I now have all the information needed to construct a comprehensive, well-referenced differential diagnosis. Let me synthesize everything.
Top 15 Differential Diagnosis
Patient Summary: 51F, non-pregnant, post-vaginal hysterectomy, overweight, PMH: GERD, IBS, bilateral ovarian cysts, depression. Meds: esomeprazole, aspirin, bupropion, alprazolam, acetaminophen/hydrocodone. Key CT finding: area of increased attenuation within the mesenteric fat in the RUQ surrounding an area of diminished attenuation, arising from the transverse colon — this is the pathognomonic "fat ring sign" / "pseudocapsule" pattern.
🥇 #1 — Mesenteric Panniculitis / Sclerosing Mesenteritis (Most Likely)
Rationale: The CT description is the textbook imaging signature of this condition. Increased attenuation within mesenteric fat surrounding a central area of diminished attenuation (the "fat halo" or "fat ring sign") arising near the transverse colon is the defining CT finding of mesenteric panniculitis/sclerosing mesenteritis. This is a spectrum of disease — from predominantly inflammatory (mesenteric panniculitis) to fibrotic (sclerosing/retractile mesenteritis). It occurs in middle-aged to older adults (median age ~65), affects females, and presents with abdominal pain, nausea/vomiting, altered bowel habits, and sometimes a palpable mass. It can manifest as an acute or chronic disorder.
CT hallmarks:
- Hyperattenuating mesenteric fat mass (−40 to −60 HU vs. normal −100 to −160 HU)
- "Fat ring sign" = preserved hypodense fat surrounding mesenteric vessels coursing through fibrosis
- "Tumor pseudocapsule" = hypodense zone around the associated mass
- Encapsulated mesenteric lymph nodes < 10 mm
- No bowel wall invasion; no vascular involvement
The RUQ/transverse colon location is atypical (most cases center on the small-bowel mesentery to the left), which makes confirmation/biopsy more critical here.
Schwartz's Principles of Surgery, 11th Ed.; Grainger & Allison's Diagnostic Radiology; Sleisenger & Fordtran's GI and Liver Disease
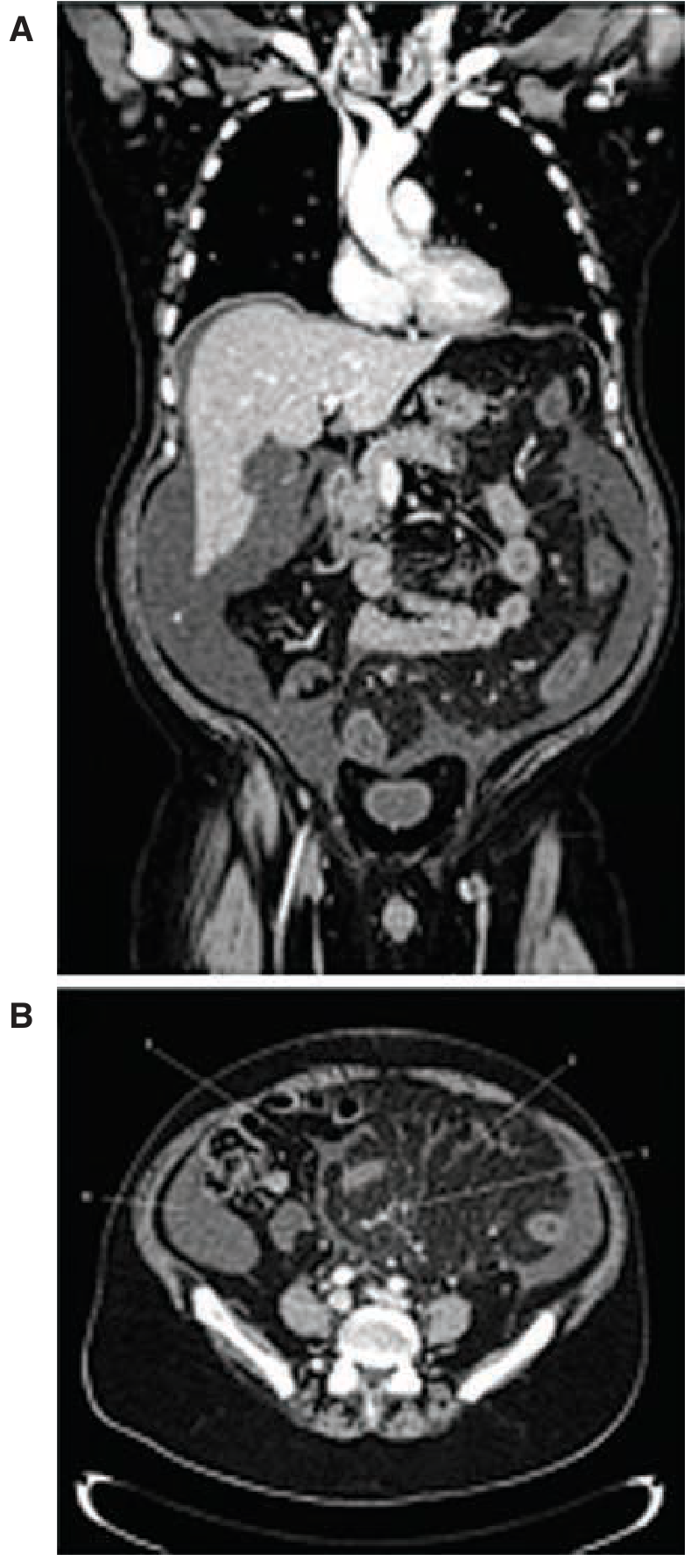
CT scan findings of sclerosing mesenteritis — coronal (A) and axial (B) views. Arrows indicate area of higher density and edema in the inflamed mesentery. — Schwartz's Principles of Surgery, 11th Ed.
