Peptic ulcer in very detail with reference to standard textbooks
Reading File
Finding Sources
Finding Sources
Searching PubMed
"peptic ulcer"[MeSH Terms] AND "Helicobacter pylori"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive material from all major textbooks. Let me compile the definitive, detailed answer.
Peptic Ulcer Disease - A Comprehensive Review
Based on: Robbins & Cotran Pathologic Basis of Disease (10th ed), Robbins & Kumar Basic Pathology, Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Schwartz's Principles of Surgery (11th ed), Bailey & Love's Short Practice of Surgery (28th ed), Guyton & Hall Textbook of Medical Physiology, Yamada's Textbook of Gastroenterology (7th ed)
1. Definition
Peptic ulcer disease (PUD) refers to chronic mucosal ulcerations involving the stomach or duodenum that extend through the muscularis mucosae into the submucosa or deeper, caused by an imbalance between mucosal defense mechanisms and aggressive acid-peptic forces. The term "peptic" implies dependence on acid and pepsin - but notably, in the complete absence of acid, peptic ulcers do not form, and virtually all benign ulcers heal with proton pump inhibitor (PPI) therapy that renders the patient nearly achlorhydric.
- Bailey & Love's Short Practice of Surgery, 28th Ed.
- Guyton & Hall Textbook of Medical Physiology
2. Epidemiology
-
PUD is one of the most common GI disorders worldwide. In the United States, prevalence is approximately 2% with a lifetime cumulative risk of ~10% for males and ~4% for females, peaking around age 70.
-
More than 4 million individuals in the US are treated for PUD each year.
-
Costs (including lost work and productivity) exceed $8 billion/year in the US.
-
The incidence of PUD is falling as H. pylori infection rates decrease, but PUD in patients over 60 years has increased due to growing NSAID use.
-
Duodenal ulcers (DU) are more common than gastric ulcers (GU). DU has a male predominance; GU has an equal gender incidence.
-
GU patients tend to be older and are more prevalent in low socioeconomic groups and resource-poor countries.
-
Robbins & Cotran Pathologic Basis of Disease, p. 719
-
Schwartz's Principles of Surgery, 11th Ed., p. 1148
3. Etiology and Risk Factors
Primary Causes
| Cause | Contribution |
|---|---|
| H. pylori infection | >70% of all PUD; >90% of DU |
| NSAIDs/aspirin | Rising cause, especially in the elderly; predominant cause of GU in developed countries |
| Zollinger-Ellison syndrome (gastrinoma) | Rare; massive hypergastrinemia and acid hypersecretion |
Other Risk Factors
- Cigarette smoking - reduces mucosal blood flow and healing; reduces mucosal prostaglandin synthesis
- High-dose corticosteroids - suppress prostaglandin synthesis, impair healing
- Alcohol-related cirrhosis
- Chronic obstructive pulmonary disease (COPD)
- Chronic renal failure and hyperparathyroidism - hypercalcemia stimulates gastrin production and acid secretion
- Cocaine use
- Blood group O - GWAS studies confirmed the long-reported epidemiological link between O blood type and DU (the risk allele at ABO locus [rs505922] provides a molecular basis)
- Psychological stress - particularly physiological stress (trauma, burns, ICU patients)
- Genetic factors - a Finnish twin study estimated 39% of liability for PUD is explained by genetic factors; GWAS identified loci on chromosome 8q24 (PSCA gene) and 9q34 (ABO)
"In the United States, probably more than 90% of serious peptic ulcer complications can be attributed to H. pylori infection, NSAID use, and/or cigarette smoking."
- Schwartz's Principles of Surgery, 11th Ed., p. 1149
- Yamada's Textbook of Gastroenterology, 7th Ed.
- Robbins & Kumar Basic Pathology
4. Pathophysiology
The final common pathway to ulcer formation is acid-peptic injury of the gastroduodenal mucosal barrier - a result of an imbalance between aggressive and defensive factors.
