastric epithelium, disrupts the mucous barrier, increases back-diffusion of acid into the mucosa, and impairs mucosal healing
Step 3 - Cigarette smoking:
- Reduces mucosal blood flow and healing; impairs prostaglandin synthesis; increases acid secretion; may promote H. pylori colonization
Step 4 - Acid injury:
- With defensive mechanisms disrupted, gastric acid and pepsin penetrate the mucosal barrier
- Mucosal erosion progresses through the epithelium, lamina propria, muscularis mucosae, and into the submucosa/muscularis propria = ulcer
Step 5 - Bleeding:
- The ulcer erodes into submucosal blood vessels (arterioles)
- Arterial erosion causes active spurting hemorrhage (high risk); venous erosion causes slower oozing
- Blood enters the GI lumen, is digested by gastric acid and bacteria
- Hemoglobin → hematin (black pigment) → melena
Summary of risk factors present in this patient:
- NSAIDs (COX inhibition)
- Aspirin (COX inhibition + topical acid)
- Chronic alcohol use (direct mucosal toxin)
- Cigarette smoking (2 packs/day - reduces healing, blood flow)
- Chronic epigastric symptoms (pre-existing ulcer disease)
- Hypertension (likely on antihypertensives that may affect splanchnic perfusion)
Source: Robbins & Kumar Basic Pathology; Sleisenger and Fordtran's
8. ALGORITHM: MANAGEMENT OF GI BLEEDING BASED ON ENDOSCOPIC FINDINGS
Initial Resuscitation (before endoscopy)
- Two large-bore IV lines (≥18 gauge) or central cordis
- Supplemental oxygen; consider intubation if hematemesis/altered mental status
- IV fluid resuscitation immediately - do not delay for ICU transfer
- Admit to ICU if hemodynamic instability or active bleeding
- Type and screen / crossmatch
- IV Proton Pump Inhibitor (PPI) - high-dose; continuous infusion or every 12 hours IV
- Transfuse if Hgb <7 g/dL (restrictive strategy shown to reduce mortality and rebleeding vs. liberal strategy)
Endoscopy within 24 hours after adequate resuscitation in most patients with overt UGIB
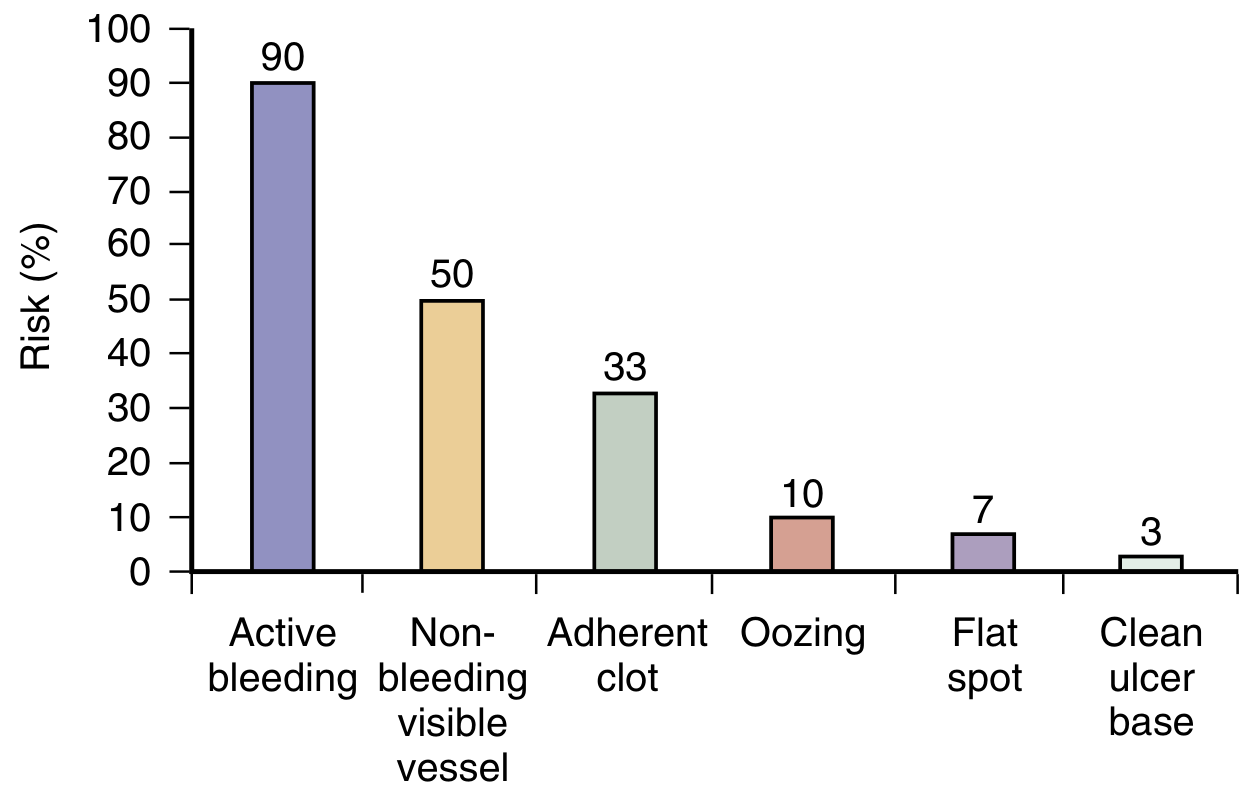
Endoscopic Findings - Forrest Classification and Management
The Forrest classification stratifies ulcer risk based on endoscopic stigmata of recent hemorrhage (SRH):
| Forrest Class | Appearance | Rebleeding Risk | Management |
|---|
| Ia | Active arterial spurting | ~90% | Endoscopic hemostasis MANDATORY (combination therapy: epinephrine injection + thermal coagulation or clips) + high-dose IV PPI infusion |
| Ib | Active oozing | ~10% | Endoscopic hemostasis + IV PPI |
| IIa | Non-bleeding visible vessel (NBVV) | ~50% | Endoscopic hemostasis MANDATORY + IV PPI |
| IIb | Adherent clot | ~33% | Endoscopic therapy (attempt clot removal + treat underlying vessel) + IV PPI |
| IIc | Flat pigmented spot | ~7% | Medical management with oral PPI; outpatient follow-up acceptable |
