

Screenshot_20260623-143315_Adobe Acrobat.png
Screenshot_20260623-143306_Adobe Acrobat.png
Analyse above report
Reading File
analyse_media
analyse_media
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the data needed for a complete, structured analysis. Here is the full report breakdown:
MRI Fistulogram Report - Analysis
Patient: Mr. Chitransh Kumar | 22-year-old Male
Facility: Best Diagnostics, New Delhi (NABH Accredited) | Report date: 22 Jun 2026
Referred by: Dr. Anil Agarwal (Urologist)
Clinical background: Prior fistula surgery; presents with perianal pain and pus discharge for 1 month
Study Protocol
High-resolution T1- and T2-weighted MRI of the pelvis in sagittal and axial planes, with fat-suppressed T2W axial, sagittal, and coronal images using a phased-array surface coil. This is the standard protocol for an MRI fistulogram, which is the imaging gold standard for complex or recurrent anal fistulae.
Key MRI Findings - Tract-by-Tract
1. Internal Opening
- Located at 6 o'clock position, approximately 2.5 cm proximal to the anal verge - this corresponds to the dentate line level, which is the classic cryptoglandular origin.
2. Primary Tract Course
The tract has a multi-segment path:
- Segment 1: Runs superiorly in the intersphincteric plane for ~2 cm at 6 o'clock
- Segment 2: Pierces the external sphincter at 6 o'clock at the level of the puborectalis sling (~4.5 cm from anal verge), with a sphincter defect of ~5.5 mm
- Segment 3: Travels posteriorly ~2.0 cm below the tip of the coccyx
This path - beginning intersphincteric, then traversing the external sphincter - is the defining anatomy of a transsphincteric fistula (Parks Type 2). The level at the puborectalis sling means a significant portion of the external sphincter is involved, classifying this as a high transsphincteric fistula.
3. Branching Pattern
After reaching the post-coccygeal space, the tract ramifies into multiple branches - a key feature of complex fistula disease:
| Branch | Direction | Size | Status |
|---|---|---|---|
| Right paramedian caudal | Posterior, opens into intergluteal cleft (R side, 6 o'clock) | ~2.0 cm long, 3.0 mm wide | Open |
| Right paramedian cranial | Posterior, opens into intergluteal cleft (R side, 6 o'clock) | ~5.0 cm long, 5.0 mm wide | Partially fibrosed |
| Left paramedian | Posterior | ~1.6 cm long | Blind-ending |
4. Associated Pilonidal Abscess
A small pilonidal abscess (~1.5 x 1.1 cm) is present in the left paramedian intergluteal cleft at the Co1 level (coccyx level 1). Importantly, there is suspected communication between this abscess and the cranial right paramedian branch - meaning the fistula network and the pilonidal disease may be interconnected.
5. Additional Negative Findings (clinically reassuring)
- No horseshoe abscess - rules out deep post-anal space involvement with bilateral ischiorectal extension
- No supralevator extension - rules out the more dangerous suprasphincteric or extrasphincteric pattern
- No ischiorectal fossa involvement on either side
- No pelvic collection
- Prostate, seminal vesicles, bony structures, and pelvic soft tissues all normal
- Mild inflammatory fat stranding only (expected with active fistula)
Radiologist's Impression (Final Diagnosis)
Recurrent complex posterior transsphincteric fistula-in-ano with multiple secondary branching tracts and associated pilonidal abscess/sinus showing probable communication with the fistulous network, on a background of chronic postoperative fibrotic change.