Aggressive Factors
- Hydrochloric acid (HCl)
- Pepsin
- H. pylori and its virulence factors
- NSAIDs (COX inhibition)
- Bile acids (in gastric reflux)
Defensive Factors
-
Mucus-bicarbonate barrier (mucous cells, Brunner's glands)
-
Mucosal blood flow (provides bicarbonate, removes acid, supports healing)
-
Epithelial tight junctions and cell renewal
-
Prostaglandins (stimulate mucus, bicarbonate, blood flow; inhibited by NSAIDs)
-
Duodenal neutralization by pancreatic bicarbonate
-
Secretin feedback (acid in duodenum stimulates secretin → pancreatic bicarbonate)
-
Neural feedback (acid in duodenum inhibits gastric acid secretion and peristalsis)
-
Guyton & Hall Textbook of Medical Physiology, p. 825
Role of Helicobacter pylori
H. pylori is a gram-negative spiral bacterium that colonizes beneath the mucous layer overlying gastric epithelium. Its pathogenetic mechanisms include:
- Urease production - converts urea to NH₃ and CO₂; ammonia is directly cytotoxic and buffers the local environment, allowing bacterial survival at low pH
- VacA (vacuolating cytotoxin A) - induces vacuolation and cell death in epithelial cells
- CagA (cytotoxin-associated gene A) - encoded on the cag pathogenicity island (PAI); delivered via a type IV secretion system into host cells; activates NF-κB, induces IL-8, promotes inflammation and mucosal injury
- Lipopolysaccharide (LPS) - triggers innate immune responses and PMN infiltration
- Acid hypersecretion - H. pylori antral gastritis impairs somatostatin secretion by D cells → reduced inhibition of gastrin → elevated gastrin → increased parietal cell acid output
- Decreased duodenal bicarbonate secretion - contributes to loss of buffering
- Only 5-10% of infected individuals develop ulcers, indicating that host genetic factors and bacterial strain pathogenicity (cagA-positive strains) both play a role
