Explain 10 heart disease with ecg finding
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Here is a thorough guide to 10 heart diseases and their characteristic ECG findings, drawn from authoritative sources including Braunwald's Heart Disease, Goldman-Cecil Medicine, Rosen's Emergency Medicine, Fuster and Hurst's The Heart, and Harrison's Principles of Internal Medicine.
10 Heart Diseases and Their ECG Findings
1. ST-Elevation Myocardial Infarction (STEMI)
ECG Findings:
- Hyperacute T waves - tall, broad, peaked T waves (earliest change, minutes after onset)
- ST-segment elevation - >1 mm in 2 contiguous limb leads or >2 mm in 2 contiguous precordial leads
- Reciprocal ST depression - in leads "opposite" the infarct territory
- Pathological Q waves - develop within hours; width >40 ms, depth >25% of R wave (indicates transmural necrosis)
- T-wave inversion - follows ST normalization (reperfusion phase)
Localization:
| Territory | Leads with ST elevation | Culprit artery |
|---|---|---|
| Anterior | V1-V4 | LAD |
| Inferior | II, III, aVF | RCA (or LCx) |
| Lateral | I, aVL, V5-V6 | LCx |
| Posterior | Tall R + ST depression V1-V2 | RCA/LCx |
| Right ventricle | V4R elevation | RCA proximal |
Special patterns:
- Wellens syndrome - deep biphasic/inverted T waves in V2-V3 = critical LAD stenosis (preinfarction)
- De Winter sign - upsloping ST depression + peaked T in V1-V6 = LAD occlusion without classic elevation
- Sgarbossa criteria - used to diagnose AMI in the presence of LBBB
Rosen's Emergency Medicine, p. 993-1100; Harrison's 22E
2. Non-ST Elevation ACS (NSTEMI / Unstable Angina)
ECG Findings:
- Horizontal or downsloping ST depression - >0.5 mm, typically in multiple leads (indicates subendocardial ischemia)
- T-wave inversion - new symmetric T-wave inversion, especially >1 mm deep
- Transient ST changes - correlate with pain episodes
- ECG may be normal in up to 1-6% of confirmed NSTEMIs
Key distinction: No persistent ST elevation; no new Q waves typically form.
Harrison's 22E; Goldman-Cecil Medicine
3. Acute Pericarditis
ECG Findings (evolve in 4 classic stages):
| Stage | Timing | ECG Change |
|---|---|---|
| Stage 1 | Days 1-2 | Diffuse ST elevation (concave/saddle-shaped) in all leads except aVR and V1 + PR-segment depression |
| Stage 2 | Days 3-7 | ST and PR normalize (pseudo-normalization) |
| Stage 3 | Weeks 1-3 | Diffuse T-wave inversions |
| Stage 4 | Weeks-months | ECG returns to baseline |
Distinguishing from STEMI:
- ST elevation is diffuse (involves most leads, not territory-specific)
- ST morphology is concave upward ("saddle-shaped"), not convex
- PR depression is the hallmark finding
- No reciprocal changes (except in aVR and V1)
- No Q waves
Braunwald's Heart Disease; Goldman-Cecil Medicine, block 8; Fuster and Hurst's The Heart, block 16
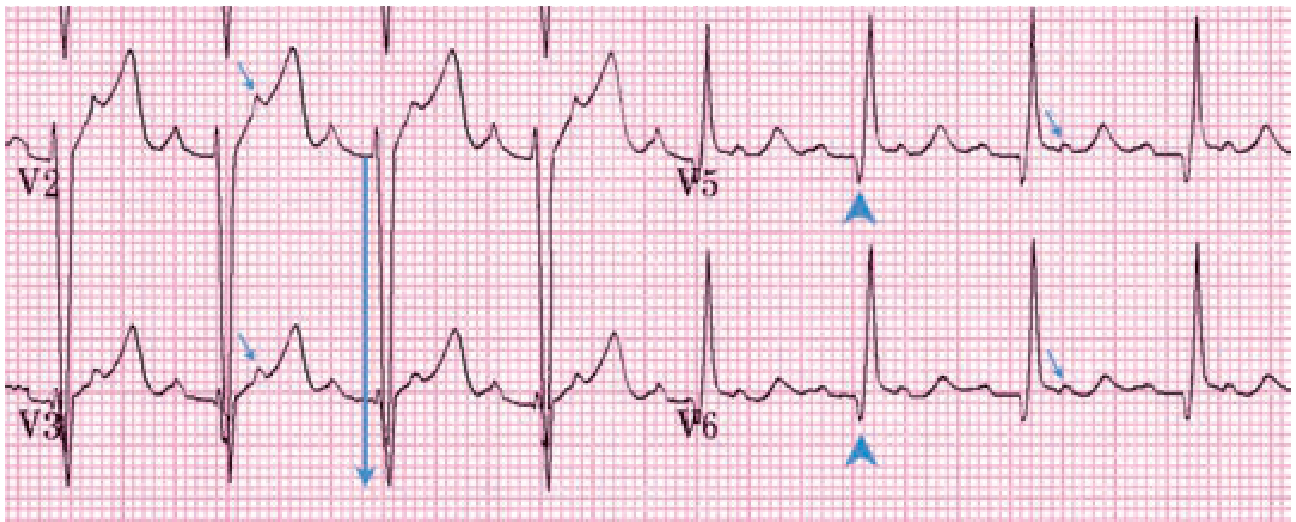
4. Hypertrophic Cardiomyopathy (HCM)
ECG Findings (abnormal in ~95% of cases):
- Left ventricular hypertrophy (LVH) - high-voltage QRS (Sokolow-Lyon: S in V1 + R in V5/V6 >35 mm)
- Deep, narrow Q waves in inferolateral leads (II, III, aVF, V4-V6) - called "septal Q waves," reflect hypertrophied septum
