Easy explanation and important points of Shoulder joint biomechanics for exam point of view
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the complete exam-focused answer.
Shoulder Joint Biomechanics - Exam Study Guide
Sources: Gray's Anatomy for Students | Miller's Review of Orthopaedics 9th Ed | Rheumatology (Elsevier 2022)
1. The Shoulder Complex - Overview
The shoulder is NOT a single joint. It is a complex of 4 joints that work together:
| Joint | Type |
|---|---|
| Glenohumeral (GHJ) | Ball & socket (synovial, multiaxial) - main joint |
| Acromioclavicular (ACJ) | Plane synovial joint |
| Sternoclavicular (SCJ) | Diarthrodial saddle joint (only bony link of UL to trunk) |
| Scapulothoracic (STJ) | Physiological (not a true anatomical joint) |
Exam tip: The shoulder sacrifices bony stability for maximum mobility - it is the most mobile AND most commonly dislocated joint in the body.
2. Glenohumeral Joint - Bony Architecture
- Type: Ball-and-socket, multiaxial synovial joint
- The humeral head is large and spherical; the glenoid fossa is small and shallow
- Glenoid covers only 25-30% of the humeral head surface area - this is why bony stability is inherently poor
- Humeral head inclination: 125 degrees (neck-shaft angle)
- Humeral retroversion: 25 degrees
- Glenoid retrotilt: slight - contributes to posterior stability
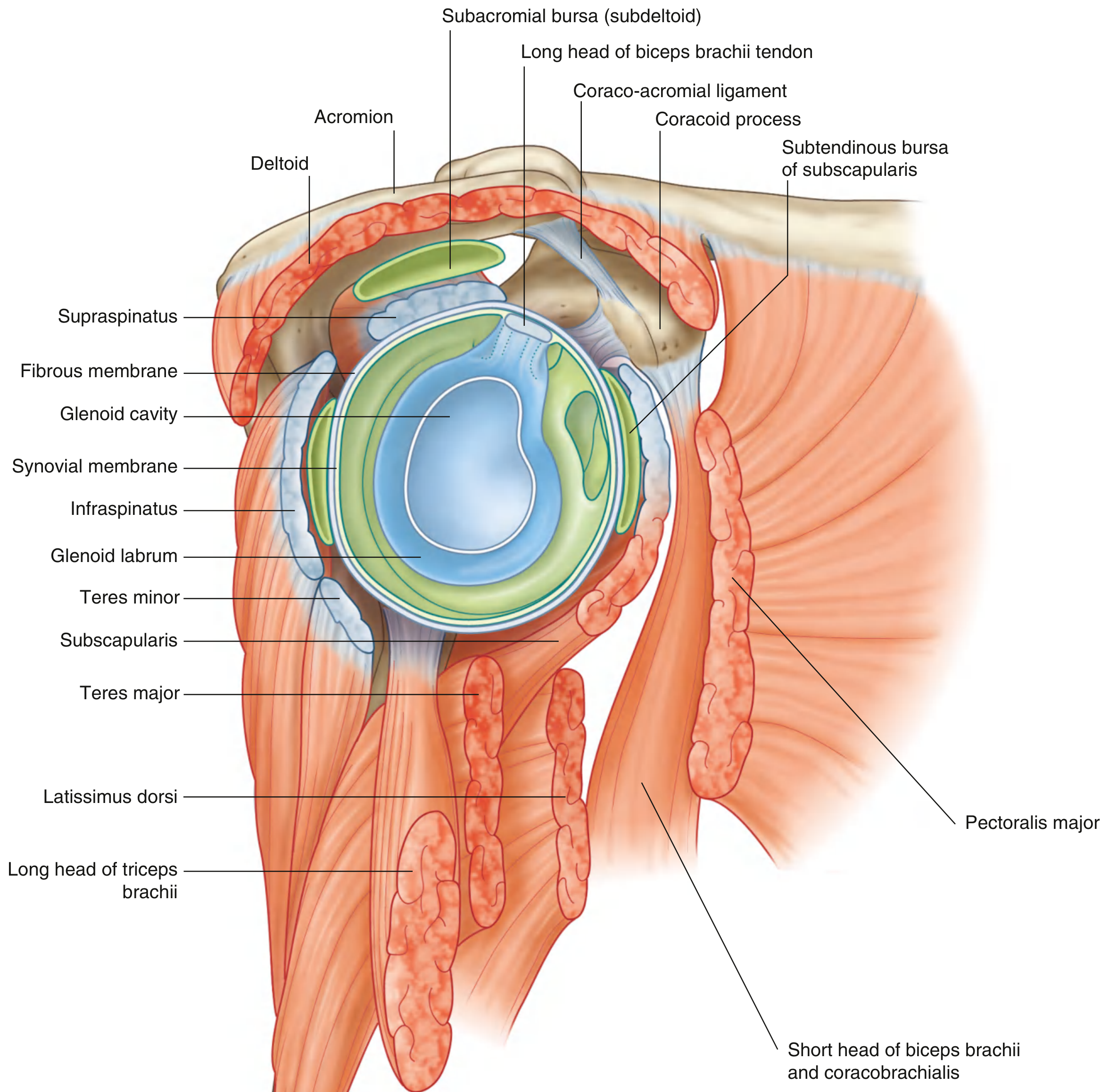
3. Glenoid Labrum
- Fibrocartilaginous rim attached around the glenoid margin
- Deepens the glenoid fossa and increases contact with the humeral head
- Works together with negative intraarticular pressure to provide a suction cup-like stability effect
- Superiorly continuous with the long head of biceps tendon (attaches to supraglenoid tubercle)
- Tears of the anteroinferior labrum = Bankart lesion (classic in anterior dislocation)
4. Joint Capsule
- Attaches to the glenoid margin (outside glenoid labrum) and to the anatomical neck of humerus
- Inferiorly loose and redundant - accommodates full abduction
- Medially, the capsule extends down the shaft - also allows abduction
- Becomes taut at extremes of motion; laxity in one region = tautness in the opposite region
5. Stabilizers - Static vs Dynamic (HIGH YIELD)
Static Stabilizers
| Stabilizer | Role |
|---|---|
