Explain Hl and NHL
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content to write a detailed answer. Let me compose it.
Hodgkin Lymphoma (HL) and Non-Hodgkin Lymphoma (NHL)
Both HL and NHL are cancers of lymphoid tissue, but they differ fundamentally in their cell of origin, histology, clinical behavior, spread pattern, and prognosis.
HODGKIN LYMPHOMA (HL)
Definition
Hodgkin lymphoma is a B-cell lymphoma defined by the presence of Reed-Sternberg (RS) cells - large, distinctive neoplastic giant cells surrounded by a reactive (but ineffective) inflammatory infiltrate. Most patients (~90%) have classic Hodgkin lymphoma (cHL); the remaining ~10% have nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL), which has a distinct immunophenotype and natural history.
- Goldman-Cecil Medicine, Chapter 172
Epidemiology
- Incidence: ~2.7 per 100,000; ~30,000 new cases/year in North America and Europe
- Bimodal age distribution: early peak at 25-30 years, later peak at >50 years
- Slightly more common in males and in White populations
- In the Indian subcontinent, the age distribution shifts strongly into childhood
- Lifetime risk: approximately 1 in 250-300 in North America
Pathogenesis
Cell of origin: Elegant microdissection studies proved that every RS cell in a given case carries the same immunoglobulin gene rearrangements with somatic hypermutation - confirming origin from germinal center B cells.
EBV association: EBV is present in RS cells in up to 70% of mixed-cellularity subtype cases and a smaller fraction of other classic forms. The integration site is identical across all RS cells in a given case, indicating infection precedes clonal expansion.
Immune evasion: RS cells escape the host immune response by:
- Expressing PD-L1 and PD-L2 (checkpoint ligands that block T-cell activation)
- Losing β2-microglobulin function, preventing MHC class I expression
- Secreting immunosuppressive cytokines (IL-5, TGF-β, IL-13)
This makes HL one of the most responsive cancers to anti-PD-1 checkpoint inhibitors (nivolumab, pembrolizumab).
- Robbins & Kumar Basic Pathology
The Reed-Sternberg Cell
The RS cell is the sine qua non of HL:
- Very large (15-45 µm)
- Multilobate nucleus with enormous, prominent nucleoli
- Classic "owl-eye" appearance: two mirror-image nuclei, each with a large acidophilic nucleolus surrounded by a clear halo
- Immunophenotype (classic): CD15+, CD30+, CD45-, B-cell markers negative, T-cell markers negative
Here is the histology showing classic RS cells among reactive lymphocytes (mixed-cellularity type):
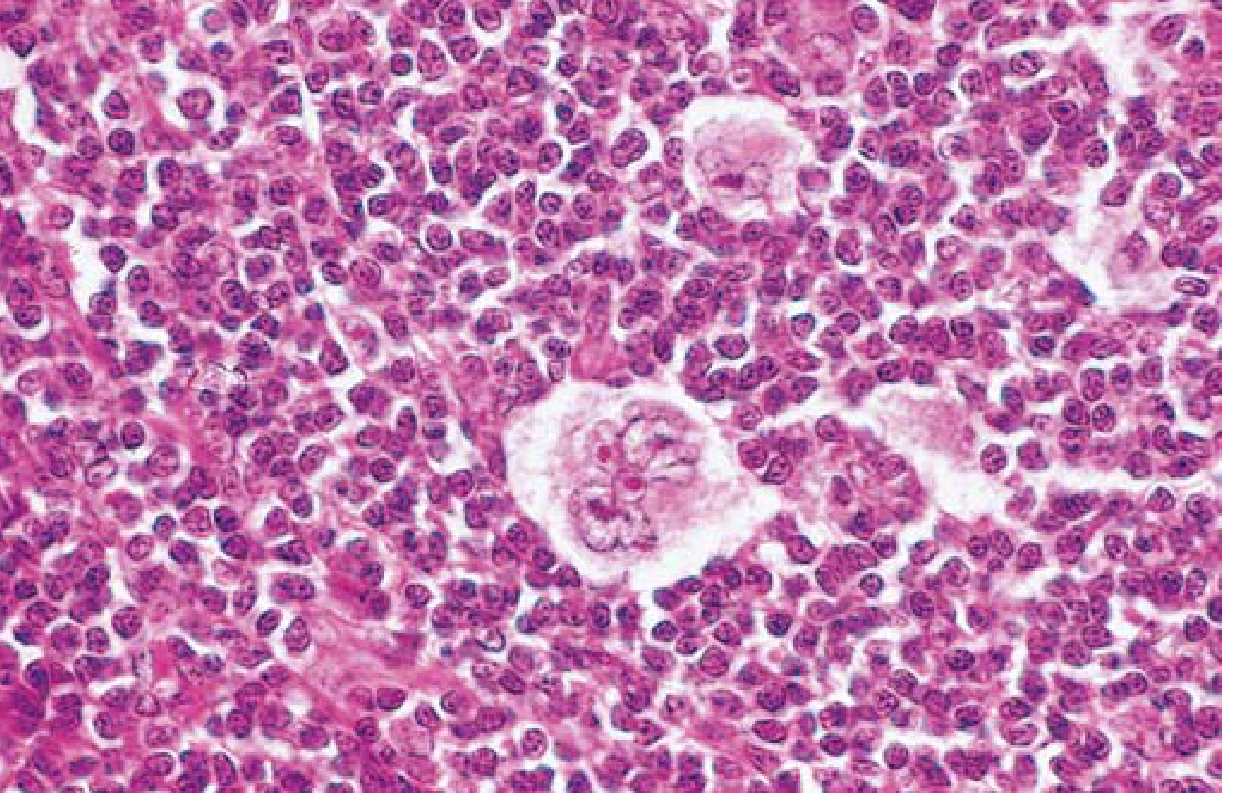
Classic Reed-Sternberg cell with owl-eye nucleoli, surrounded by lymphocytes - Robbins Pathology
Subtypes of HL
| Subtype | Frequency | Key Features |
|---|---|---|
