Mumps characteristic presentation and treatment
Reading File
Finding Sources
Searching PubMed
mumps clinical presentation treatment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough summary of mumps based on Harrison's 22E, Goldman-Cecil, and Tintinalli's Emergency Medicine.
Mumps - Characteristic Presentation and Treatment
The Pathogen
Mumps virus is a single-stranded, negative-sense, enveloped RNA virus in the Paramyxoviridae family, genus Rubulavirus. There is only one serotype. Twelve genotypes exist (A-N); genotype G predominates in the U.S., while the widely used Jeryl Lynn vaccine strain is genotype A. The virus is rapidly inactivated by formalin, ether, chloroform, heat, and ultraviolet light.
Transmission and Incubation
- Spreads by direct contact with respiratory droplets or saliva from an infected person
- Incubation period: 12-25 days (average 16-18 days)
- Infectivity window: 2 days before to 5 days after onset of parotitis; virus detectable in saliva up to 7 days before and 9 days after onset
- Virus can also be isolated from urine and seminal fluid up to 14 days after parotitis onset
- Humans are the only known natural reservoir
Clinical Presentation
Prodrome (1-2 days before parotitis)
- Low-grade fever
- Malaise
- Myalgia
- Anorexia
- Headache
Cardinal Sign: Parotitis
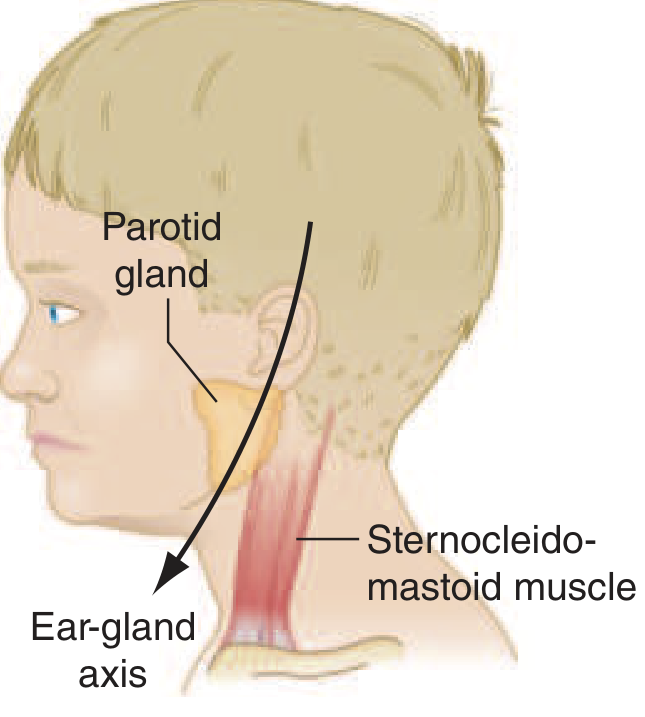
Normal vs. enlarged parotid gland - Harrison's Principles of Internal Medicine 22E
- Parotid gland swelling is the hallmark - occurs in ~95% of symptomatic cases
- Typically starts unilaterally, then progresses to bilateral involvement in most cases
- The gland is tense and painful, but erythema and warmth are notably absent (distinguishing from suppurative parotitis)
- Stensen's duct may appear inflamed, but no pus can be expressed
- Swelling typically lasts 1-5 days
- Can obscure the angle of the mandible
- Submandibular and sublingual glands may also be affected
- Up to 20% of infections are subclinical (asymptomatic)
Complications
Orchitis (most clinically significant in males)
- Occurs in 20-30% of postpubertal males (rare before puberty); usually unilateral but bilateral in ~15-30% of orchitis cases
- Presents with fever, chills, headache, nausea, and testicular pain/swelling - typically 4-8 days after parotitis
- Testicular atrophy follows in ~50% of affected testes, but bilateral atrophy causing sterility is rare (~13% of cases with bilateral orchitis)
- Neither glucocorticoids nor incision of the tunica albuginea are of proven value
Oophoritis / Mastitis
- Oophoritis: ~7% of unvaccinated postpubertal women; presents with lower abdominal pain and vomiting
- Mastitis: up to 30% of unvaccinated postpubertal women; much less common in vaccinated individuals
Pancreatitis
- ~4% of unvaccinated patients; <1% of vaccinated patients
- Elevated serum amylase can reflect either parotitis or pancreatitis; elevated serum lipase helps distinguish pancreatitis
CNS Involvement
- Subclinical CNS involvement (CSF pleocytosis) occurs in up to 55% of patients
