What is nystagmus
Reading File
Finding Sources
Searching the Web
nystagmus definition types causes clinical features
Reading File
Reading File
Reading File
Here is a comprehensive overview of nystagmus drawn from multiple authoritative textbooks:
Nystagmus
Definition
Nystagmus is an involuntary, rhythmic, biphasic oscillation of the eyes in which at least one phase is slow. It reflects an imbalance in one or more of the systems that normally maintain stable gaze. — Bradley and Daroff's Neurology in Clinical Practice
Types
1. Jerk Nystagmus (more common)
- Alternates between a slow (pathological) phase and a fast corrective (saccadic) phase in the opposite direction
- Named by the direction of the fast phase (e.g., "right-beating" nystagmus = fast phase beats to the right)
- Subtypes based on the shape of the slow-phase velocity profile:
- Linear (constant velocity) slow phase → vestibular dysfunction (peripheral or central)
- Decreasing velocity exponential → "leaky" neural integrator; gaze-paretic nystagmus
- Increasing velocity exponential → typically central origin; classic in infantile nystagmus syndrome (INS)
2. Pendular Nystagmus
- Oscillations are roughly equal in both directions — no clear fast or slow phase
- Central (brainstem or cerebellar) in origin
- On lateral gaze, may convert to jerk type with fast phase toward the side of gaze
Mechanism
Nystagmus arises from dysfunction in one of three gaze-stabilization systems:
- Vestibulo-ocular reflex (VOR) — maintains foveal fixation during head movement
- Neural integrator — holds eyes in eccentric gaze positions
- Smooth pursuit / fixation centers — keeps gaze steady in the primary position
The slow phase is the pathological component; the fast phase is a corrective brainstem response returning the fovea to target. — Ganong's Review of Medical Physiology
Causes
| Category | Examples |
|---|---|
| Drugs / Toxins | Alcohol, barbiturates, phenytoin, other antiepileptics, sedatives (most common cause of jerk nystagmus) |
| Peripheral vestibular | Labyrinthitis, benign paroxysmal positional vertigo (BPPV), temporal bone fracture |
| Central (brainstem/cerebellum) | Stroke, multiple sclerosis, head injury, brain tumors, cerebellar lesions |
| Congenital / Infantile | Infantile nystagmus syndrome (INS) — present at birth |
| Normal (physiologic) | End-gaze nystagmus at extreme lateral gaze — bilateral, disappears moving toward midline |
Localizing Value
| Nystagmus Type | Lesion Location |
|---|---|
| Downbeat nystagmus | Bilateral cervicomedullary junction (flocculus) |
| Upbeat nystagmus | Bilateral pontomesencephalic junction |
| Pendular nystagmus | Medial medulla, paramedian pons, deep cerebellum |
| Periodic alternating (PAN) | Floor of 4th ventricle |
| Gaze-paretic nystagmus | Neural integrator (brainstem) |
— Bradley and Daroff's Neurology in Clinical Practice
Key Symptoms
- Oscillopsia — the illusion that the visual environment is moving/oscillating; caused by poor foveation during nystagmus
- Blurred vision — from inability to maintain stable retinal image
- Vertigo — especially with vestibular (peripheral) causes
Clinical Testing
- Examine eyes first in primary position, then with up, down, and lateral gaze
- Peripheral vestibular nystagmus is suppressed by visual fixation; Frenzel lenses remove fixation to unmask it
- Caloric testing (COWS mnemonic): Cold water → nystagmus beats to Opposite side; Warm water → nystagmus beats to Same side. Used to test vestibular integrity.
Dissociated / Disconjugate Nystagmus
Oscillations differ between the two eyes — seen with brainstem lesions or spasmus nutans. Monocular nystagmus may be associated with amblyopia or vision loss.
Treatment
There is no universal cure. Management is directed at the underlying cause:
- Stopping offending drugs
- Surgical removal of tumors
- Rectus muscle surgery for select cases
- Botulinum toxin (temporary; paralyzes extraocular muscles)
— Ganong's Review of Medical Physiology; Adams and Victor's Principles of Neurology
Benign paroxysmal positional vertigo
Finding Sources
Searching the Web
benign paroxysmal positional vertigo BPPV pathophysiology diagnosis treatment 2024
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Here is a comprehensive review of Benign Paroxysmal Positional Vertigo (BPPV):
Benign Paroxysmal Positional Vertigo (BPPV)
Definition
BPPV is the most common peripheral vestibular disorder and the most common cause of vertigo overall. It is characterised by brief, severe episodes of vertigo triggered by specific changes in head position relative to gravity.
