A 25 year old intern complaints of throat pain . How to manage
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pharyngitis" AND "management"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive, well-structured answer. Here it is:
Management of Sore Throat in a 25-Year-Old
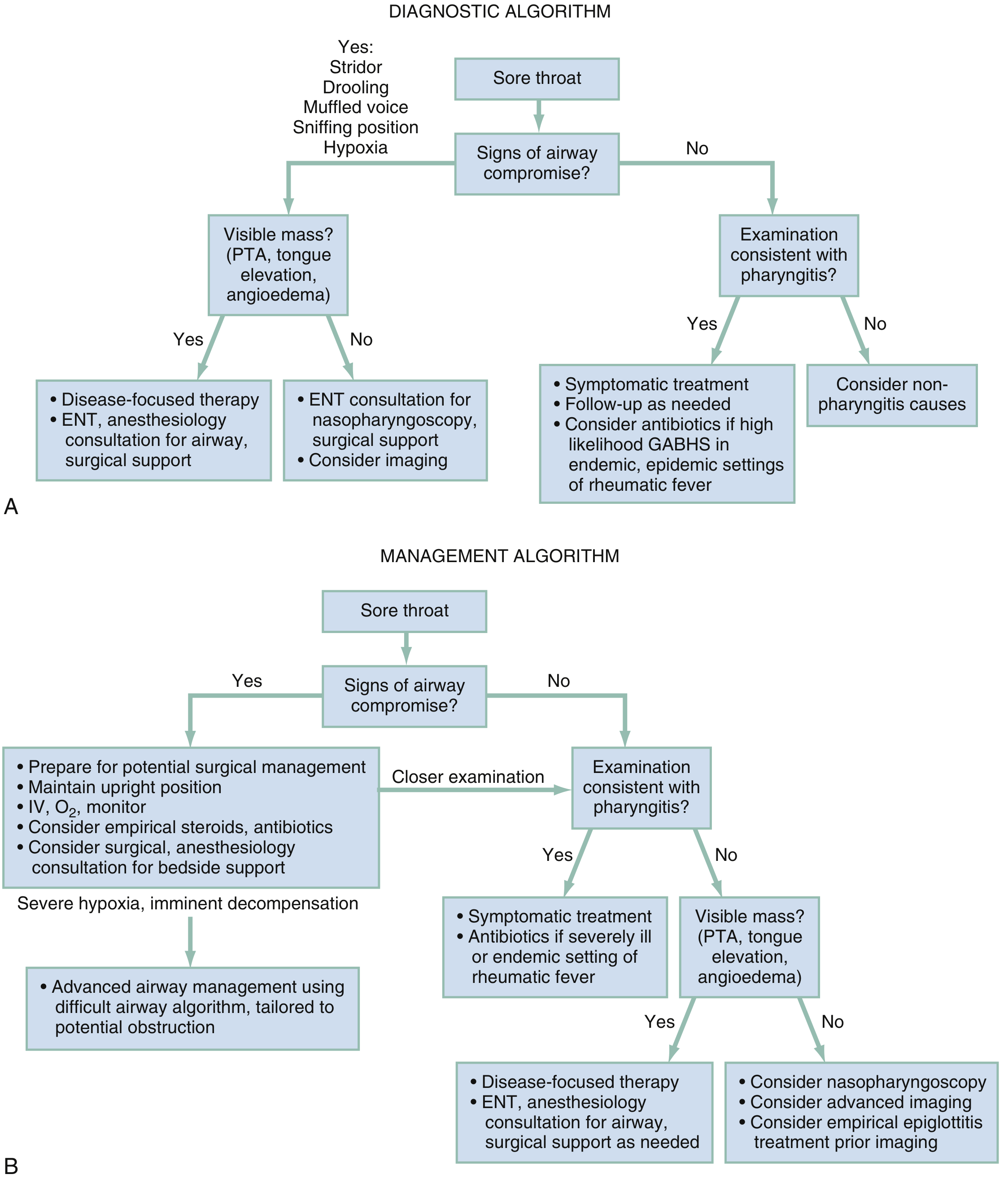
Step 1 - Rule Out Airway Emergency First
Before anything else, assess for signs of airway compromise:
| Red Flag Sign | Suggests |
|---|---|
| Stridor, drooling, muffled/"hot potato" voice | Epiglottitis |
| Sniffing position, hypoxia | Supraglottic obstruction |
| Trismus, unilateral tonsillar bulge, uvular deviation | Peritonsillar abscess (PTA) |
| Neck rigidity, bilateral swelling | Retropharyngeal/parapharyngeal abscess |
If any of these are present: upright positioning, IV access, O₂ monitoring, ENT/anesthesia consult, and prepare for advanced airway. Do not proceed to routine workup.