- Aseptic meningitis: up to 10% of unvaccinated; ≤1% of vaccinated patients. Self-limited, presents ~5 days after parotitis with stiff neck, headache, drowsiness. Can precede parotitis or occur without parotitis in 40-50% of cases
- Encephalitis: ≤1% of patients; presents with high fever, altered consciousness, seizures (20-30% of CNS cases), focal neurologic signs. Mortality ~1.5%; permanent sequelae possible
- Other CNS manifestations: cerebellar ataxia, facial palsy, transverse myelitis, hydrocephalus, Guillain-Barre syndrome
Hearing Loss
- Up to 4% of unvaccinated patients; <1% of vaccinated patients
- Usually sudden onset, unilateral, and transient; bilateral permanent hearing loss is rare
- Results from viral damage to the cochlea (organ of Corti and tectorial membrane)
Cardiac
- ECG abnormalities in up to 15% of cases (usually transient)
- Rare: myocarditis, endocardial fibroelastosis
Other
- Thyroiditis, nephritis, arthritis, hepatic disease, keratouveitis, thrombocytopenic purpura, hemolytic anemia
Diagnosis
- Primarily clinical in typical presentations
- Lab confirmation indicated for atypical cases, vaccinated individuals, and outbreak investigations
- Buccal swab or urine for RT-PCR (preferred during first 3 days of parotitis)
- Serology: IgM and IgG mumps antibodies (note: IgM may be absent in vaccinated individuals)
- Elevated serum amylase reflects parotid/pancreatic inflammation
Differential diagnosis of parotid swelling includes: suppurative parotitis (pus from Stensen's duct, erythema), sialolithiasis, Sjogren's syndrome, sarcoidosis, lymphoma, drugs (iodine, thiouracil), HIV-associated salivary gland disease.
Treatment
There is no specific antiviral therapy for mumps. Management is entirely supportive:
| Setting | Management |
|---|---|
| Parotitis | Analgesics (NSAIDs/acetaminophen), adequate hydration, soft diet |
| Orchitis | Scrotal support, ice packs, analgesics; glucocorticoids NOT proven beneficial |
| Pancreatitis | IV fluids, analgesia, NPO if severe |
| Aseptic meningitis | Supportive; self-limited |
| Encephalitis | Supportive; ICU-level care as needed |
- Mumps immune globulin is NOT recommended for post-exposure prophylaxis or treatment
- Patients should be isolated (droplet precautions) for 5 days after onset of parotitis
- Children should be excluded from school for 9 days after onset of parotid swelling
- Immunocompetent patients with isolated parotitis or orchitis can be managed as outpatients; admit for systemic complications (encephalitis, severe pancreatitis)
Prevention
- MMR vaccine (2-dose schedule): first dose at 12-15 months, second dose at 4-6 years
- A third dose of MMR has been recommended by the CDC during active outbreaks in high-risk settings (colleges, close-knit communities)
- Vaccine efficacy: ~79-88% per dose; two doses provide ~88% protection
- Disease is milder in vaccinated individuals who do become infected
Sources: Harrison's Principles of Internal Medicine 22E (Ch. 213); Goldman-Cecil Medicine (Ch. 340); Tintinalli's Emergency Medicine; Bradley & Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.