Diabetic mellitus management
Reading File
Finding Sources
Searching PubMed
"diabetes mellitus" AND "management" AND "guidelines"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a thorough, well-structured answer. Let me compile it.
Diabetes Mellitus Management
Based on Harrison's Principles of Internal Medicine 22E (2025), Goodman & Gilman's Pharmacological Basis of Therapeutics, and Rosen's Emergency Medicine.
1. Goals of Therapy
The goals of therapy for all forms of DM are to:
- Eliminate symptoms related to hyperglycemia
- Reduce or eliminate long-term microvascular (retinopathy, nephropathy, neuropathy) and macrovascular (ASCVD, stroke, PAD) complications
- Allow the patient to achieve as normal a lifestyle as possible
Symptoms of hyperglycemia typically resolve when plasma glucose falls below 11.1 mmol/L (200 mg/dL); most treatment therefore targets the reduction of complications.
2. Comprehensive Diabetes Care Framework
Optimal management is far more than glucose control alone. The ADA recommends applying the Chronic Care Model with a multidisciplinary team including the primary care physician/endocrinologist, advanced practice provider, pharmacist, certified diabetes educator, nutritionist, and behavioral health professional.
Ongoing surveillance checklist (Table 416-1, Harrison's 22E):
| Domain | Frequency |
|---|---|
| HbA1c testing | 2-4 times/year |
| Continuous glucose monitoring (CGM) or fingerstick BG | Daily |
| Diabetes-related eye examination | Annual or biannual |
| Foot examination (by provider) | 1-2 times/year |
| Neuropathy examination | Annual |
| Kidney disease testing (urine albumin, eGFR) | Annual |
| Blood pressure assessment | 2-4 times/year |
| Lipid panel | 1-2 times/year |
| Psychosocial assessment (depression, anxiety, diabetes distress) | Ongoing |
| Immunizations (influenza, pneumococcal, hepatitis B, COVID-19) | Per schedule |
3. Glycemic Targets
The ADA recommends individualized glycemic goals based on patient status:
| Patient Group | HbA1c Target | CGM: Time in Range |
|---|---|---|
| Most adults (non-pregnant) | < 7.0% (53 mmol/mol) | > 70% within 3.9-10.0 mmol/L (70-180 mg/dL) |
| Elderly with intact cognition | < 7.0-7.5% | > 70% within 4.4-10.0 mmol/L |
| Elderly with serious comorbidities | < 8.0% | > 50% within 5.5-10.0 mmol/L |
| Elderly with complex comorbidities/poor cognition | < 8.5% (with hypoglycemia avoidance) | > 40% within 6.7-12.2 mmol/L |
| Some younger patients without hypoglycemia risk | ≤ 6.5% (more stringent) | - |
A higher HbA1c target is appropriate for those with cognitive impairment, reduced hypoglycemia awareness, or limited life expectancy. Fasting blood sugar targets: 90-130 mg/dL.
4. Lifestyle Management
Nutrition Therapy (Medical Nutrition Therapy - MNT)
- Type 1 DM: Focus on coordinating insulin administration with carbohydrate intake; carbohydrate counting is the standard approach
- Type 2 DM: Focus on weight loss (goal ≥5-10% body weight reduction), modest caloric reduction, increased physical activity
- Very-low-carbohydrate diets may produce rapid glucose lowering in new-onset T2DM
- High-fiber diets improve glycemic control
- For patients fasting during Ramadan: risk-stratify and adjust medications accordingly
Physical Activity
- 150 min/week of moderate aerobic activity distributed over at least 3 days (no gaps > 2 consecutive days)
- Resistance exercise, flexibility, and balance training are also advised
- Reduces blood pressure, improves insulin sensitivity, maintains muscle mass
- Type 1 DM caution: Monitor BG before, during, and after exercise; delay if BG > 14 mmol/L (250 mg/dL) with ketones; ingest carbohydrate if BG < 5.0 mmol/L (90 mg/dL) before exercise
Psychosocial Care
- Screen for depression, anxiety, and "diabetes distress"
- Patients should be active team members, not passive recipients of care
- Diabetes self-management education and support (DSMES) is a core component
5. Pharmacological Management
Type 2 DM - Treatment Algorithm
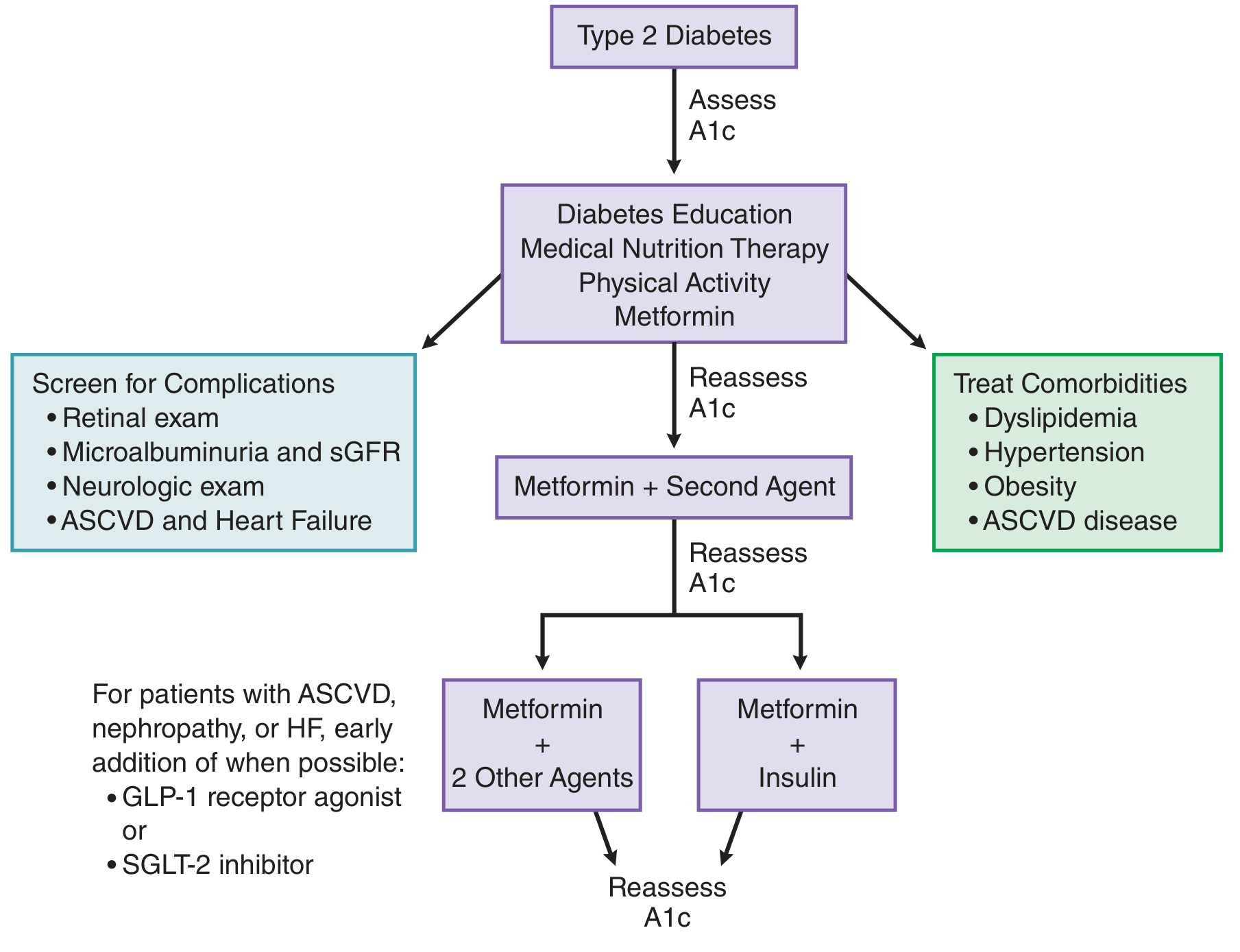
Step 1: Diabetes education + Medical Nutrition Therapy + Physical Activity + Metformin at diagnosis
Step 2: If HbA1c target not achieved in 2-3 months → add a second agent
Step 3: If still not at goal → Metformin + two additional agents OR Metformin + Insulin
Special consideration: In patients with established ASCVD, nephropathy, or heart failure, a GLP-1 receptor agonist or SGLT-2 inhibitor should be added early, even before the usual stepwise progression fails.