| Bony anatomy (inclination, retroversion) | Passive congruence |
| Glenohumeral ligaments (GHL) | Primary ligamentous restraints |
| Glenoid labrum | Deepens socket |
| Negative intraarticular pressure | Prevents inferior subluxation |
| Joint capsule | Passive end-range restraint |
Dynamic Stabilizers
| Stabilizer | Role |
|---|---|
| Rotator cuff (SITS) | Most important dynamic stabilizer |
| Long head of biceps brachii | Restricts upward humeral head migration |
| Periscapular muscles | Optimize scapular position |
| Rotator interval structures | Fill the gap between supraspinatus & subscapularis |
6. Glenohumeral Ligaments (GHL) - HIGH YIELD
Three thickenings of the anterior capsule:
| Ligament | Origin | Insertion | Key Function |
|---|---|---|---|
| Superior GHL (SGHL) | Anterosuperior glenoid | Proximal lesser tuberosity | Limits inferior translation + external rotation in adduction |
| Middle GHL (MGHL) | Superomedial glenoid | Lesser tuberosity | Secondary stabilizer (anteroinferior) |
| Inferior GHL (IGHL) | Anteromedial glenoid | Distal lesser tuberosity + proximal shaft | Most important ligament - limits external rotation & anteroinferior instability in abduction |
IGHL exam fact: It is the primary restraint against anterior dislocation when the arm is in abduction + external rotation (the classic position of shoulder dislocation). It has 3 components to handle multi-directional loading.
Coracohumeral ligament: SGHL + coracohumeral together limit inferior translation and external rotation of the adducted arm.
7. Rotator Cuff - Force Couple Concept (VERY HIGH YIELD)
SITS muscles: Supraspinatus, Infraspinatus, Teres minor, Subscapularis
All originate from the scapula and insert into the greater (SST = Supra, Infra, Teres minor) and lesser (Subscapularis) tuberosities.
The Force Couple:
The deltoid pulls the humeral head superiorly (vertical vector). Alone, it would cause subacromial impingement.
The rotator cuff acts as humeral head depressors - they pull the head inferiorly and medially into the glenoid. Together with the deltoid, they convert this into a rotational (abduction) force.
Think of it as: Deltoid = engine, Rotator cuff = steering - they work together as "guy ropes" to keep the humeral head centered.
