Fetal hepatic calcification
Reading File
Finding Sources
Finding Sources
Searching PubMed
"fetal hepatic calcification" ultrasound
Finding Sources
Finding Sources
Reading Article
PMID: 39467273
Finding Sources
Finding Sources
Searching PubMed
"fetal liver calcifications" outcome management
Reading File
Finding Sources
Reading Article
PMID: 40713069
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a detailed overview of fetal hepatic calcification:
Fetal Hepatic Calcification (Fetal Liver Calcifications - FLCs)
Definition
Fetal liver calcifications (FLCs) are areas of abnormal brightness (echogenic foci) in the fetal liver parenchyma or on its peritoneal surface, often with posterior acoustic shadowing. They are a subset of echogenic abdominal lesions encountered on prenatal ultrasound.
Incidence
- Echogenic hepatic lesions: approximately 5-6 per 10,000 pregnancies
- Overall prevalence estimated at 5-10 per 10,000 births
- Cholelithiasis (gallstones): ~0.5%, almost always in the 3rd trimester
Etiology and Pathogenesis
FLCs can be classified by their anatomical origin and cause:
Intrahepatic Parenchymal
| Cause | Notes |
|---|---|
| TORCH infections | Toxoplasmosis, CMV, rubella, herpes - most important infectious cause |
| Hemangioma | Most common benign cause of isolated intrahepatic echogenic foci |
| Hamartoma | Benign developmental lesion |
| Thrombosis/vascular events | In utero portal or hepatic vein thrombus leading to dystrophic calcification |
| Aneuploidy | Trisomy 13, 18, 21, triploidy |
| Malignancy | Very rare; hepatoblastoma, metastatic neuroblastoma |
On Hepatic Peritoneal Surface
| Cause | Notes |
|---|---|
| Meconium peritonitis | In utero bowel perforation causes chemical peritonitis; secondary inflammatory response produces foreign body granulomas and calcification on the liver surface |
Diagnostic Features on Ultrasound
- Appear as hyperechoic (bright) foci in the fetal abdomen or liver
- May produce posterior acoustic shadowing (classic for true calcification)
- Location matters:
- Intrahepatic (parenchymal) - infection, vascular, tumor
- Peritoneal surface of liver - meconium peritonitis
- Gallbladder fossa - cholelithiasis
Important caveat: Harmonic-enhanced imaging and higher-frequency transducers can overexaggerate echogenicity. Harmonic imaging should be disabled before confirming the finding, as apparent echogenic lesions may disappear when harmonics are turned off.
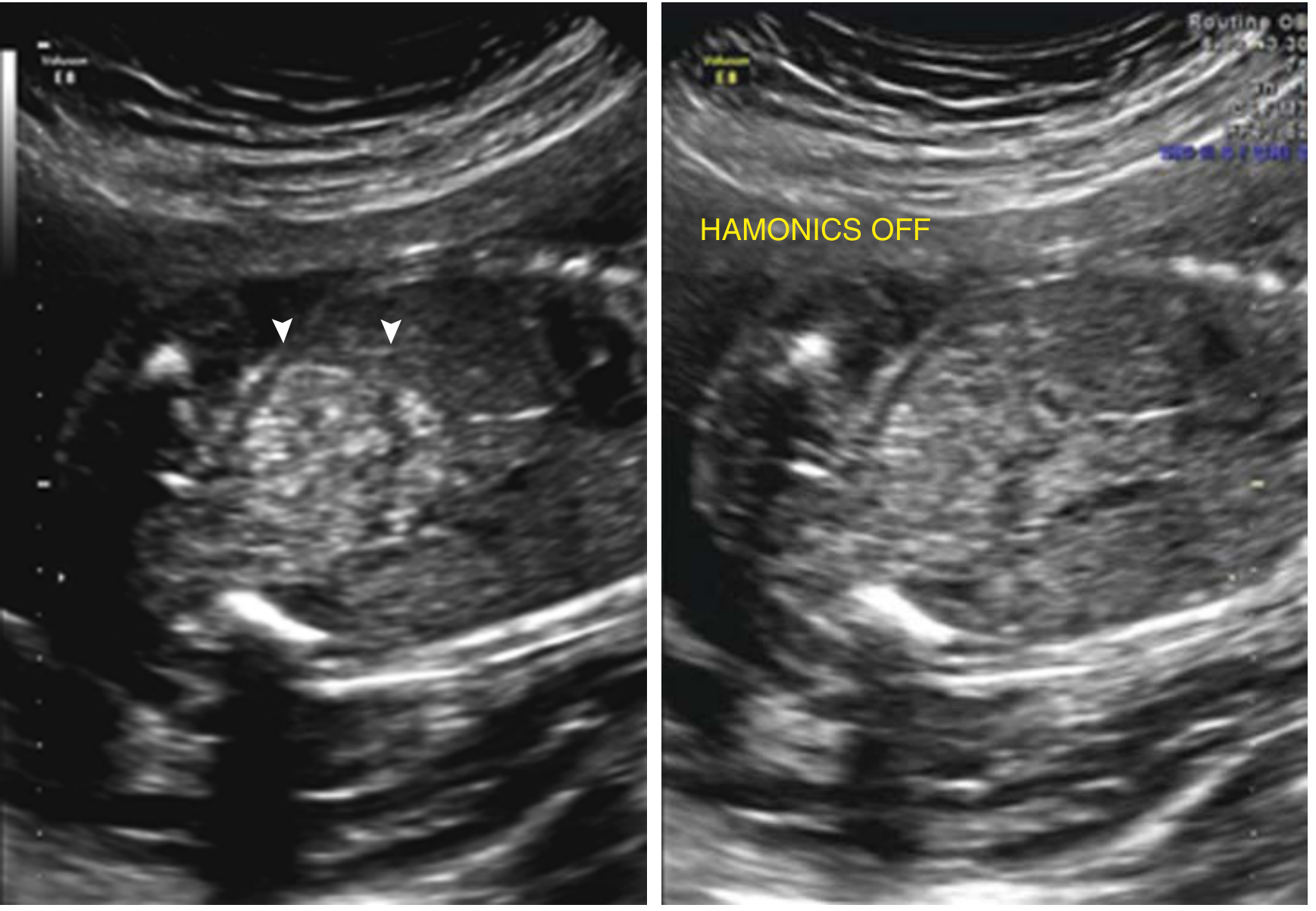
Harmonic imaging can falsely exaggerate echogenicity - always confirm with harmonics disabled.
Associated Anomalies
- Multiple intrahepatic echogenic foci are more often associated with TORCH infection or aneuploidy (poorer prognosis)
- Isolated singular lesions are more likely benign (e.g., hepatic hemangioma)
- All fetal organs should be assessed to rule out other congenital malformations and genetic syndromes
- Look for: cerebral calcifications, ventriculomegaly, hydrops (suggest TORCH), fetal growth restriction, cardiac/renal anomalies
Key distinction:
Multiple echogenic foci in the fetal abdomen or liver are likely to be associated with infection or meconium peritonitis, whereas isolated echogenic foci are more likely benign.
Workup / Investigations
When FLCs are identified, a structured work-up should be initiated:
- Detailed anomaly scan - assess all fetal organs; rule out structural defects, cardiac anomalies, CNS involvement
- Maternal serology (TORCH titers) - IgM and IgG for toxoplasmosis, CMV, rubella, herpes; if CMV IgM positive, perform CMV avidity testing (low avidity = recent primary infection)
- Maternal STORCH screen - syphilis, toxoplasma, CMV, rubella, herpes
- Cystic fibrosis carrier status testing
- Maternal AFP and hCG - may help determine etiology and prognosis
- Fetal karyotype / chromosomal microarray - if multiple anomalies or markers of aneuploidy present
- Fetal echocardiography
- Fetal MRI - helpful when ultrasound findings are indeterminate
- Serial ultrasound - monitor fetal growth, amniotic fluid, and worsening condition; nonstress testing/biophysical profile twice weekly from 32-34 weeks if persistent echogenicity and/or fetal growth restriction
- Delivery at a tertiary care facility if persistent echogenicity, associated fetal abnormalities, or FGR is present
Prognosis
| Finding | Prognosis |
|---|---|
| Isolated singular intrahepatic echogenic lesion | Generally good outcome |
| Multiple intrahepatic lesions | More often TORCH or aneuploidy; poorer prognosis |
| Isolated FLC with normal karyotype, no infection, no CF, no FGR | Good for normal outcome |
| Coarse isolated FLCs (even large) | May still resolve with normal postnatal outcome if all investigations are negative |
- Isolated FLCs, even when coarse, do not appear to impact fetal or neonatal outcomes when potential causes are excluded (2025 BMJ Case Reports, PMID: 40713069)
- Long-term prognosis depends mostly on associated abnormalities and/or underlying disease
Neonatal Management
- Continue postnatal imaging: ultrasound, plain abdominal X-ray, upper/lower GI barium studies, MRI
- Expectant management appropriate if investigation is unremarkable
- Surgical treatment may be warranted for bowel obstruction with or without perforation, volvulus, ascites, pneumoperitoneum
- Pediatric surgery consultation as appropriate
Summary Points
- FLCs are uncommon but important prenatal ultrasound findings with a broad differential
- The key discriminator is whether they are isolated vs. multiple - isolated lesions tend to be benign while multiple lesions suggest infection or chromosomal abnormality
- A structured work-up (TORCH screen, CF carrier status, karyotype, detailed anatomy scan) is essential
- When all investigations are normal, prognosis is excellent and isolated FLCs can be managed expectantly with serial monitoring
Sources: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, p. 511-514 | Derme et al., J Clin Ultrasound 2025, PMID: 39467273 | