Incarnated hernia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"incarcerated hernia" management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Obstructed hernia vs incarcerated hernia
Finding Sources
Finding Sources
Reading File
Reading File
Here is a detailed comparison, synthesized from multiple surgical textbooks:
Obstructed Hernia vs Incarcerated Hernia
Definitions
| Feature | Incarcerated Hernia | Obstructed Hernia |
|---|---|---|
| Core meaning | Contents are trapped/irreducible - cannot be returned to abdominal cavity | Irreducible hernia + bowel lumen blocked causing intestinal obstruction |
| Blood supply | Intact (no vascular compromise) | Intact (no vascular compromise) |
| Reducibility | Irreducible | Irreducible (always) |
| Bowel obstruction | May or may not be present | Always present |
| Urgency | Urgent (6-12 hrs) | Urgent surgical emergency |
The Spectrum of Hernia Complications
From S Das Manual of Clinical Surgery (a widely used framework), hernias are classified as:
- Reducible - contents freely return to abdomen
- Irreducible - contents trapped, no other complication (due to adhesions, large scrotal hernia, sliding hernia)
- Obstructed / Incarcerated = Irreducible + intestinal obstruction, no vascular compromise
- Strangulated = Irreducible + obstruction + arrested blood supply (surgical emergency)
- Inflamed - rare; from inflamed contents (appendix, Meckel's diverticulum)
Key point from S Das: "An obstructed hernia means the hernia is associated with intestinal obstruction due to occlusion of the lumen of the bowel. There is NO interference with blood supply to the intestine."
Important Nuance: How Different Texts Use "Incarcerated"
There is genuine terminological variation across textbooks:
S Das (Indian surgery tradition) uses "obstructed or incarcerated" together - treating them as essentially synonymous (irreducible + intestinal obstruction, no vascular compromise).
Bailey & Love distinguishes more subtly: "Incarcerated" literally means "imprisoned" - it means a hernia that is not only irreducible but also potentially developing toward strangulation. It may or may not yet have bowel obstruction.
Mulholland & Greenfield (US tradition): "Incarcerated = irreducible." It is not in itself a surgical emergency - many hernias are chronically incarcerated due to adhesions of omentum without any obstruction or strangulation.
Roberts & Hedges (Emergency Medicine): "An incarcerated hernia is one whose contents are not reducible without surgical intervention." A strangulated hernia is an incarcerated hernia with compromised blood supply.
Practical Clinical Distinctions
| Incarcerated (uncomplicated) | Obstructed | |
|---|---|---|
| Symptoms | Tender, tense, non-reducible mass; may be mild/chronic | Colicky abdominal pain, vomiting, distension, absolute constipation |
| Bowel sounds | May be normal within hernia | High-pitched, tinkling; absent later |
| Systemic signs | Usually minimal | Dehydration, electrolyte imbalance |
| Skin over hernia | Normal | Normal (erythema = strangulation) |
| Temperature | Afebrile | Afebrile (fever = strangulation) |
| Imaging | Dilated bowel proximal to hernia on CT/US | Same; may see transition point at hernia neck |
From Maingot's Abdominal Operations: "The incarcerated hernia may be mildly tender due to venous congestion from the tight defect. The strangulated hernia will be tender and warm and may have surrounding skin erythema... The incarcerated hernia requires operation on an urgent basis within 6-12 hours."
Why This Distinction Matters Clinically
- Both obstructed and incarcerated hernias require urgent surgery, but neither is as immediately life-threatening as strangulation
- The danger is that obstructed hernia can rapidly progress to strangulation - strangulation may occur within just 2 hours of incarceration (Yamada's Gastroenterology)
- Diagnosing "obstructed hernia" when strangulation is actually present wastes critical time - Das warns this is a "dangerous venture"
- Reduction attempts are reasonable for incarcerated hernias without obstruction signs, but must not be attempted if strangulation is suspected - reinserting ischemic/gangrenous bowel causes peritonitis and sepsis
Richter's Hernia - Special Case
In Richter's hernia, only part of the bowel wall herniates (not the full lumen). The bowel lumen remains patent, so there is no intestinal obstruction - yet strangulation of the knuckle can still occur. This is why strangulation does not always accompany obstruction.