If rotator cuff is torn/weak:
- Humeral head migrates superiorly
- Subacromial impingement occurs
- Weakness in arm elevation
Muscle Actions Summary (Miller's Table):
| Movement | Primary Muscles |
|---|---|
| Abduction | Deltoid + Supraspinatus (cuff depresses head) |
| Adduction | Latissimus dorsi, pectoralis major, teres major |
| Forward flexion | Pectoralis major, anterior deltoid, biceps |
| Extension | Latissimus dorsi |
| Internal rotation | Subscapularis, teres major |
| External rotation | Infraspinatus, teres minor, posterior deltoid |
8. Scapulohumeral Rhythm (HIGH YIELD)
During full arm abduction to 180 degrees:
- Glenohumeral joint contributes: 120 degrees
- Scapulothoracic joint contributes: 60 degrees
- Ratio = 2:1 (GH : ST)
Memory trick: 2 parts GH, 1 part scapulothoracic = total 3 parts for every 3 degrees of abduction, 2 come from GH and 1 from scapulothoracic.
Important nuance: The 2:1 ratio is not constant throughout the range - it varies during the first 30 degrees. The early part of abduction involves more scapulothoracic (AC joint) motion.
Why it matters: Disturbance of the normal scapulohumeral rhythm causes secondary impingement.
9. Scapular Plane - Kinematics (EXAM FAVORITE)
- The scapula sits 30 degrees anterior to the coronal plane
- This plane is the preferred reference plane for ROM measurements
- Abduction in the scapular plane is called "scaption"
- Abduction requires external rotation of the humerus to prevent the greater tuberosity from impinging under the acromion
- With internal rotation contracture: abduction is limited to only 120 degrees
10. Zero Position / Resting Position
- Abduction of 165 degrees in the scapular plane
- In this position: minimal deforming forces on the shoulder
- Clinically important:
- Ideal position for reducing shoulder dislocations
- Ideal for applying traction to fractures
11. Subacromial Space and Impingement
The coraco-acromial arch = coracoid process + acromion + coraco-acromial ligament - forms a rigid roof over the rotator cuff.
Subacromial (subdeltoid) bursa lies between the rotator cuff and the acromion - it reduces friction during movement.
In subacromial impingement:
- Reactive inflammation of the subacromial bursa occurs
- Caused by: rotator cuff weakness (superior head migration), AC joint osteophytes, acromion morphology (Type III hooked acromion)
12. Supporting Joints - Quick Facts
Acromioclavicular Joint (ACJ)
- During abduction/elevation: clavicle rotates 30-40 degrees (mainly at sternoclavicular joint)
- Stabilized by conoid and trapezoid ligaments (coracoclavicular ligament) - maintain scapula-clavicle relationship
- Scapular rotation occurs through these ligaments
Sternoclavicular Joint (SCJ)
- Only bony link between upper limb and trunk
- Diarthrodial saddle joint with an intraarticular disk
- Movements: clavicular elevation/depression (frontal plane), protraction/retraction (transverse plane), rotation around long axis
- Strong posterior ligament = primary restraint for AP stability
- Costoclavicular ligament also stabilizes
- Posterior dislocation is dangerous - may impinge on great vessels at the root of the neck
Scapulothoracic Joint
- Not a true anatomical joint - physiological joint
- Scapula lies against posterolateral thoracic wall
- Provides origin for rotator cuff and most of deltoid
- Important for maintaining optimal rotator cuff muscle length-tension relationship
13. Shoulder Arthrodesis Position (Board Exam Fact)
If shoulder fusion (arthrodesis) is needed, the position is:
- 15-20 degrees abduction
- 20-25 degrees forward flexion
- 40-50 degrees internal rotation
- Excessive external rotation must be avoided
Quick Revision Box - Most Exam-Tested Facts
| Topic | Key Number/Fact |
|---|---|
| Scapulohumeral rhythm ratio | 2:1 (GH : scapulothoracic) |
| GH motion in abduction | 120 degrees |
| Scapulothoracic in abduction | 60 degrees |
| Most important ligament | IGHL (anteroinferior stability in abduction + ER) |
| Scapular plane | 30 degrees anterior to coronal |
| Humeral inclination | 125 degrees |
| Humeral retroversion | 25 degrees |
| Zero position | 165 degrees abduction in scapular plane |
| Most common dislocation direction | Anterior (arm in abduction + ER) |
| Most commonly dislocated joint in body | Glenohumeral |
| Bankart lesion | Anteroinferior labral tear (anterior dislocation) |
| Force couple concept | Rotator cuff depresses head + deltoid abducts = rotational force |
| SCJ - only bony link to trunk | Yes - fracture/dislocation can impinge great vessels |
This is a shared conversation. Sign in to Orris to start your own chat.