| Nodular sclerosis | Most common | Adolescents/young adults; mediastinal involvement; lacunar cells; collagen bands dividing tumor into nodules |
| Mixed cellularity | 2nd most common | Strong EBV association (up to 70%); classic RS cells; eosinophils, plasma cells |
| Lymphocyte rich | Rare | Few RS cells; best prognosis among classic subtypes |
| Lymphocyte depleted | Rare | Many RS cells, few lymphocytes; older patients, advanced disease; worst prognosis |
| NLPHL | ~10% | "Popcorn" (lymphocytic/histiocytic) cells; CD20+, CD15-, CD30-; indolent, excellent prognosis |
Clinical Features
- Painless lymphadenopathy (most common presentation), usually cervical/supraclavicular/mediastinal
- B symptoms: fever, drenching night sweats, >10% weight loss
- Alcohol-induced lymph node pain (classic but rare)
- Mediastinal widening on chest X-ray (especially nodular sclerosis)
- Pruritus and anemia in advanced disease
- Spreads in a stepwise, contiguous fashion through anatomically adjacent nodes
Staging (Ann Arbor / Lugano)
| Stage | Description |
|---|---|
| I | Single lymph node region or single extranodal site (IE) |
| II | Two or more regions on the same side of the diaphragm |
| III | Regions on both sides of the diaphragm |
| IV | Diffuse/disseminated extranodal involvement (liver, bone marrow, lung) |
Suffix A = no B symptoms; B = fever, night sweats, weight loss. Staging workup includes CT neck/thorax/abdomen/pelvis + FDG-PET/CT (more sensitive and specific than CT alone; bone marrow biopsy no longer needed when PET is used).
Treatment
| Group | Stage | Treatment |
|---|---|---|
| Limited | IA or IIA, no bulky disease | ABVD × 2 cycles + involved-region radiotherapy (IRRT); OR ABVD × 3 if PET-negative |
| Advanced | IB, IIB, III, IV, or bulky disease | ABVD × 6; or A+AVD (brentuximab vedotin + AVD) × 6; or escalated BEACOPP × 4-6 |
| Relapsed/Refractory | Any stage | Second-line chemotherapy → high-dose chemoradiation → autologous HCT |
- ABVD = Adriamycin (doxorubicin), bleomycin, vinblastine, dacarbazine
- BEACOPP = bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, prednisone
- Checkpoint inhibitors (nivolumab, pembrolizumab) are highly active in relapsed/refractory HL (PD-L1 amplification makes cHL exquisitely sensitive)
Prognosis: 5-year survival >90% for stage I-IIA; ~50% disease-free survival even at stage IV. Long-term survivors treated with radiotherapy have increased risk of lung cancer, breast cancer, and cardiovascular disease.
NON-HODGKIN LYMPHOMA (NHL)
Definition
NHL is a heterogeneous group of lymphoid malignancies that do not fulfill the criteria for Hodgkin lymphoma. They arise from B cells, T cells, or (rarely) NK cells at various stages of differentiation. Unlike HL, they lack Reed-Sternberg cells and do not follow predictable contiguous spread.