- Schwartz's Principles of Surgery, 11th Ed., pp. 1145-1147
- Robbins & Cotran Pathologic Basis of Disease, pp. 718-720
Role of NSAIDs
NSAIDs cause ulcers primarily by compromising mucosal defenses:
- Inhibit COX-1 and COX-2 → reduce prostaglandin synthesis → decrease mucus and bicarbonate secretion, reduce mucosal blood flow
- Topical (direct) injury - many NSAIDs are weak acids that penetrate mucosal cells at low gastric pH, leading to cell damage
- COX-2-selective inhibitors (celecoxib) reduce but do not eliminate GI risk
- H. pylori infection interacts with NSAIDs/aspirin to amplify mucosal injury
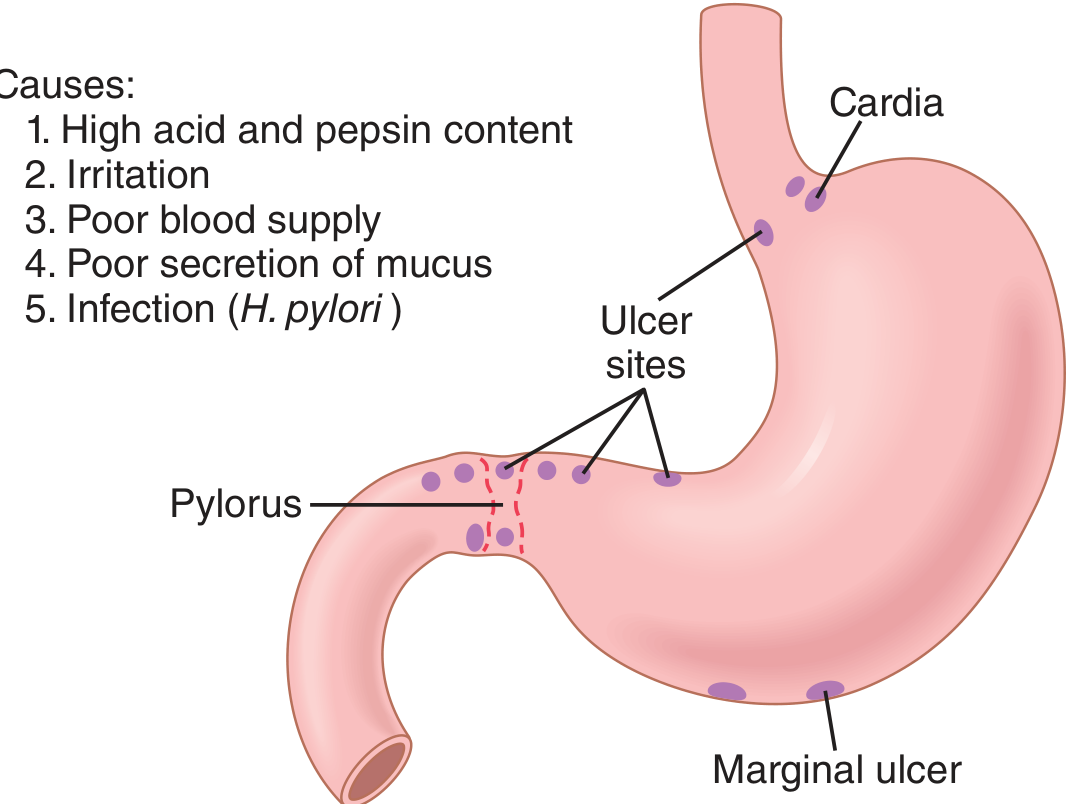
5. Sites
All PUD occurs in areas exposed to gastric juice, but localization follows a pattern:
- Duodenum - Most common site; first part (D1) within 2 cm of pylorus; "kissing ulcers" (anterior + posterior walls) occur
- Stomach - Lesser curve (especially at the incisura angularis); gastric antrum-body junction; high lesser curve ulcers occur with proximal migration of the antral-body junction due to parietal cell atrophy
- Gastroesophageal junction - Lower esophagus in GERD or Barrett's epithelium
- Meckel's diverticulum - When ectopic gastric mucosa is present
- Stomal/marginal ulcer - At gastrojejunostomy sites after gastric surgery (usually at jejunal/gastric mucosa junction)
- Zollinger-Ellison - Multiple ulcers in stomach, duodenum, and even jejunum
"In general, the ulcer occurs at a junction between different types of epithelia, in the epithelium least resistant to acid damage."
- Bailey & Love's Short Practice of Surgery, 28th Ed., p. 1174
6. Pathology (Morphology)
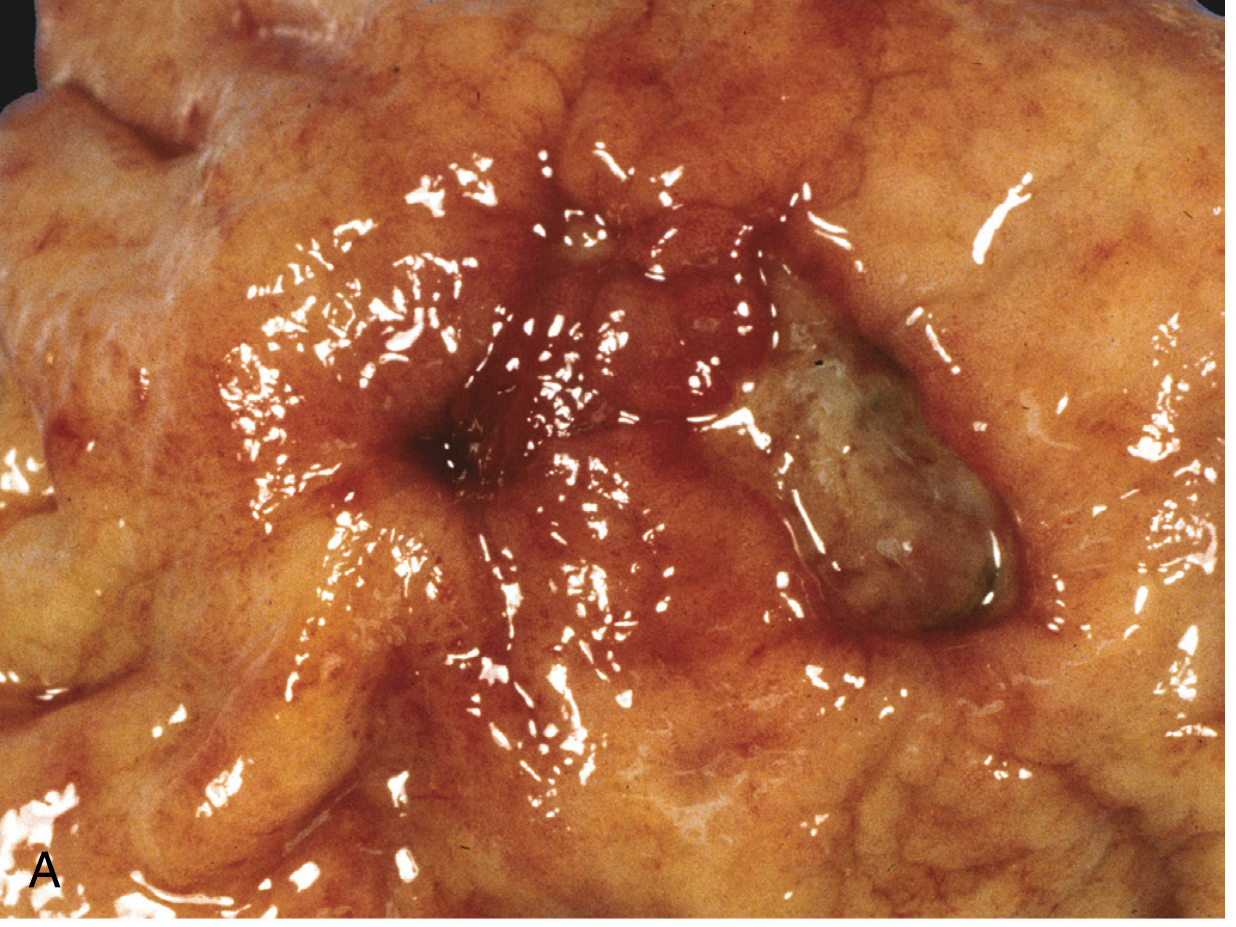
Macroscopic Features
- Solitary in >80% of patients
- Round to oval, sharply punched-out defect with a "clean" base (peptic digestion of exudate)
- Mucosal margin is level with surrounding mucosa (unlike cancers, which have heaped-up, irregular margins)
- Size - typically <2 cm; GU tend to be larger than DU
- Folds radiate outward from the ulcer base (due to submucosal scarring)
- In chronic cases, fibrosis may produce "hourglass" deformity of the stomach
Microscopic Features (4 Zones from surface to base)
- Zone of fibrinoid necrosis - thin layer at the surface; neutrophilic infiltrate
- Zone of active nonspecific cellular infiltration - mononuclear cells, neutrophils
- Zone of granulation tissue - immature vessels, fibroblasts
- Zone of fibrosis/scar - collagenous tissue extending into the muscularis propria
-
Endarteritis obliterans may be present at the base
-
Larger vessels in the scarred area are thickened and occasionally thrombosed - erosion into these causes hemorrhage
-
Foveolar (gastric-type) metaplasia is common in chronic duodenal peptic disease - a protective response, as gastric epithelium is more acid-resistant than intestinal epithelium
-
Robbins & Cotran Pathologic Basis of Disease, pp. 719-720
-
Robbins & Kumar Basic Pathology
-
Bailey & Love's Short Practice of Surgery, 28th Ed.
7. Clinical Features
Symptoms
Duodenal Ulcer (DU):
- Epigastric burning/gnawing pain, typically 2-3 hours after meals (pain when stomach is empty)
- Pain relieved by food or antacids
- Nocturnal pain (waking 1-3 AM) - highly characteristic; due to peak acid secretion during sleep
- Weight gain (eating relieves pain) or normal weight
Gastric Ulcer (GU):
- Epigastric pain, often precipitated or worsened by eating
- Nausea, anorexia, vomiting
- Weight loss (due to food aversion)
- Symptoms of DU and GU are often clinically indistinguishable
Alarm Features (Indicate Urgent Endoscopy)
-
Dysphagia/odynophagia
-
Unexplained weight loss
-
Hematemesis or melena
-
Palpable abdominal mass or lymphadenopathy
-
Iron deficiency anemia
-
Persistent vomiting
-
Age >55 with recent onset of symptoms
-
Family history of upper GI cancer
-
Schwartz's Principles of Surgery, 11th Ed., p. 1142-1143
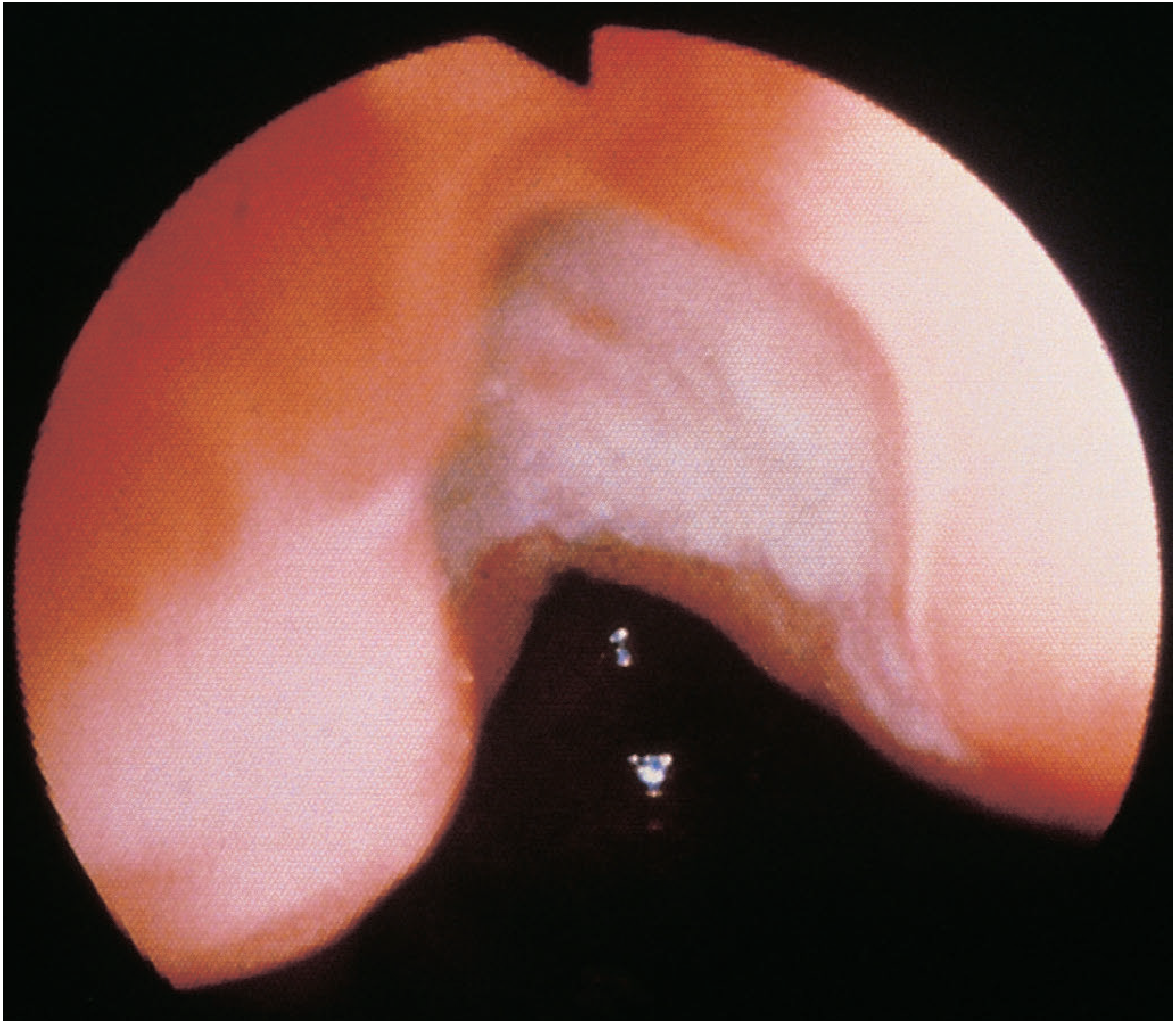
8. Investigations
Endoscopy (EGD - Gold Standard)
- Directly visualizes the ulcer; assesses size, location, active bleeding
- All gastric ulcers require multiple biopsies (base and rim) to exclude malignancy
- Antral biopsies for histology and CLO (Campylobacter-like organism/urease) test
- Brush cytology for gastric ulcers
- Follow-up endoscopy at 6-8 weeks for gastric ulcers to confirm healing
Tests for H. pylori
| Test | Sensitivity | Specificity | Notes |
|---|---|---|---|
| CLO/Rapid urease test (biopsy) | 90-95% | 95-100% | Requires endoscopy; affected by PPIs, antibiotics |
| Histology (biopsy) | 95% | 99% | Gold standard; shows bacteria in mucus layer |
| Urea breath test (UBT) | 95% | 95% | Best non-invasive test; confirms eradication |
| Stool antigen test | 94% | 97% | Good for diagnosis and post-treatment confirmation |
| Serology | 85% | 79% | Remains positive after eradication; not useful for confirming cure |
Radiology
-
Erect chest X-ray - free gas under diaphragm in perforation (seen in >50%)
-
Barium upper GI series - double-contrast; shows "niche" sign for DU; radiating folds toward GU crater
-
CT scan - preferred for suspected perforation; more sensitive than erect CXR; differentiates from pancreatitis
-
Serum gastrin - check if unusual ulcer location (distal DU, jejunal), H. pylori-negative, NSAID-negative, or multiple ulcers (to rule out ZES)
-
Schwartz's Principles of Surgery, 11th Ed., p. 1143
-
Bailey & Love's Short Practice of Surgery, 28th Ed.