Oral and Injectable Agents for T2DM
| Drug Class | Examples | Mechanism | Key Notes |
|---|---|---|---|
| Biguanides | Metformin | Decreases hepatic glucose output, improves insulin sensitivity | First-line; no weight gain; no hypoglycemia; contraindicated with eGFR < 30; lowers BG ~100 mg/dL |
| Sulfonylureas | Glipizide, glyburide, glimepiride | Stimulate insulin secretion (close K-ATP channels) | Risk of hypoglycemia; weight gain; caution with renal disease |
| Thiazolidinediones (TZDs) | Pioglitazone | PPAR-γ agonist; reduce insulin resistance | Weight gain, fluid retention, increased fracture risk; CI in CHF |
| DPP-4 Inhibitors | Sitagliptin, saxagliptin | Inhibit DPP-4 → prolong GLP-1/GIP action | Weight neutral; generally well tolerated |
| GLP-1 Receptor Agonists | Liraglutide, semaglutide, dulaglutide | Stimulate glucose-dependent insulin secretion, suppress glucagon, slow gastric emptying | Weight loss; CV benefit (ASCVD, HF); injectable or oral; nausea common |
| SGLT-2 Inhibitors | Empagliflozin, canagliflozin, dapagliflozin | Block glucose reabsorption in kidney → glycosuria | CV and renal benefits; heart failure benefit; risk of UTI, DKA; avoid if eGFR low |
| Alpha-glucosidase inhibitors | Acarbose, miglitol | Delay carbohydrate absorption | Reduce postprandial glucose; GI side effects |
| Meglitinides (glinides) | Repaglinide, nateglinide | Short-acting insulin secretagogues | Taken with meals; flexible dosing |
| Colesevelam | Colesevelam | Bile acid sequestrant; reduces HbA1c ~0.5% | Constipation; raises triglycerides |
| Bromocriptine | Bromocriptine | Dopamine agonist; CNS mechanism | Modest effect; taken in morning |
| Amylin analogue | Pramlintide | Slows gastric emptying, suppresses glucagon | Adjunct to insulin; nausea; Type 1: 15-60 µg pre-meal; Type 2: 60-120 µg pre-meal |
The GRADE study found that addition of liraglutide or basal insulin to metformin provides slightly better glycemic control than glimepiride or sitagliptin as a second agent.
Insulin Therapy
Insulin is required for Type 1 DM and often becomes necessary in Type 2 DM as beta-cell function declines over time (approximately 50% of T2DM patients need a second drug after 3 years on monotherapy).
Insulin preparations:
| Type | Examples | Onset | Peak | Duration |
|---|---|---|---|---|
| Rapid-acting (injected) | Aspart, lispro, glulisine | < 15 min | 0.5-1.5 h | 3-5 h |
| Rapid-acting (inhaled) | Inhaled human insulin | < 15 min | 1-2 h | 3 h |
| Short-acting | Regular | 0.5-1 h | 2-3 h | 4-8 h |
| Intermediate | NPH | 2-4 h | 4-10 h | 10-16 h |
| Long-acting | Glargine | 2-4 h | Flat | 20-24 h |
| Ultra-long-acting | Degludec | 1-9 h | Flat | ~42 h |
Starting basal insulin in T2DM: 10 units/day of glargine or detemir (or 0.1-0.2 units/kg once daily), titrate by 1-3 units every 1-3 days targeting FBG 90-130 mg/dL and HbA1c < 6.5-7%.