Summary
- Incarcerated = irreducible (the umbrella term in most Western textbooks)
- Obstructed = irreducible + bowel lumen occluded + blood supply intact
- All obstructed hernias are incarcerated; not all incarcerated hernias are obstructed
- Neither has vascular compromise - that defines strangulation, which is the true emergency
Sources: S Das Manual of Clinical Surgery (13th ed.); Bailey & Love's Short Practice of Surgery (28th ed.), p. 1345; Maingot's Abdominal Operations; Mulholland & Greenfield's Surgery (7th ed.); Yamada's Textbook of Gastroenterology (7th ed.); Roberts & Hedges' Clinical Procedures in Emergency Medicine
Extract all questions from surgery pearls edition 1
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I've browsed the complete library catalog (130+ books). "Surgery Pearls Edition 1" is not available in the medical textbook library.
Here is the full list of surgery-related books that are available:
| Title | Speciality |
|---|---|
| Bailey and Love's Short Practice of Surgery (28th ed.) | General Surgery |
| Current Surgical Therapy (14th ed.) | General Surgery |
| Fischer's Mastery of Surgery (8th ed.) | General Surgery |
| Maingot's Abdominal Operations | Gastro Surgery |
| Mulholland and Greenfield's Surgery (7th ed.) | General Surgery |
| S Das A Manual on Clinical Surgery (13th ed.) | General Surgery |
| Sabiston Textbook of Surgery (Biological Basis of Modern Surgical Practice) | General Surgery |
| Schwartz's Principles of Surgery (11th ed.) | General Surgery |
| 22nd Edition Pye's Surgical Handicraft | General Surgery |
| Campbell's Operative Orthopaedics (15th ed., 2026) | Orthopedics |
| Rockwood and Green's Fractures in Adults (10th ed., 2025) | Orthopedics |
"Surgery Pearls Edition 1" - whether you mean Surgery: Pearls and Pitfalls or another title with "Pearls" in the name - is not in the library database. It cannot be searched or extracted.
If you have the book as a PDF or other file, you can upload it and I can extract questions from it. Alternatively, if you were thinking of one of the surgery books listed above, let me know and I can extract question-style content (review questions, clinical scenarios, self-assessment items) from that book instead.
Author dayanand babu
Finding Sources
Searching the Web
Surgery Pearls Edition 1 Dayanand Babu book
The book is identified. The full title is "Clinical Surgery Pearls" by R. Dayananda Babu, MS, MNAMS - Professor and Head, Department of Surgery, Sree Gokulam Medical College and Research Foundation, Thiruvananthapuram, Kerala, India. Published by Jaypee Brothers Medical Publishers, ISBN: 978-93-5090-395-4 (1st edition, 2013), 509 pages.
Unfortunately, this book is NOT in the medical textbook library database. I have checked all 130+ books in the library and it is not there, regardless of the author name.
What I can tell you about this book:
- It is a popular clinical surgery exam preparation book, widely used by MBBS students and surgical postgraduate aspirants in India
- The 1st edition was published in 2013; a 2nd edition also exists (2018, co-authored with S. Vittal)
- The book follows a question-answer / pearls format - covering clinical scenarios, viva voce questions, and key surgical facts
- It covers topics like hernias, thyroid, breast, GI surgery, trauma, and more in a concise Q&A style
Options to get the questions:
- Upload the PDF - If you have a PDF copy of the book, attach it here and I can extract all questions from it
- Use available surgery books - I can extract Q&A / clinical pearls style content from books that are in the library, such as:
- S Das Manual on Clinical Surgery (13th ed.) - similar Indian surgery exam-oriented style
- Bailey & Love's Short Practice of Surgery (28th ed.)
- Schwartz's Principles of Surgery (11th ed.)
Would you like to upload the PDF, or shall I work with one of the available books?
Teach me laparoscopic appendicectomy
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Here is a complete, step-by-step surgical teaching on laparoscopic appendicectomy, drawn from Fischer's Mastery of Surgery (8th ed.), Bailey & Love (28th ed.), and Maingot's Abdominal Operations.