9. Medical Treatment
Step 1: Test and Treat for H. pylori
All patients with confirmed PUD should be tested for H. pylori. If positive, eradication dramatically reduces recurrence (from ~60-80% at 1 year to <5%).
Standard Triple Therapy (14 days, first-line in low-resistance areas):
- PPI (standard dose twice daily) + Clarithromycin 500 mg BD + Amoxicillin 1 g BD
Bismuth Quadruple Therapy (14 days, preferred in areas with high clarithromycin resistance):
- PPI BD + Bismuth subcitrate QDS + Metronidazole 400 mg QDS + Tetracycline 500 mg QDS
Concomitant Quadruple Therapy (no bismuth):
-
PPI BD + Clarithromycin + Amoxicillin + Metronidazole (all twice daily)
-
Eradication should be confirmed 4-6 weeks after completion of therapy using UBT or stool antigen (PPIs should be stopped 2 weeks prior)
-
Failure after two courses warrants culture and sensitivity testing and specialist referral
-
The Maastricht V/Florence Consensus guidelines provide current recommendations stratified by regional resistance patterns
"H. pylori eradication can be achieved in nearly every patient with assiduous treatment."
- Schwartz's Principles of Surgery, 11th Ed., p. 1147
Step 2: Acid Suppression
- PPIs (omeprazole, lansoprazole, esomeprazole) - render patient effectively achlorhydric; heal all benign ulcers, the majority within 2 weeks; symptom relief within days
- DU: 4 weeks; GU: 6-8 weeks
- H₂-receptor antagonists (ranitidine, famotidine) - historically important; effective but slower than PPIs; still used in some settings
- All gastric antisecretory agents have a high relapse rate once stopped (unless H. pylori eradicated)
Step 3: NSAID Management
- Stop NSAID if possible
- If NSAID must be continued: use lowest effective dose, add PPI; consider switching to a COX-2-selective inhibitor
- Misoprostol (prostaglandin E₁ analogue) at 200 µg QDS effectively reduces NSAID-induced ulcers (MUCOSA trial: clinical UGI events halved); limited by GI side effects (diarrhea)
Lifestyle Modifications
- Stop smoking (impairs mucosal blood flow and healing)
- Avoid known NSAIDs/aspirin unless essential
- Dietary modifications (avoid personal trigger foods)
10. Complications and Their Management
10.1 Hemorrhage (Most Common Complication)
- Most common serious complication; most peptic ulcer-related deaths are from bleeding
- Presents with hematemesis, melena, or hematochezia (massive bleed)
- Posterior DU - erosion into the gastroduodenal artery; risk of life-threatening hemorrhage
Assessment:
- Rockall Score (pre- and post-endoscopy): integrates age, comorbidity, diagnosis, endoscopic stigmata
- Score 0-2: low risk (mortality <1%); score ≥8: mortality 41%
- AIMS65 score (Albumin <3, INR >1.5, altered Mental status, Systolic BP <90, age ≥65): predicts in-hospital mortality
Endoscopic Stigmata (Forrest Classification):
| Class | Finding | Rebleed Risk |
|---|---|---|
| Ia | Active spurting | 55-90% |
| Ib | Active oozing | 30-50% |
| IIa | Non-bleeding visible vessel | 43-55% |
| IIb | Adherent clot | 22-36% |
| IIc | Flat pigmented spot | 7-10% |
| III | Clean base | <5% |
Management:
-
Resuscitation (blood transfusion; target Hb ~7-9 g/dL unless cardiovascular disease)
-
High-dose IV PPI (bolus + infusion): reduces rebleeding; no acid = stable clot
-
Endoscopic hemostasis - injection (epinephrine), thermal coagulation (heater probe, APC), or mechanical (clips); most (75%) stop with conservative management
-
Endoscopic re-treatment for rebleeding
-
Surgery (if endoscopic hemostasis fails twice): underrunning the bleeding vessel (DU); Billroth I/II gastrectomy for GU