— Cummings Otolaryngology; Bailey and Love's Short Practice of Surgery
Epidemiology
- Accounts for 17–40% of patients with peripheral vestibular disease — nearly twice as frequent as Ménière's disease
- Incidence: ~64 per 100,000 population (Minnesota study)
- Mean age of onset: 4th–5th decade; incidence increases with age
- Twice as common in women
- ~25% of cases have an identifiable cause; the majority are idiopathic
- First described by Bárány (1921); Dix and Hallpike (1952) described the classical diagnostic maneuver
Pathophysiology
Two mechanisms are recognized:
1. Canalithiasis (most common)
Free-floating otoconia (calcium carbonate crystals) dislodged from the utricular macula migrate into a semicircular canal — most commonly the posterior canal (~85–90% of cases). Head position changes cause gravity-driven movement of this debris, deflecting the cupula and triggering vertigo and nystagmus. This explains:
- The latency (time for debris to begin moving)
- The brief duration (<1 min; debris settles at the canal's lowest point)
- Fatigability (debris disperses with repetition)
- Reversal of nystagmus on returning to upright (retrograde debris movement)
2. Cupulolithiasis (less common)
Otoconia adhere to the cupula of the posterior canal, making it abnormally gravity-sensitive. This causes nystagmus with little or no latency that persists as long as the provocative position is maintained.
Canals affected:
| Canal | Frequency |
|---|---|
| Posterior semicircular canal | ~85–88% |
| Horizontal (lateral) canal | ~12% |
| Superior (anterior) canal | ~2% |
Causes / Predisposing Factors
- Idiopathic (most common — ~48% in large surveys)
- Closed head trauma (most common known cause)
- Vestibular neuritis (~15% later develop BPPV)
- Prolonged bed rest
- Ménière's disease
- Infections
- Post-surgical (stapedectomy, dental procedures, cochlear implantation)
- Migraine-associated ischemia (especially in children)
Clinical Features
- Severe vertigo triggered by head position changes — rolling in bed, lying down, rising, looking up, bending forward
- Duration: seconds to <1 minute (patient perception often overestimates duration)
- No hearing loss, tinnitus, or neurological symptoms (distinguishes BPPV from other causes)
- Episodes often cluster in time, separated by remissions of months
- Chronic lightheadedness and imbalance between acute attacks, worse in the morning
- Patient often identifies the offending side: "dizziness only when I roll to the right"
Diagnosis — Dix-Hallpike Maneuver
The diagnosis is confirmed by observing the classical nystagmus pattern during the Dix-Hallpike maneuver:
Technique: Patient sits on table; head turned 45° toward the suspected ear; patient is rapidly lowered to supine with head hanging over edge. Eyes are observed.
Classical findings (posterior canal BPPV):
- Latency — nystagmus onset after a few seconds
- Vertical upbeat + torsional component — superior poles of eyes beat toward the lower (affected) ear
- Duration <1 minute
- Vertigo invariably accompanies nystagmus
- Fatigable — nystagmus diminishes with repeated testing
- Reversal of nystagmus direction on returning to upright
Pure vertical nystagmus on Dix-Hallpike is not BPPV.