#2 — Epiploic Appendagitis
Rationale: Epiploic appendagitis occurs when a small fat-filled peritoneal appendage along the colon undergoes torsion or spontaneous venous thrombosis, producing focal fat inflammation with a central hyperdense dot on CT — exactly matching the "area of increased attenuation surrounding an area of diminished attenuation." Though classically in the sigmoid or ascending colon, it does occur along the transverse colon. Presents with acute, severe, localized abdominal pain. NSAIDs (aspirin) may partially mask inflammation. It is generally self-limiting and managed conservatively.
CT hallmarks: Oval fat-density lesion (−60 to −130 HU) with hyperattenuating ring; central hyperdense dot (thrombosed vessel); no bowel wall thickening.
#3 — Omental Infarction
Rationale: Segmental omental infarction presents with acute, severe abdominal pain and a CT finding nearly identical to the description — a fatty mass with increased peripheral attenuation and a central area of fat necrosis/diminished density. The greater omentum overlies the transverse colon, making the RUQ a classic location. Obesity (overweight patient) is a significant risk factor due to poor vascular supply of redundant omental fat. The aspirin use does not prevent this condition.
CT hallmarks: Encapsulated fatty mass in the right abdomen with surrounding hyperattenuating stranding; central fat necrosis; adjacent to the colon.
#4 — Colonic Carcinoma (Transverse Colon)
Rationale: A malignant mass of the transverse colon can present with surrounding fat stranding and desmoplastic reaction, producing exactly the CT appearance described — a central soft-tissue mass of diminished attenuation (tumor/necrosis) surrounded by hyperattenuating fat stranding (pericolic infiltration/desmoplasia). This patient is 51 years old (screening age), overweight, taking aspirin (some chemopreventive role, but does not eliminate risk). Severe abdominal pain and nausea in this age group with a colonic mass demands malignancy exclusion.
Key distinguishing features: Luminal narrowing, mucosal irregularity, bowel obstruction signs, adenopathy, CEA elevation.
#5 — Diverticular Disease / Acute Diverticulitis (Transverse Colon)
Rationale: Transverse colon diverticulitis is uncommon (~3% of diverticulitis) but well-documented. It produces pericolonic fat stranding with increased attenuation and a central low-density abscess or inflamed diverticulum — matching the CT description precisely. Severe abdominal pain and nausea are typical. The overweight, middle-aged female profile fits. Aspirin use does not protect and may blunt fever response.
CT hallmarks: Pericolonic fat stranding, diverticula, possible pericolic abscess (diminished attenuation core), bowel wall thickening.
#6 — Mesenteric Cyst (with Inflammation or Hemorrhage)
Rationale: Mesenteric cysts can arise adjacent to the transverse colon and present with acute abdominal pain from cyst rupture, torsion, or hemorrhage into the cyst. The CT finding of a lesion with a hyperdense rim (inflammation/blood) and a central hypodense area (cyst fluid/necrosis) fits. Nausea and diffuse abdominal pain occur with cyst rupture. Post-hysterectomy patients may have altered pelvic and mesenteric anatomy increasing cyst susceptibility.
Schwartz's Principles of Surgery, 11th Ed.