Intensive Type 1 management uses MDI (multiple daily injections) or CSII (insulin pump/AID system). Automated Insulin Delivery (AID) is the preferred delivery method, combining a pump, CGM, and algorithm to modulate basal rates automatically. Hybrid closed-loop systems are rapidly expanding.
6. Glucose Monitoring
- CGM is preferred over fingerstick glucose for most patients, especially Type 1 DM
- Real-time CGM provides glucose readings every 5 minutes, reduces hypoglycemia, and improves glycemic control
- CGM metrics (Time in Range, Time Below Range) are now incorporated into glycemic targets alongside HbA1c
7. Acute Hyperglycemic Emergencies
Diabetic Ketoacidosis (DKA)
- Primarily Type 1 DM; can occur in T2DM with SGLT-2 inhibitor use (often euglycemic DKA)
- Features: nausea/vomiting, abdominal pain, Kussmaul respirations, fruity breath, dehydration, elevated ketones
- Measure beta-hydroxybutyrate (preferred over urine ketones)
- Treatment: IV fluid resuscitation, insulin infusion, electrolyte replacement (especially K+), identify precipitant
Hyperglycemic Hyperosmolar State (HHS)
- Primarily Type 2 DM
- Features: extreme hyperglycemia, hyperosmolality, severe dehydration, no significant ketosis or acidosis
- Higher mortality than DKA; management is aggressive hydration + insulin
8. Management of DM Complications & Comorbidities
| Condition | Target / Intervention |
|---|---|
| Hypertension | BP < 130/80 mmHg; ACE inhibitors/ARBs preferred (especially with proteinuria) |
| Dyslipidemia | Statin therapy; LDL-C target depends on CV risk |
| ASCVD | GLP-1 RA or SGLT-2 inhibitor preferred add-on; low-dose aspirin per guidelines |
| Diabetic kidney disease | ACE/ARB + SGLT-2 inhibitor; monitor eGFR and urine albumin |
| Heart failure | SGLT-2 inhibitor (proven mortality benefit with empagliflozin, canagliflozin) |
| Neuropathy | Glycemic control; pregabalin, duloxetine, or tricyclics for pain |
| Retinopathy | Annual eye exam; referral to ophthalmology; strict glycemic and BP control |
| Foot care | Daily patient self-exam; annual provider exam; podiatrist referral if needed |
9. Special Populations
- Elderly: Individualize HbA1c targets; prioritize avoiding hypoglycemia over tight control in frail patients
- Pregnant/Gestational DM: Tight control (HbA1c 6-7%); insulin preferred; oral agents have limited evidence in some guidelines
- Chronic kidney disease: Avoid metformin if eGFR < 30; adjust SGLT-2 inhibitor dosing; insulin often required
- Hospitalized patients: Insulin is the preferred agent; target BG 140-180 mg/dL; avoid hypoglycemia
10. Emerging Therapies
- Anti-CD3 monoclonal antibodies (teplizumab): FDA-approved to delay Stage 3 Type 1 DM onset in high-risk individuals (Stage 2)
- Artificial pancreas / bionic pancreas: Bihormonal (insulin + glucagon) closed-loop devices being tested; show improved mean glucose with fewer hypoglycemic episodes
- Immunomodulatory approaches targeting TXNIP and beta-cell preservation in Type 1 DM are under investigation
Key clinical principle: Management is highly individualized. Shared decision-making incorporating patient preferences, comorbidities, financial resources, and social determinants of health should guide every treatment decision.
Sources: Harrison's Principles of Internal Medicine 22E (2025), Chap. 416; Goodman & Gilman's Pharmacological Basis of Therapeutics, Chap. 51; Rosen's Emergency Medicine, Chap. 115
This is a shared conversation. Sign in to Orris to start your own chat.