- Giant negative T waves in mid-precordial leads (V3-V5) - characteristic of apical HCM (Yamaguchi variant)
- ST-segment depression and T-wave inversions in lateral leads
- Left atrial enlargement - broad notched P wave (P mitrale)
- Atrial fibrillation - common in advanced disease
- LVH pattern + inferolateral Q waves in an athlete strongly favors HCM over athlete's heart
Tintinalli's Emergency Medicine, p. 1613; Goldman-Cecil Medicine
5. Pulmonary Embolism (PE)
ECG Findings:
- ECG is abnormal in ~70% of cases but non-specific - a normal ECG does not exclude PE
- Sinus tachycardia - most common finding
- S1Q3T3 pattern - deep S wave in lead I, Q wave in lead III, inverted T in lead III (present in only ~20%, but classic sign of acute right heart strain)
- New right bundle branch block (RBBB) - complete or incomplete - indicates right ventricular strain/overload
- T-wave inversions in V1-V4 (right precordial leads) - reflects RV strain
- Right axis deviation
- P pulmonale - tall peaked P waves in inferior leads (>2.5 mm) = right atrial overload
- Atrial fibrillation or flutter - occasional
- ST depression in inferior/lateral leads - from RV ischemia
Goldman-Cecil Medicine; Rosen's Emergency Medicine, block 3
6. Atrial Fibrillation (AF)
ECG Findings:
- Absent P waves - replaced by rapid irregular fibrillatory baseline ("f" waves at 350-600/min)
- Irregularly irregular RR intervals - the defining feature; no two RR intervals are alike
- QRS is typically narrow (unless aberrant conduction or bundle branch block is present)
- Ventricular rate is variable: typically 100-180/min if uncontrolled; <60/min if rate-controlled
Special situations:
- AF with WPW - can produce wide, irregular, very rapid QRS complexes (pre-excited AF) - life-threatening
- AF with LBBB - wide complex irregular rhythm mimicking VT
Rosen's Emergency Medicine, block 30; Braunwald's Heart Disease
7. Complete (Third-Degree) Heart Block
ECG Findings:
- P waves and QRS complexes are completely dissociated (independent rhythms)
- Atrial rate is regular and faster than ventricular rate (normal sinus rate ~60-100/min)
- Ventricular escape rhythm - QRS at 20-40/min (wide, bizarre if junctional escape is below His)
- If the escape pacemaker is junctional (above bifurcation): narrow QRS at 40-60/min
- If the escape pacemaker is ventricular: wide QRS at 20-40/min
- PP intervals are regular; RR intervals are regular - but they are independent of each other
Braunwald's Heart Disease, block 8; Goldman-Cecil Medicine
8. Wolff-Parkinson-White Syndrome (WPW)
ECG Findings:
- Short PR interval (<120 ms) - impulse bypasses the AV node via accessory pathway
- Delta wave - slurred upstroke at the beginning of the QRS (initial pre-excitation of ventricular myocardium)
- Widened QRS (>120 ms) - due to fusion of normal conduction + accessory pathway activation
- ST-T changes - secondary repolarization abnormalities opposite to the delta wave direction
- Pseudo-infarct patterns - negative delta waves in inferior or precordial leads can mimic Q waves of MI
Localization: Delta wave polarity and transition in precordial leads identifies the accessory pathway location (e.g., right anteroseptal: positive delta in inferior leads, transition V1-V2).