#7 — Bowel Obstruction (Adhesion-Related, Post-Hysterectomy)
Rationale: This patient had a vaginal hysterectomy, creating adhesion risk. Small or large bowel obstruction from adhesions can cause severe, diffuse abdominal pain and nausea. Adjacent fat can show secondary inflammation on CT. While the CT description fits a primary mesenteric process, an adhesion-related obstruction causing downstream bowel ischemia and fat stranding is in the differential — particularly given the RUQ transverse colon location. IBS history makes functional vs. mechanical distinction critical.
#8 — Peptic Ulcer Disease / Perforated Ulcer
Rationale: This patient has GERD (esomeprazole), takes aspirin (a major ulcerogenic agent) and hydrocodone (constipating, may increase GI pressure), and has a known upper GI history. Peptic ulcer disease — including perforation — causes severe, diffuse abdominal pain and nausea. A perforated ulcer could produce secondary mesenteric and omental fat changes on CT. Her esomeprazole partially protects but does not fully prevent aspirin-induced ulcers. Peak age for peptic ulcer disease is the 50s.
Tintinalli's Emergency Medicine
#9 — Acute Pancreatitis
Rationale: Acute pancreatitis causes severe, diffuse abdominal pain with nausea and vomiting and can produce peripancreatic and mesenteric fat stranding visible on CT. The head/uncinate process of the pancreas is near the RUQ and the transverse mesocolon is a primary route of inflammatory spread. The patient takes bupropion and hydrocodone — both rarely associated with pancreatitis. IBS and GERD often accompany functional upper GI pain that can obscure earlier pancreatitis signs. Lipase/amylase would be elevated.
#10 — Acute Cholecystitis / Biliary Pathology
Rationale: The RUQ location of this CT finding places acute cholecystitis and biliary disease prominently in the differential. Gallbladder inflammation produces pericholecystic fat stranding on CT that can involve the transverse mesocolon. Obesity is a major risk factor (the "5 F's"). Severe nausea and RUQ pain radiating across the abdomen fit. The CT description, if representing pericholecystic rather than primary mesenteric inflammation, makes this diagnosis critical to exclude urgently.
#11 — Ischemic Colitis (Transverse Colon)
Rationale: The transverse colon watershed zone (splenic flexure) is the most vulnerable segment to ischemia, but the transverse colon body can also be involved. Ischemic colitis produces transmural inflammation with pericolonic fat stranding — a hyperattenuating halo around a segment of colon with possible mucosal submucosal thickening (thumbprinting). Overweight patients with cardiovascular risk factors, aspirin use (suggesting possible vascular disease), and atherosclerotic risk warrant this consideration. Severe pain and nausea are typical.
#12 — Ovarian Cyst Complication (Rupture / Hemorrhage / Torsion)
Rationale: The patient has known bilateral ovarian cysts even post-hysterectomy (ovaries preserved with vaginal hysterectomy). Ovarian cyst rupture, hemorrhagic cyst, or torsion causes acute severe abdominal pain — sometimes diffuse — with nausea/vomiting. Hemorrhagic cyst fluid or blood products can track along the right paracolic gutter to the RUQ, producing increased mesenteric/fat attenuation near the transverse colon on CT. The ovaries remain in situ after vaginal hysterectomy unless oophorectomy is explicitly performed.
Berek & Novak's Gynecology; Rosen's Emergency Medicine
#13 — Opioid-Induced Bowel Dysfunction / Narcotic Bowel Syndrome
Rationale: The patient is on acetaminophen/hydrocodone chronically. Opioid-induced bowel dysfunction and narcotic bowel syndrome cause severe, diffuse abdominal pain that paradoxically worsens with increased opioid dosing — a recognized paradoxical hyperalgesia syndrome. Severe nausea is prominent. The underlying mesenteric CT finding may be incidental (mesenteric panniculitis found on workup) while the functional pain is opioid-mediated. Bupropion, while an antidepressant, has no GI protective effects and can cause GI upset.
#14 — Mesenteric Lymphoma / Mesenteric Metastases
Rationale: The CT finding of increased mesenteric fat attenuation with a central hypodense area near the transverse colon is a known mimic of mesenteric panniculitis and raises concern for mesenteric lymphoma (particularly non-Hodgkin lymphoma), mesenteric carcinoid, or metastatic disease. Lymphoma can produce the "misty mesentery" sign. Colon carcinoma, ovarian carcinoma (given known bilateral ovarian cysts), or gastric malignancy can all metastasize to the transverse mesocolon. The depression, weight considerations, and this CT pattern mandate malignancy workup.