Laparoscopic Appendicectomy - Complete Surgical Guide
Why Laparoscopic?
Laparoscopic appendicectomy (LA) has become the standard approach in most centers. Advantages over open:
| Laparoscopic | Open |
|---|---|
| Shorter hospital stay | Shorter OR time |
| Better pain control | Lower OR cost |
| Fewer wound infections | Fewer intra-abdominal abscesses |
| Better cosmesis | Lower hospital cost |
| Diagnostic advantage - can visualize entire abdomen | |
| Particularly valuable in women of childbearing age (normal appendix in >40%; gynecologic pathology found in 73% laparoscopically vs. 17% open) |
Preoperative Preparation
- NPO - confirm fasting status; consider nasogastric decompression if not prolonged NPO
- IV antibiotics - single preoperative dose of a second-generation cephalosporin (e.g., cefoxitin); continue only if scheduled antibiotics already running
- Foley catheter - mandatory to decompress bladder and avoid port-site bladder injury; can be omitted if patient voids just before OR
- Nasogastric tube - to decompress stomach, especially in non-fasted patients
- Consent - include possibility of conversion to open
Patient Positioning & Room Setup
- Patient positioned supine, left arm tucked and padded
- Monitor placed on patient's right side at level of anterior superior iliac spine
- Surgeon and assistant both stand on the patient's left side
- After ports are placed: reverse Trendelenburg with left side tilted down - this improves visualization of the appendix and right lower quadrant by allowing bowel to fall away
Port Placement (3-Port Technique)
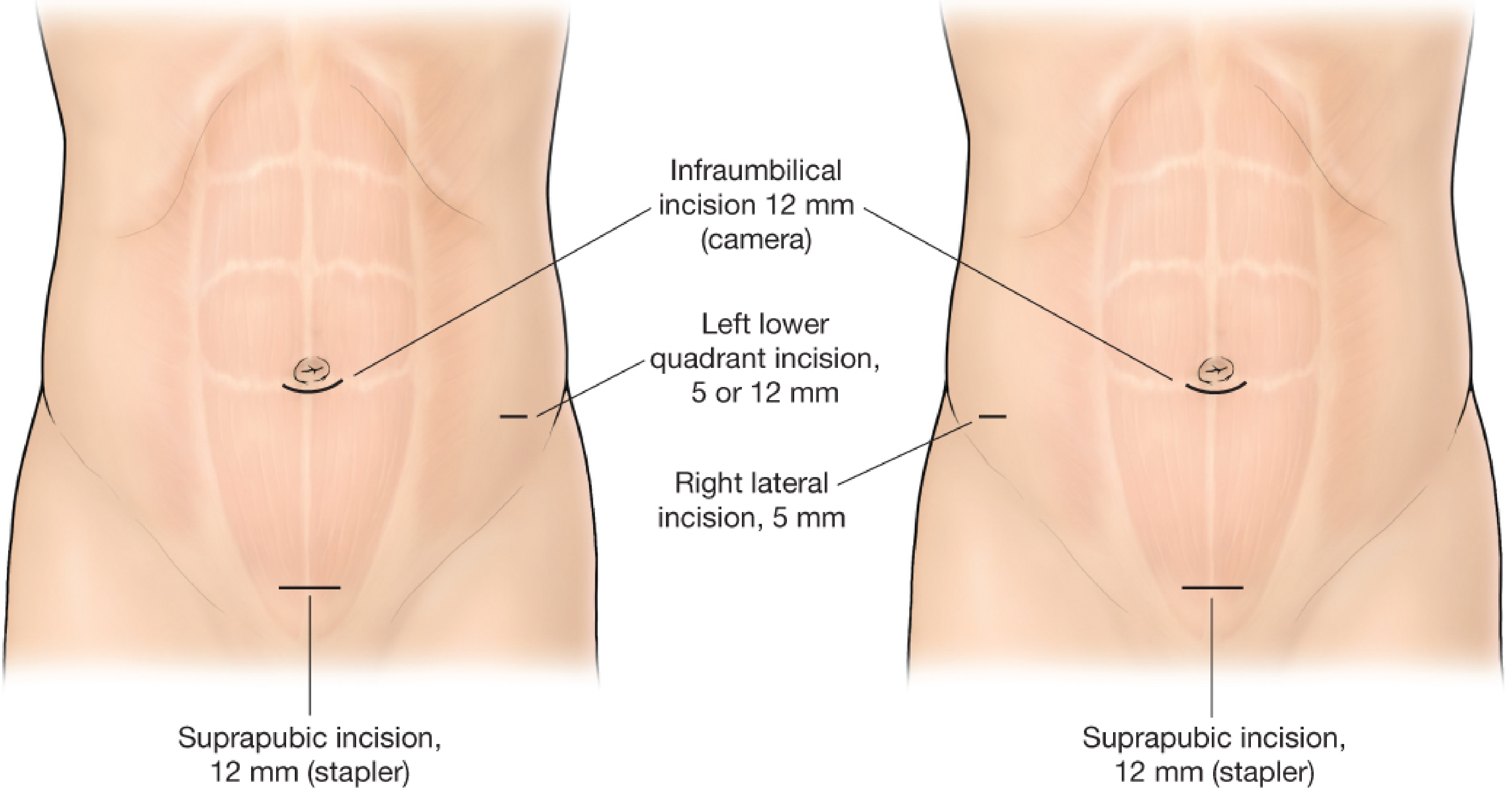
Standard three-port configuration: infraumbilical 12mm (camera), suprapubic 12mm (stapler), left lower quadrant 5mm or 12mm (working port)
The principle is triangulation - port positions direct the camera and instruments toward the RLQ for optimal appendix visualization.
| Port | Size | Purpose |
|---|---|---|
| Infraumbilical | 12 mm | Camera port (30° scope) |
| Suprapubic | 12 mm | Stapler/working port |
| Left lower quadrant | 5 or 12 mm | Working/retraction port |
Alternative: some surgeons use a right lateral 5mm port instead of LLQ port. Port configuration may be modified based on prior scars.
Abdominal Entry & Pneumoperitoneum
Three accepted techniques - use whichever you are most comfortable with; have a backup method ready:
1. Open (Hassan) technique (described):
- Vertical skin incision just above the umbilicus
- Carry down to fascia
- Grasp fascia with Kocher clamps and elevate
- Incise fascia with scalpel