-
Sleisenger & Fordtran's Gastrointestinal and Liver Disease (Rockall score table)
-
Schwartz's Principles of Surgery, 11th Ed., p. 1131
10.2 Perforation
- Incidence has changed little despite widespread PPI/eradication use
- Now predominantly affects elderly females on NSAIDs
- Most commonly: anterior DU perforating into the peritoneal cavity; posterior ulcers erode (penetrate) into the pancreas
Clinical Features:
- Sudden-onset severe generalized abdominal pain - instantaneously recognized
- Board-like (peritonitic) rigidity; abdomen immobile with respiration
- Shock, tachycardia; pyrexia develops hours later (bacterial peritonitis)
- Fluid may track to right iliac fossa mimicking appendicitis
- Atypical presentation in elderly (steroids blunt signs): higher index of suspicion required
Investigations:
- Erect CXR - free gas under diaphragm (>50% of cases)
- CT abdomen - most accurate; also rules out pancreatitis; serum amylase can be elevated in both (though usually lower in PUD perforation)
- ECG (to exclude inferior MI presenting as acute abdomen)
Management:
-
Resuscitation + analgesia (adequate analgesia does NOT mask signs; it actually clarifies them)
-
NG tube decompression, IV fluids, antibiotics
-
Surgery - upper midline laparotomy (or laparoscopic approach); Graham patch repair (omental patch closure); add H. pylori eradication and PPI post-operatively
-
Conservative management (Taylor's method: NG suction, IV PPIs, antibiotics) may be considered in carefully selected stable patients where perforation may have sealed spontaneously
-
Bailey & Love's Short Practice of Surgery, 28th Ed., pp. 1186-1188
-
Schwartz's Principles of Surgery, 11th Ed., p. 1134
10.3 Gastric Outlet Obstruction (Pyloric Stenosis)
-
Most commonly associated with longstanding PUD and gastric cancer
-
Results from chronic scarring/fibrosis at the pyloric channel or D1
-
Presents with: repeated vomiting of undigested food, distension, succussion splash, weight loss
-
Metabolic abnormality: hypochloremic hypokalemic metabolic alkalosis (loss of HCl and K+ in vomit); distinct from cancer-related obstruction (which lacks this pattern)
-
Management: fluid/electrolyte correction; endoscopic balloon dilatation (first-line); surgery (antrectomy with gastrojejunostomy or Billroth II) if dilatation fails or cancer excluded
-
Bailey & Love's Short Practice of Surgery, 28th Ed., p. 1190 (Summary Box)
10.4 Malignant Transformation
-
Duodenal ulcers do NOT undergo malignant transformation
-
Gastric ulcers: Two scenarios
- Benign chronic gastric ulcer undergoes malignant transformation - rare
- An ulcer assessed endoscopically as benign proves on biopsy to be malignant - more common; hence all gastric ulcers must be biopsied
-
The underlying risk: H. pylori → chronic gastritis → atrophy → intestinal metaplasia → dysplasia → adenocarcinoma (Correa cascade)
-
Bailey & Love's Short Practice of Surgery, 28th Ed.
10.5 Penetration
- Posterior gastric/DU erodes into adjacent structures without free perforation:
- Posterior DU → pancreas (causes pancreatitis; amylase rises)
- Gastric ulcer → splenic artery (risk of hemorrhage), transverse colon (gastrocolic fistula)
- Pain becomes constant, radiates to the back; loses meal periodicity
11. Surgical Treatment
Surgery for uncomplicated PUD has markedly decreased and is now seldom performed (medical and eradication therapy has supplanted it). Surgery is reserved for complications (perforation, uncontrolled hemorrhage, obstruction refractory to endoscopy/dilatation).