Epidemiology
- Far more common than HL: NHL represents ~85-90% of all lymphomas
- Incidence increases with age
- Risk factors: immunodeficiency (HIV, post-transplant), autoimmune disease, prior chemotherapy/radiation, infectious agents (EBV, HTLV-1, H. pylori, HCV, HHV-8)
WHO Classification (Selected Key Types)
B-cell lymphomas (most common, ~85%):
| Type | Behavior | Key Features |
|---|---|---|
| Diffuse Large B-Cell Lymphoma (DLBCL) | Aggressive | Most common NHL in adults; rapidly enlarging nodes |
| Follicular Lymphoma | Indolent | Nodular growth pattern; t(14;18), BCL2 overexpression; frequent relapse |
| Burkitt Lymphoma | Very aggressive | "Starry sky" pattern; EBV-associated; t(8;14) MYC translocation; highly curable |
| Mantle Cell Lymphoma | Aggressive/indolent | t(11;14), cyclin D1 overexpression; poor prognosis |
| Marginal Zone Lymphoma (MALT) | Indolent | Associated with H. pylori (gastric), HCV, Sjogren's |
| CLL/SLL | Indolent | Same disease: CLL = blood/marrow; SLL = nodal |
| Primary CNS Lymphoma | Aggressive | DLBCL variant; EBV-associated in immunocompromised |
| Primary Effusion Lymphoma | Aggressive | HHV-8 + EBV; presents as malignant effusion (no mass); rare, HIV-associated |
| Plasmablastic Lymphoma | Aggressive | EBV+, CD20-negative; oropharynx; HIV-associated |
T-cell and NK-cell lymphomas (~15%):
| Type | Key Features |
|---|---|
| Peripheral T-cell lymphoma (PTCL) | Heterogeneous, generally aggressive |
| Anaplastic Large Cell Lymphoma (ALCL) | ALK+ (better prognosis) or ALK- |
| T-cell lymphoblastic lymphoma | Often mediastinal mass; SVC/airway obstruction risk |
| Adult T-cell leukemia/lymphoma (ATLL) | HTLV-1 associated; hypercalcemia, lytic bone lesions |
| NK/T-cell lymphoma, nasal type | EBV-associated; destructive midline facial lesion |
Clinical Features
- Painless lymphadenopathy (most common)
- B symptoms (fever, night sweats, weight loss)
- Unlike HL, NHL spreads non-contiguously and often presents at advanced stage
- Extranodal involvement is common (GI tract, skin, CNS, bone marrow)
- Aggressive NHL (e.g., DLBCL, Burkitt): rapidly enlarging nodes, elevated LDH, risk of tumor lysis syndrome
- Indolent NHL (e.g., follicular): slow-growing, waxing and waning, often incurable but long survival
Diagnosis
- Excisional lymph node biopsy (preferred; core biopsy acceptable in some cases)
- Immunohistochemistry and flow cytometry for cell markers (CD19, CD20, CD3, CD5, CD10, CD23, BCL2, MYC, cyclin D1, etc.)
- Cytogenetics/FISH for characteristic translocations (t(14;18) follicular, t(8;14) Burkitt, t(11;14) mantle cell)
- Staging: CT + PET; bone marrow biopsy when indicated
- LDH, β2-microglobulin (prognostic markers)
Treatment
Highly subtype-dependent:
- DLBCL (aggressive): R-CHOP (rituximab + cyclophosphamide, doxorubicin, vincristine, prednisone) x 6 cycles; autologous HCT for relapsed chemosensitive disease; CAR-T cell therapy (axicabtagene, tisagenlecleucel) for refractory disease
- Follicular (indolent): Watch-and-wait for asymptomatic low-burden disease; rituximab ± chemotherapy; obinutuzumab; autologous HCT in younger patients with multiple relapses
- Burkitt: Intensive multi-agent chemotherapy (e.g., CODOX-M/IVAC); highly curable (~80-90%)
- T-cell lymphoblastic: ALL-type induction chemotherapy; CNS prophylaxis; HCT in high-risk
- Mantle cell: R-CHOP or R-HyperCVAD; autologous HCT as frontline consolidation; BTK inhibitors (ibrutinib) for relapsed disease
- Primary CNS lymphoma: High-dose methotrexate-based regimens; radiation is palliative
- In HIV-associated NHL: antiretroviral therapy is the cornerstone; chemotherapy added for systemic disease
KEY DIFFERENCES AT A GLANCE
| Feature | Hodgkin Lymphoma | Non-Hodgkin Lymphoma |
|---|---|---|
| Hallmark cell | Reed-Sternberg cell (CD15+, CD30+) | No RS cell; neoplastic lymphocytes |
| Cell of origin | Germinal center B cell | B cell (85%), T/NK cell (15%) |
| Spread | Contiguous, stepwise | Non-contiguous, unpredictable |
| Age | Bimodal (young adults + elderly) | Predominantly elderly (most subtypes) |
| EBV association | Frequent (esp. mixed cellularity) | Burkitt, DLBCL in HIV, PEL, PTCL |
| Extranodal disease | Rare at presentation | Common |
| Mediastinal involvement | Common (nodular sclerosis) | Less common (except T-LBL) |
| B symptoms | Common | Variable |
| Prognosis | Generally excellent; most cured | Highly variable by subtype |
| Key treatment | ABVD; checkpoint inhibitors | R-CHOP (B-cell); CAR-T for refractory |
Sources:
- Robbins & Kumar Basic Pathology (HL pathogenesis, RS cell morphology, subtypes)
- Goldman-Cecil Medicine, Chapters 172 (HL) and 171 (NHL)
- Swanson's Family Medicine Review (pediatric NHL subtypes)
This is a shared conversation. Sign in to Orris to start your own chat.