- Insert blunt 12 mm trocar directly into peritoneal cavity
- Establish CO₂ pneumoperitoneum
- Insert 30° 5-mm camera
2. Veress needle technique - blind needle insertion then trocar
3. Optiview technique - visual entry trocar under direct vision
Remaining two 5mm ports placed under direct visualization - take great care to avoid bladder and hollow viscus injury.
Intraoperative Steps
Step 1 - Initial Survey
Before focusing on the appendix, inspect the entire abdominal cavity systematically. If the appendix is normal, you must identify the real pathology:
- Tubo-ovarian abscess
- Ovarian cyst/torsion
- Endometriosis / PID
- Meckel's diverticulitis
- Terminal ileitis
- Cholecystitis
Step 2 - Locating the Appendix
Sweep small bowel out of the RLQ. Use these anatomical landmarks:
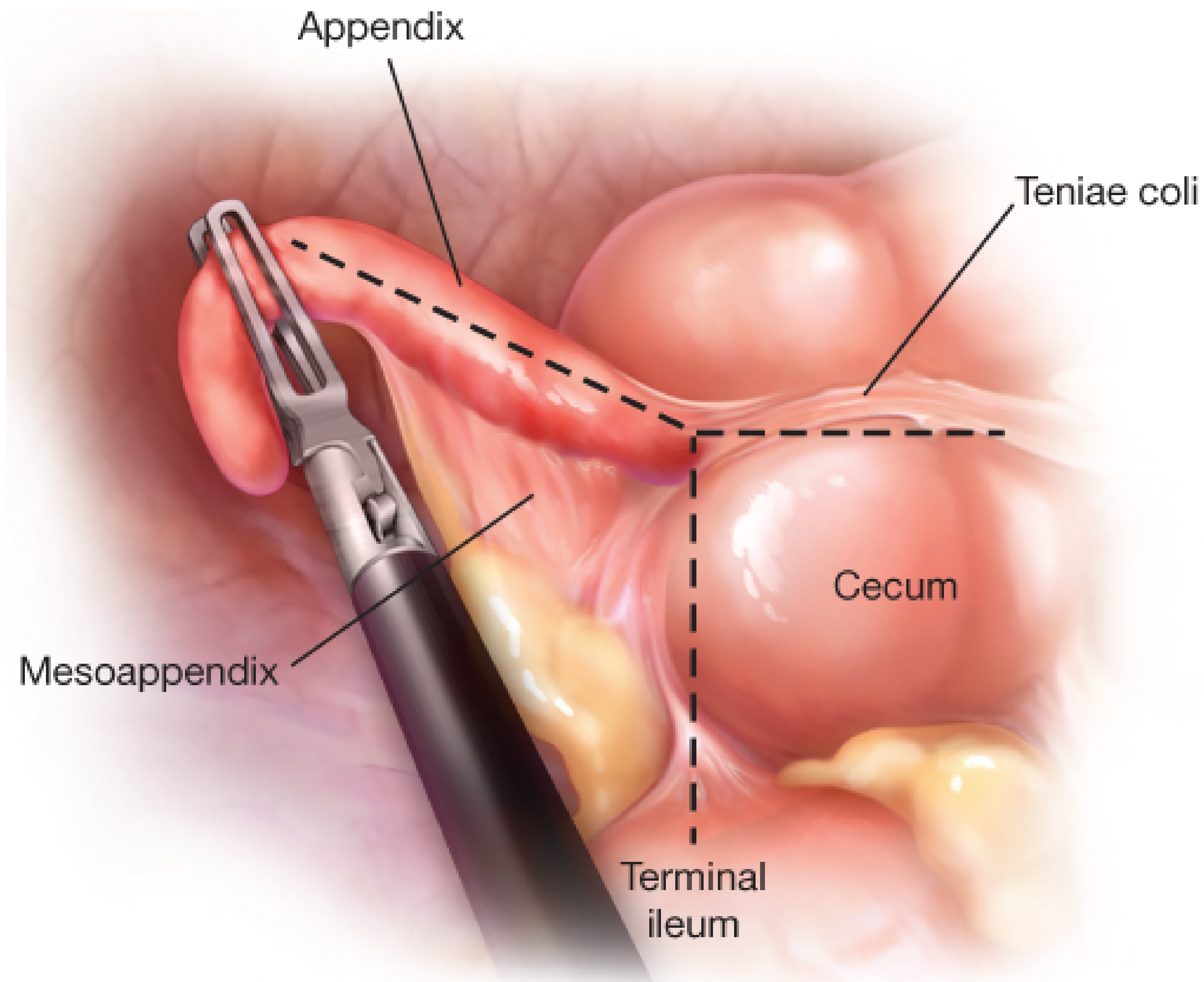
The teniae coli all converge on the cecum, directly leading to the appendix base
- Teniae coli of right colon all coalesce at the cecum - trace them to find the appendix base
- Ileal sail - antimesenteric fat pad on terminal ileum
- Ligament of Treves - from terminal ileum to appendix base
If the appendix is retrocecal (most common variant), you will need to mobilize the cecum and ascending colon by dividing peritoneal attachments laterally.