Historic Surgical Procedures (now rarely for elective use)
| Operation | Operative Mortality | Side Effects | Recurrence |
|---|---|---|---|
| Gastrectomy | 1-2% | 20-40% | 1-4% |
| Gastroenterostomy alone | <1% | 10-20% | 50% |
| Truncal vagotomy + drainage | <1% | 10-20% | 2-7% |
| Selective vagotomy + drainage | <1% | 10-20% | 5-10% |
| Highly selective vagotomy | <0.2% | <5% | 2-10% |
| Truncal vagotomy + antrectomy | 1% | 10-20% | 1% (lowest recurrence) |
- Bailey & Love's Short Practice of Surgery, 28th Ed., Table 67.2
Post-Gastrectomy Syndromes (~30% of patients)
- Early dumping (20-30 min post-prandially): hyperosmolar chyme dumps into small intestine → fluid shifts → vasomotor symptoms (flushing, palpitations, dizziness) + GI symptoms (cramps, diarrhea)
- Late dumping (1-3 hours post-prandially): hypoglycemia secondary to reactive insulin surge
- Bilious vomiting/bile reflux gastritis
- Small stomach syndrome: early satiety, weight loss
- Diarrhea (especially post vagotomy)
- Malnutrition/malabsorption: iron, B12, folate deficiency; post-gastrectomy osteoporosis (calcium malabsorption)
- Malignant transformation: increased gastric remnant cancer risk after Billroth II
12. Special Situations
Zollinger-Ellison Syndrome (ZES)
- Gastrin-secreting tumor (gastrinoma), usually in the duodenum or pancreas (the "gastrinoma triangle")
- 25% associated with MEN-1
- Massive acid hypersecretion → multiple ulcers in atypical locations (distal duodenum, jejunum), refractory to standard treatment
- Diagnosis: fasting serum gastrin >1000 pg/mL (diagnostic) or secretin stimulation test (paradoxical gastrin rise >200 pg/mL)
- Treatment: high-dose PPI; surgical resection; octreotide for metastatic disease
NSAID-Induced Ulcer Prevention
- COX-2 inhibitors + PPI: most effective prophylaxis in high-risk patients
- Misoprostol: effective but poorly tolerated
PUD in Pregnancy
- Covered briefly by Creasy & Resnik; PPIs (omeprazole) generally safe; avoid misoprostol (uterotonic); H. pylori eradication may be deferred post-partum
13. H. pylori Eradication - Indications (ACG Guidelines)
Established indications:
- Active peptic ulcer disease (gastric or duodenal)
- Confirmed history of PUD not previously treated for H. pylori
- Gastric MALT lymphoma (low grade)
- After endoscopic resection of early gastric cancer
- Uninvestigated dyspepsia (depending on prevalence)
Controversial:
-
Nonulcer dyspepsia
-
GERD
-
Persons using NSAIDs
-
Unexplained iron deficiency anemia
-
Populations at higher risk for gastric cancer
-
Schwartz's Principles of Surgery, 11th Ed., Table 26-8
14. Summary (Key Points)
| Feature | Duodenal Ulcer | Gastric Ulcer |
|---|---|---|
| Frequency | More common | Less common |
| Location | D1, within 2 cm of pylorus | Lesser curve, incisura angularis |
| Age | Younger | Older |
| Gender | Male > Female | Equal |
| Acid secretion | Increased (usually) | Normal or decreased |
| H. pylori association | >90% | 70% |
| Malignant potential | None | Yes (biopsy all GU) |
| Pain timing | 2-3 h after meals, relieved by food | Precipitated by food |
| Weight | Gain or normal | Loss |
| Follow-up endoscopy | Not routinely needed | Mandatory (6-8 weeks) |
Recent Evidence (PubMed, 2024-2026)
- A 2025 systematic review and meta-analysis (PMID: 40281437) reported on the prevalence and patterns of PUD across Africa, noting high H. pylori rates as a dominant etiological driver in that region.
- A 2026 systematic review (PMID: 41236450) in Gastroenterology quantified the broader disease burden of H. pylori beyond gastric cancer, strengthening the evidence for mass eradication strategies to reduce PUD burden globally.
References:
- Robbins & Cotran Pathologic Basis of Disease, 10th Ed. (Kumar et al.), pp. 718-720
- Robbins & Kumar Basic Pathology, pp. 3903-3910
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease, pp. 305+
- Schwartz's Principles of Surgery, 11th Ed., pp. 1125-1136, 1143-1152
- Bailey & Love's Short Practice of Surgery, 28th Ed., pp. 1174-1190
- Guyton & Hall Textbook of Medical Physiology, pp. 825-828
- Yamada's Textbook of Gastroenterology, 7th Ed., Chapter 49
This is a shared conversation. Sign in to Orris to start your own chat.