Step 2 - Identify the Likely Cause
The two most common causes in a 25-year-old are viral pharyngitis (~90%) and Group A Streptococcus (GAS) pharyngitis (~10% of adults).
Use the Centor Score to Risk-Stratify for GAS
Each feature scores 1 point:
- History of fever
- Absence of cough
- Tender anterior cervical lymphadenopathy
- Tonsillar exudate or swelling
| Score | GAS Probability | Action |
|---|---|---|
| 0 | ~2% | No testing, no antibiotics |
| 1-2 | ~5-17% | Rapid antigen test (RADT) if warranted |
| 3-4 | ~28-41% | Test and treat if positive; consider empiric Rx at score 4 |
Note: As a healthcare worker/intern, GAS risk is slightly elevated due to patient exposure. - Harrison's Principles of Internal Medicine 22E
Clues to Specific Non-Strep Causes
| Clinical Finding | Consider |
|---|---|
| Posterior cervical adenopathy, splenomegaly, petechiae on palate | Infectious mononucleosis (EBV) - common 15-35 yrs |
| Fever, rash, myalgia, new sexual partner | Acute HIV infection |
| Persistent sore throat unresponsive to penicillin, sexual risk | Gonorrhea (N. gonorrhoeae) |
| Persistent symptoms + cough | Mycoplasma pneumoniae |
Step 3 - Treatment
A. All patients with pharyngitis (regardless of cause)
- Analgesics (first-line for symptom relief): Paracetamol (acetaminophen) or NSAIDs (ibuprofen) - take around-the-clock, not just as needed, for better symptom control
- Supportive measures: Saline gargles, humidification, soft foods, tea with honey, adequate hydration
- Avoid antibiotics for viral pharyngitis - no benefit, increases resistance and adverse effects
B. Corticosteroids (for severe pharyngitis with significant dysphagia)
- Single dose dexamethasone 0.6 mg/kg (max 10 mg) orally or IM
- Reduces pain and duration in patients with marked swelling
- Not routinely recommended for uncomplicated pharyngitis by IDSA guidelines
- Harrison's notes caution: even short steroid courses carry risks of sepsis, GI bleeding, VTE within 30 days
C. Antibiotic therapy - ONLY if GAS confirmed or high clinical suspicion
First-line (no penicillin allergy):
| Drug | Dose |
|---|---|
| Penicillin V (oral) | 500 mg QID or 1000 mg BID x 10 days |
| Amoxicillin (oral) | 500 mg BID or 1000 mg OD x 10 days |
| Benzathine Penicillin G (IM) | Single dose |
Penicillin-allergic (non-anaphylactic):
- Cephalexin or cefadroxil (10-day course)
Penicillin-allergic (anaphylactic):
- Erythromycin, clarithromycin, or clindamycin
GAS has never developed resistance to penicillin. Shorter antibiotic courses are less effective for GAS - a full 7-10 days is required. - Harrison's 22E
Step 4 - When to Escalate / Refer
- Fluctuant peritonsillar mass - drain (ENT referral); peritonsillar abscess requires I&D as definitive treatment
- Symptoms persisting >5 days without improvement
- Shaking chills/rigors, neck swelling beyond lymphadenopathy, trouble swallowing, drooling
- Severe systemic illness: IV clindamycin (900 mg TID) + ceftriaxone (1g q24h) empirically, with ENT consult
- Suspected epiglottitis or deep space neck infection: imaging (CT neck with contrast) + ENT/anesthesia emergently
Summary for This Intern
Since he is 25 with no stated alarm signs, the most likely diagnosis is viral pharyngitis. The management is:
- Calculate Centor score on examination
- If Centor 0-2: symptomatic treatment only (NSAIDs/paracetamol), no antibiotics, reassure
- If Centor 3-4: perform Rapid Antigen Test; treat with Penicillin V x 10 days if positive
- Consider mono (EBV) if posterior lymphadenopathy or splenomegaly - do a monospot test; never prescribe amoxicillin/ampicillin in suspected mono (causes maculopapular rash)
- Advise rest, fluids, return if worsening or no improvement by day 5
Sources: Rosen's Emergency Medicine (9th ed.), p. 235-236; Harrison's Principles of Internal Medicine 22E (2025), pp. from Chapter 37 (Streptococcal Pharyngitis section)
This is a shared conversation. Sign in to Orris to start your own chat.