Step 3 - Mobilization & Retraction
- Grasp appendix with laparoscopic tissue-holding forceps (left hand)
- Retract appendix toward anterior abdominal wall
- Elevate the appendix to display the mesoappendix
- Use a Maryland dissector (right hand) to create a window between the appendix base and mesoappendix - do this carefully under direct vision to avoid cecal injury
- The camera can be moved to the LLQ port for better triangulation and stapling angle
Step 4 - Dividing the Mesoappendix
Once the window at the base is established:
Option A - Linear cutting stapler:
- Use endo-GIA with vascular load (2.5 mm staple height)
- May need multiple firings depending on mesentery length
Option B - Energy device:
- LigaSure or harmonic scalpel along the length of mesoappendix
Option C - Clips:
- Isolate appendicular artery, apply laparoscopic clips, then divide
Step 5 - Dividing the Appendix at the Base
Option A - Linear stapler (preferred for inflamed/thick appendix):
- Endo-GIA with 3.5 mm staple height
- Introduced through the 12 mm suprapubic port
- Smaller jaw inserted through the window created between appendix and mesoappendix
- Must visualize both distal ends of the jaws to confirm no other viscera are included
- Fire at the appendix-cecum junction
Option B - Endoloop (for less inflamed cases):
- Divide mesoappendix first
- Apply absorbable loop ligature (endoloop) at the base
- Divide with laparoscopic scissors
- Two loops proximally, one distally is the standard practice
If the cecum base is inflamed or gangrenous, staple above the area of involvement - include a rim of healthy cecum on the proximal stapled end. If inflammation reaches the ileocecal valve, ileocecectomy with anastomosis may be necessary.
Step 6 - Specimen Extraction
- Place the divided appendix into a laparoscopic specimen bag
- Remove the bag through the 12 mm umbilical port site
- Avoids contamination of port site and wound infection
Step 7 - Washout & Inspection
- Inspect the appendiceal stump for adequate closure - no leaks, good staple line
- Check hemostasis in the mesoappendix
- Irrigate RLQ and pelvis with warm saline to evacuate any purulent fluid
- The benefit of irrigation is still debated in the literature - do not over-irrigate as this may spread contamination
Closure
- Remove all ports under direct visualization
- Close fascia at the 12 mm port sites with absorbable suture (interrupted or figure-of-eight) - prevents port-site hernia
- Fascia at 5 mm sites generally does not need closure
- Skin closed subcuticularly with absorbable suture at all port sites
Postoperative Care
Simple (uncomplicated) appendicitis:
- Remove NGT and Foley before patient wakes
- No postoperative antibiotics needed
- Diet as tolerated once awake
- Oral analgesia
- Many patients discharged same day from PACU
Complicated appendicitis (perforated/gangrenous):
- In-hospital observation required
- Continue IV antibiotics
- Monitor for intra-abdominal abscess (most common complication of LA vs. wound infection in open)
Intraoperative Problems & Solutions
| Problem | Management |
|---|---|
| Normal appendix found | Remove it anyway (avoid future diagnostic confusion); carefully exclude Meckel's, terminal ileitis, tubo-ovarian pathology |
| Cannot find the appendix | Mobilize cecum; trace teniae coli to their confluence before diagnosing "absent appendix" |
| Appendix mass / abscess | Safer to abandon appendicectomy; drain abscess, give IV antibiotics, monitor; interval appendicectomy later |
| Retrocecal appendix | Divide lateral peritoneal attachments; mobilize cecum/ascending colon; protect right ureter |
| Inflamed base / cecal involvement | Staple with rim of healthy cecum; if ileocecal junction involved - consider ileocecectomy |
| Reduction en masse concern (post-reduction) | If mesoappendix divided before appendix - still valid; confirm stump is fully closed |
Laparoscopic vs. Open: Bottom Line
From Maingot's: "One cannot convincingly recommend either open or laparoscopic over the other. Each has advantages that should be considered."
The main scenarios where LA is clearly preferred:
- Diagnostic uncertainty (especially women of childbearing age)
- Obese patients (wound complications higher with open)
- When early return to activity is important
The main scenario where open may be preferred:
- Limited laparoscopic resources or expertise
- Dense adhesions from prior surgery
Robotic-Assisted Appendicectomy (Emerging)
- 3D 4K visualization superior to standard laparoscope
- Articulated instruments improve ergonomics
- May be useful in complex cases requiring difficult dissection
- May reduce conversion-to-open rates
- Data on outcomes versus standard laparoscopy still limited
Sources: Fischer's Mastery of Surgery (8th ed.); Bailey & Love's Short Practice of Surgery (28th ed.); Maingot's Abdominal Operations
This is a shared conversation. Sign in to Orris to start your own chat.