Braunwald's Heart Disease, block 7; Medical Physiology
9. Long QT Syndrome (LQTS)
ECG Findings:
- Prolonged QTc interval - corrected QT (Bazett formula: QT/√RR):
- Normal: <440 ms (men), <460 ms (women)
- Borderline: 440-470 ms
- Abnormal/diagnostic: >500 ms (high risk for Torsades)
- T-wave morphology varies by subtype:
- LQT1 - broad-based T wave (exercise-triggered arrhythmias)
- LQT2 - notched, bifid T wave (triggered by auditory stimuli/startle)
- LQT3 - late-onset, peaked T wave with long isoelectric ST segment (arrhythmias at rest/sleep)
- Torsades de Pointes (TdP) - polymorphic VT with QRS axis rotating around the baseline; may degenerate to VF
- Prominent U waves - occasionally seen (more typical of hypokalemia-induced QTc prolongation)
Fuster and Hurst's The Heart; Braunwald's Heart Disease
10. Left Ventricular Hypertrophy (LVH) / Hypertensive Heart Disease
ECG Findings:
- High-voltage QRS - the primary marker:
- Sokolow-Lyon criteria: S(V1) + R(V5 or V6) >35 mm
- Cornell criteria: R(aVL) + S(V3) >28 mm (men) or >20 mm (women)
- Left axis deviation - QRS axis between -30° and -90°
- "LV strain" pattern - asymmetric ST depression and T-wave inversion in lateral leads (I, aVL, V5-V6); reflects subendocardial ischemia from increased wall stress
- Left atrial enlargement (P mitrale) - broad, notched biphasic P wave in V1 (negative terminal component >1 mm deep and >40 ms wide)
- Prolonged QRS duration - near LBBB threshold in advanced disease
- Increased QRS duration + large voltages = increased LV mass confirmed on echo
Braunwald's Heart Disease; Goldman-Cecil Medicine
Quick Reference Summary
| Disease | Key ECG Finding |
|---|---|
| STEMI | ST elevation + Q waves (territory-specific) |
| NSTEMI/UA | ST depression + T-wave inversion |
| Acute Pericarditis | Diffuse saddle ST elevation + PR depression |
| HCM | LVH + deep septal Q waves + giant T inversions |
| Pulmonary Embolism | Sinus tach + S1Q3T3 + RBBB + right precordial T inversions |
| Atrial Fibrillation | No P waves + irregularly irregular RR intervals |
| Complete Heart Block | P-QRS dissociation + slow escape rhythm |
| WPW Syndrome | Short PR + delta wave + widened QRS |
| Long QT Syndrome | Prolonged QTc + T-wave morphology by subtype |
| LVH/Hypertensive Heart | High voltage + lateral strain pattern |
Sources: Rosen's Emergency Medicine; Braunwald's Heart Disease (2 Vol Set); Goldman-Cecil Medicine; Fuster and Hurst's The Heart 15E; Harrison's Principles of Internal Medicine 22E; Medical Physiology (Boron & Boulpaep); Tintinalli's Emergency Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.