Grainger & Allison's Diagnostic Radiology; Goldman-Cecil Medicine
#15 — Hydrocodone/NSAID-Exacerbated IBS / Functional Abdominal Pain Disorder
Rationale: The patient's underlying IBS is a diagnosis of exclusion that can produce severe, diffuse abdominal pain and nausea, particularly in the context of medication effects. Aspirin and opioids both dysregulate gut motility and visceral hypersensitivity. Bupropion has serotonergic/noradrenergic activity and can alter gut function. Depression (treated with bupropion/alprazolam) is strongly associated with heightened visceral pain perception (brain-gut axis dysregulation). However, the CT finding of mesenteric fat abnormality distinguishes a likely organic etiology from pure functional pain — IBS should be revisited only after structural causes are excluded.
Harrison's Principles of Internal Medicine 22E; Sleisenger & Fordtran's
Summary Table
| Rank | Diagnosis | CT Finding Fit | Clinical Fit | Priority |
|---|
| 1 | Mesenteric Panniculitis / Sclerosing Mesenteritis | ⭐⭐⭐⭐⭐ | ⭐⭐⭐⭐ | URGENT workup |
| 2 | Epiploic Appendagitis | ⭐⭐⭐⭐⭐ | ⭐⭐⭐⭐ | Usually self-limiting |
| 3 | Omental Infarction | ⭐⭐⭐⭐⭐ | ⭐⭐⭐⭐ | Usually self-limiting |
| 4 | Colonic Carcinoma | ⭐⭐⭐⭐ | ⭐⭐⭐⭐ | URGENT colonoscopy |
| 5 | Diverticulitis (Transverse Colon) | ⭐⭐⭐⭐ | ⭐⭐⭐⭐ | Antibiotics ± surgery |
| 6 | Mesenteric Cyst (complicated) | ⭐⭐⭐ | ⭐⭐⭐ | Surgery if ruptured |
| 7 | Bowel Obstruction (adhesion) | ⭐⭐⭐ | ⭐⭐⭐⭐ | Surgical consult |
| 8 | Perforated Peptic Ulcer | ⭐⭐⭐ | ⭐⭐⭐⭐ | Emergency surgery |
| 9 | Acute Pancreatitis | ⭐⭐⭐ | ⭐⭐⭐ | Lipase/amylase |
| 10 | Acute Cholecystitis | ⭐⭐⭐ | ⭐⭐⭐⭐ | RUQ US |
| 11 | Ischemic Colitis | ⭐⭐⭐ | ⭐⭐⭐ | Colonoscopy |
| 12 | Ovarian Cyst Complication | ⭐⭐⭐ | ⭐⭐⭐⭐ | Pelvic US |
| 13 | Narcotic Bowel Syndrome | ⭐ | ⭐⭐⭐⭐ | Opioid taper |
| 14 | Mesenteric Lymphoma / Mets | ⭐⭐⭐⭐ | ⭐⭐ | Tissue biopsy |
| 15 | IBS / Functional Pain | ⭐ | ⭐⭐⭐ | Diagnosis of exclusion |
Recommended Next Steps
- Colonoscopy — mandatory to evaluate the transverse colon mass/lesion (exclude carcinoma, diverticular disease, ischemia)
- RUQ ultrasound — exclude acute cholecystitis, biliary pathology, evaluate ovaries
- Lipase, amylase, LFTs, CBC, CMP — pancreatitis, biliary, metabolic workup
- Pelvic ultrasound (transvaginal) — characterize bilateral ovarian cysts, exclude torsion/hemorrhage
- Surgical/GI consultation — for possible laparoscopic biopsy of the mesenteric lesion if colonoscopy is unrevealing
- Consider MRI abdomen — better soft-tissue characterization of mesenteric mass; low T1/T2 signal in sclerosing mesenteritis helps differentiate from lymphoma
- Malignancy workup: CEA, CA-125, CA 19-9
Key clinical anchor: The CT finding of increased mesenteric fat attenuation with central diminished attenuation ("fat ring sign" / "pseudocapsule") arising from the transverse colon is the radiologic signature of mesenteric panniculitis/sclerosing mesenteritis — but this is a diagnosis of exclusion and malignancy (lymphoma, colonic carcinoma, metastatic disease) must be actively ruled out, as these produce identical imaging appearances.
Sources: Schwartz's Principles of Surgery 11e; Grainger & Allison's Diagnostic Radiology; Sleisenger & Fordtran's GI and Liver Disease; Tintinalli's Emergency Medicine; Harrison's Principles of Internal Medicine 22E; Berek & Novak's Gynecology; Rosen's Emergency Medicine; AJR "Misty Mesentery" review; PMC Mesenteric Panniculitis Clinical Review