Clinical Significance
Parks Classification - Type 2 (Transsphincteric):
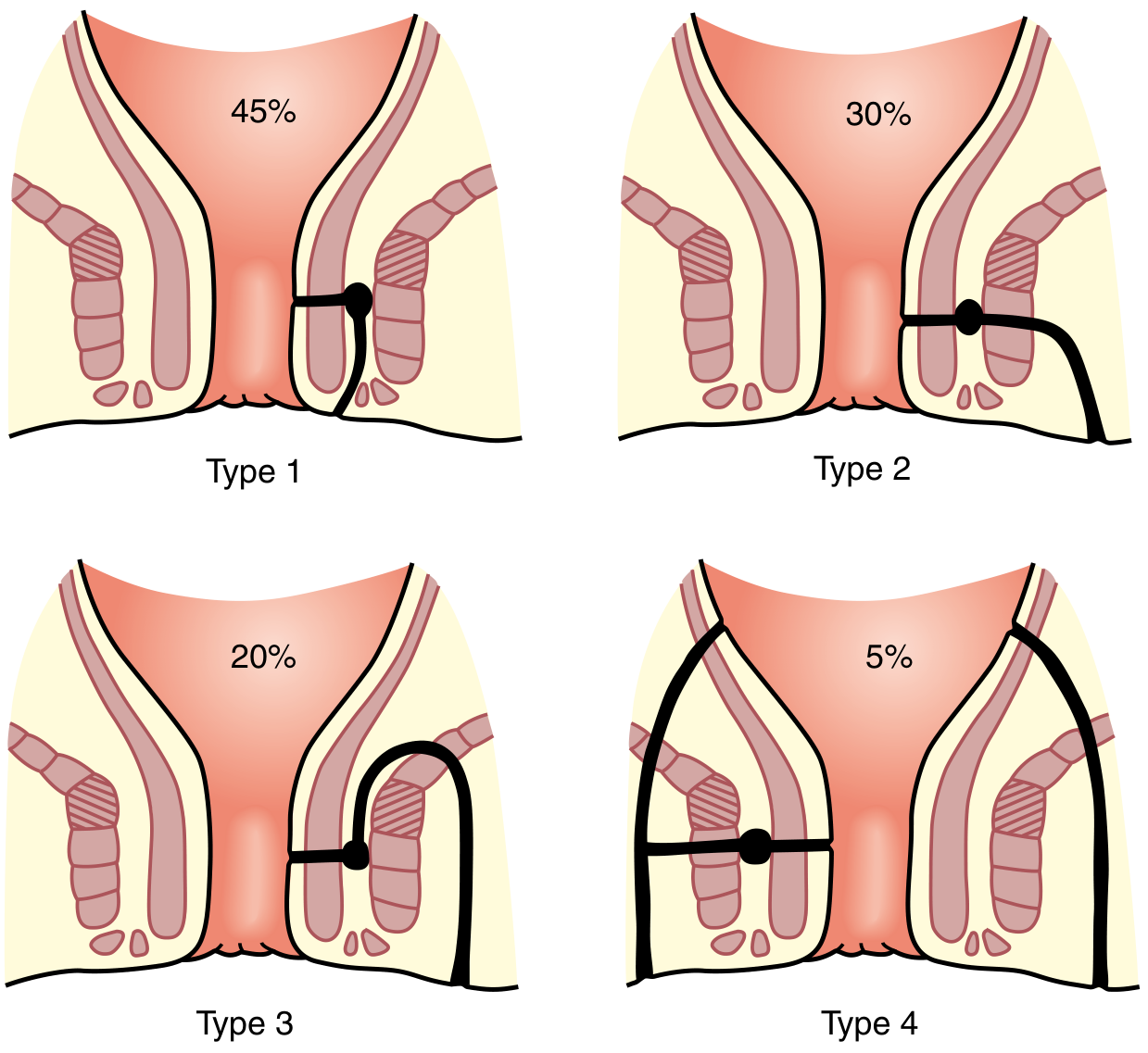
This patient's fistula is Parks Type 2 (transsphincteric), which accounts for ~30% of anal fistulae. The tract traverses the external sphincter, which is what makes it a complex fistula and surgically challenging. The additional features that elevate complexity here include:
- High level - at the puborectalis sling (high transsphincteric)
- Multiple secondary branching tracts (3 branches)
- Recurrent disease - background of prior fistula surgery
- Marked peripheral fibrosis from chronic postoperative change
- Associated pilonidal abscess with possible communication to the main network
Per surgical textbook guidance (Current Surgical Therapy, 14e; Sabiston Surgery), high transsphincteric fistulae are classified as complex fistulas because:
- Simple fistulotomy carries a high risk of fecal incontinence (division of the puborectalis sling or upper external sphincter is not tolerated)
- Recurrence rates are significantly higher than for low fistulae
- Sphincter-preserving techniques are required
Surgical Management Options to Discuss with the Colorectal Surgeon
| Procedure | Notes |
|---|---|
| Draining seton | First-stage or definitive; controls sepsis, maintains drainage, allows tract fibrosis |
| LIFT (Ligation of Intersphincteric Fistula Tract) | Sphincter-preserving; suitable for transsphincteric fistula |
| Mucosal/anorectal advancement flap | Closes internal opening without sphincter division |
| Fibrin glue / collagen plug | Adjunct options; lower success rates but sphincter-preserving |
| Separate treatment of pilonidal abscess | The pilonidal component (and its probable fistula communication) will need to be addressed - typically by excision or unroofing |
Simple fistulotomy (lay-open) is NOT appropriate here because the fistula is high transsphincteric and division of the puborectalis sling/upper external sphincter would cause fecal incontinence.
Summary for the Patient
This MRI confirms that the fistula has recurred after prior surgery, has become more complex with multiple branches, and is now connected to a small abscess near the tailbone (pilonidal abscess). This is a challenging surgical problem that requires a colorectal surgeon experienced with complex fistulae. The scan is very well done - it has mapped out all the tracts precisely, which is essential information the surgeon will need before planning any procedure. Clinical correlation and examination under anaesthesia (EUA) will typically be the next step.
- Sabiston Textbook of Surgery, p. 2163
- Current Surgical Therapy 14e, p. 347
This is a shared conversation. Sign in to Orris to start your own chat.