Horizontal canal BPPV is tested with the supine roll test (head turned rapidly side to side in supine position) — produces horizontal nystagmus, either geotropic (beating toward the down ear) or ageotropic (beating away).
The Epley (Canalith Repositioning) Maneuver
The primary treatment for posterior canal BPPV. Success rates: 50–90% in controlled studies.
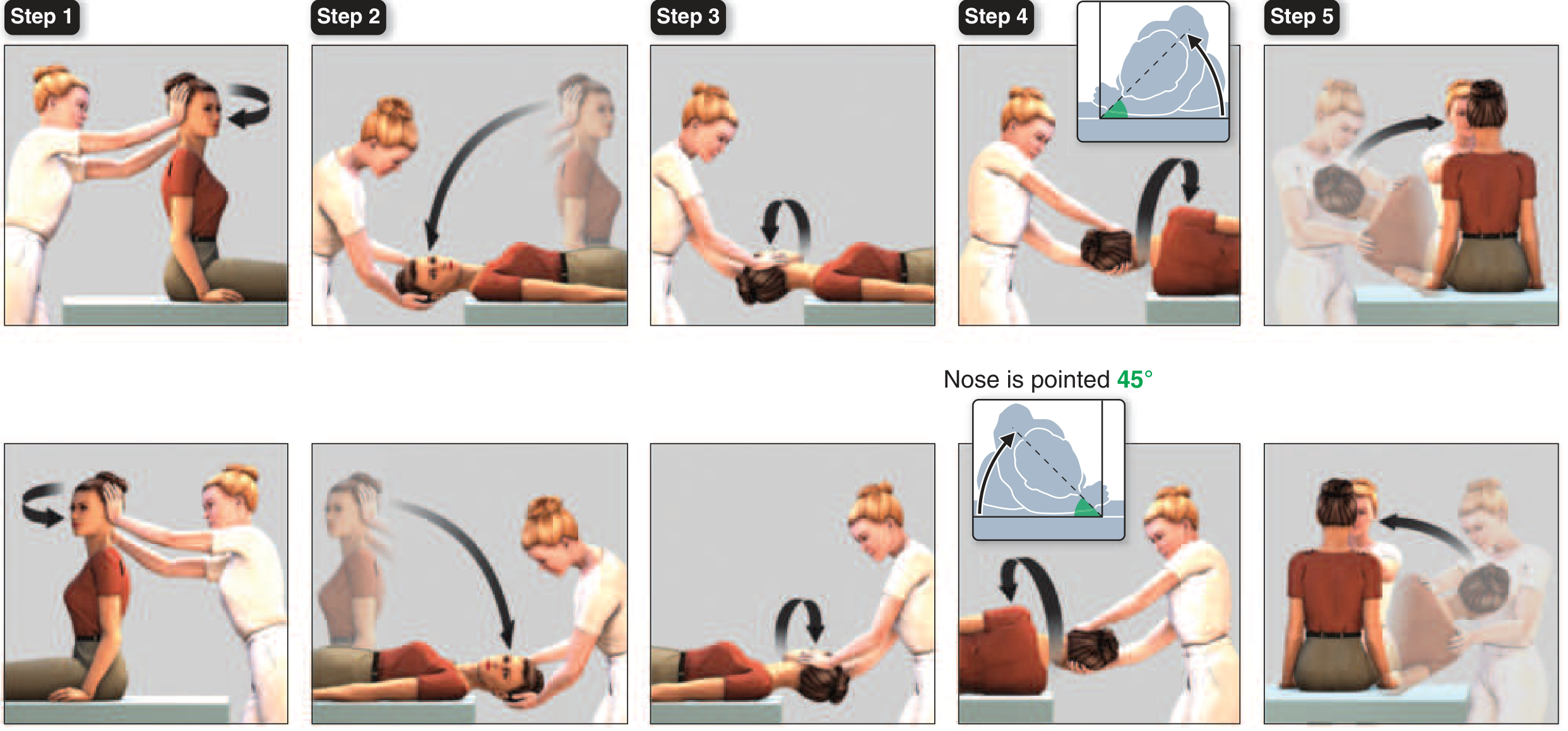
Steps (right posterior canal BPPV):
- Head turned 45° toward affected ear (seated)
- Patient lowered to head-hanging position — hold ≥30 s until nystagmus resolves
- Head turned 90° to opposite side — hold 30 s
- Patient rolled onto their side, head turned another 90° nose-down 45° — hold 30 s
- Patient sits upright; maneuver repeated to confirm resolution
— Harrison's Principles of Internal Medicine (2025); Rosen's Emergency Medicine
For horizontal canal BPPV: The barbecue roll — patient rotates head in 90° increments away from the involved side, progressing through prone.
Treatment Summary
| Approach | Details |
|---|---|
| Epley maneuver | First-line for posterior canal BPPV; 50–90% success |
| Barbecue roll / Gufoni maneuver | Horizontal canal BPPV |
| Semont (liberatory) maneuver | Alternative to Epley |
| Home exercises | Patients taught self-Epley for refractory/recurrent cases |
| Vestibular suppressants | NOT routinely recommended; reserved for ED patients actively vomiting or unable to tolerate repositioning maneuvers |
| Surgery | Rare; posterior canal occlusion for refractory cases |
Guidelines specifically advise against routine use of vestibular suppressant medications (e.g., meclizine, dimenhydrinate) as they do not address the underlying mechanism.
Prognosis
- Typically self-limiting — spontaneous resolution occurs in most patients
- Recurrence rate is significant (~15–50% within 1 year)
- Posterior canal BPPV rarely bilateral
Sources: Cummings Otolaryngology; Harrison's Principles of Internal Medicine 22E (2025); Bailey & Love's Surgery; Rosen's Emergency Medicine; Bradley and Daroff's Neurology
Benign paroxysmal positional vertigo definition
Based on the authoritative textbooks already consulted in this session:
Definition of BPPV
Benign Paroxysmal Positional Vertigo (BPPV) is the most common peripheral vestibular disorder, characterised by brief, recurrent episodes of severe vertigo provoked by specific changes in head position relative to gravity.
It is caused by free-floating otoconia (calcium carbonate crystals) that have been dislodged from the utricular macula and migrated into one of the semicircular canals — most commonly the posterior canal. When head position changes, gravity moves these crystals within the canal, deflecting the cupula and triggering vertigo and nystagmus.
Breaking down the name:
| Term | Meaning |
|---|---|
| Benign | Not life-threatening; typically self-limiting |
| Paroxysmal | Sudden, brief attacks (seconds, always <1 minute) |
| Positional | Triggered by specific head position changes (rolling in bed, looking up, bending) |
| Vertigo | Illusion of rotational movement |
— Harrison's Principles of Internal Medicine 22E (2025); Cummings Otolaryngology; Bailey & Love's Short Practice of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.