| III | Clean ulcer base | ~3% | Oral PPI; may be discharged early if no other high-risk features |
Endoscopic Hemostasis Techniques
- Injection therapy: Epinephrine injection (causes vasoconstriction + tamponade); never used alone - always combined
- Thermal/contact therapy: Bipolar electrocoagulation, thermocoagulation (heater probe) - causes coaptive coagulation of bleeding vessel
- Mechanical therapy: Hemostatic clips (over-the-scope or through-the-scope) - physically occludes vessel
- Non-contact thermal: Argon plasma coagulation (APC)
- Combination therapy (injection + thermal or injection + clips) is superior to monotherapy for high-risk stigmata
Post-Endoscopy Management
- High-dose IV PPI after successful endoscopic hemostasis of high-risk ulcers (reduces rebleeding, transfusion, hospital stay)
- H. pylori testing; eradicate if positive (reduces recurrence)
- Stop NSAIDs and aspirin (if medically permissible); if aspirin must be continued, add PPI
- Repeat endoscopy ("second look") is selective, not routine
- Angiographic embolization for patients who fail endoscopic therapy
- Surgery (oversewing of ulcer, vagotomy/pyloroplasty) for patients refractory to endoscopic + angiographic therapy
Sources: Sleisenger and Fordtran's; Sabiston Textbook of Surgery; Frameworks for Internal Medicine
9. HISTORY OF PRESENT ILLNESS (Reconstructed)
A 45-year-old male advertising executive with a background of hypertension and chronic intermittent epigastric burning presents to the emergency department with a 3-day history of passage of black, sticky, malodorous stools (melena), associated with:
- Lightheadedness - consistent with orthostatic hypotension and cerebral hypoperfusion from blood loss
- Easy fatiguability and generalized body weakness - symptoms of anemia and reduced oxygen delivery to tissues
- Worsening epigastric burning - exacerbation of pre-existing peptic ulcer disease, now unresponsive to doubled doses of antacids (Tums/calcium carbonate)
Relevant exposure history:
- Regular NSAID use for chronic back pain (COX inhibition, impaired mucosal defense)
- Recently started low-dose aspirin for cardiac prophylaxis (additional COX inhibition)
- Heavy cigarette smoking - 2 packs per day (impaired mucosal healing, reduced blood flow)
- Alcohol use - 3-4 martinis/cocktails daily (direct mucosal toxin, portal hypertension risk)
Pertinent negatives: No hematemesis (blood did not reach the esophagus in significant quantity to trigger vomiting), no weight loss (against malignancy), good appetite, no easy bruisability (normal coagulation), no history of liver disease or abdominal surgery
10. ETIOLOGY (Causes - in this specific patient)
This patient has multiple concurrent etiologic factors all converging to produce peptic ulceration and hemorrhage:
Primary Etiologic Agents
| Factor | Mechanism |
|---|
| NSAIDs (chronic use) | COX-1 inhibition → reduced prostaglandin synthesis → breakdown of mucus-bicarbonate barrier → acid injury. In the U.S., NSAID use is now the most common cause of gastric ulcers as H. pylori rates decline with aging population increasing aspirin use - Robbins Basic Pathology |
| Aspirin | Both topical acid injury AND systemic COX inhibition. Even low-dose aspirin disrupts the gastric mucosal barrier |
| Chronic alcohol consumption | Direct toxin to gastric epithelium; disrupts mucous layer; increases back-diffusion of H+ ions; impairs mucosal cell proliferation; causes erosive gastritis |
| Cigarette smoking | Reduces mucosal blood flow and prostaglandin synthesis; impairs ulcer healing; increases gastric acid secretion; may enhance H. pylori virulence |
Contributing/Underlying Factors
| Factor | Role |
|---|
| H. pylori infection (likely, not yet tested) | Present in >70% of PUD; causes chronic gastritis, impairs mucosal defenses; MUST be tested and eradicated |
| Stress / sympathoadrenal activation | Advertising executive with high-stress occupation; stress increases acid secretion, reduces mucosal blood flow |
| Pre-existing peptic ulcer diathesis | Years of chronic episodic epigastric burning suggest a pre-existing vulnerable mucosa |
| Hypertension medications | Some antihypertensives may affect splanchnic perfusion |
Why the Bleed Occurred NOW
The combination of doubling NSAID dose + adding aspirin for cardiac prophylaxis simultaneously overwhelmed an already compromised mucosa (from years of alcohol and smoking), finally tipping the balance from chronic ulceration to frank hemorrhage with erosion into a submucosal vessel.
Summary Table
| Item | Key Points |
|---|
| Diagnosis | UGIB from bleeding peptic ulcer (gastric or duodenal) |
| Key history | 3 days melena, chronic epigastric burning, NSAIDs, aspirin, alcohol, heavy smoking |
| Key exam | Orthostatic hypotension, tachycardia, pale conjunctiva, cool extremities, epigastric tenderness, melena on rectal exam |
| Key labs | Hgb 9, Hct 27%, normocytic (acute), BUN 45 (BUN:Cr = 45 - confirms UGIB), normal PT/PTT, normal Cr |
| Type of GI bleed | Overt, moderate-severe, UPPER GI bleeding (melena) |
| Pathophysiology | NSAID/aspirin COX inhibition + alcohol + smoking → mucosal defense failure → acid injury → ulceration → arterial erosion → melena |
| Management | IV access, resuscitation, IV PPI, upper endoscopy within 24h, hemostasis based on Forrest class, stop NSAIDs, test and treat H. pylori |
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Sabiston Textbook of Surgery; Frameworks for Internal Medicine; Robbins & Kumar Basic Pathology; Tintinalli's Emergency Medicine; Symptom to Diagnosis 4th ed.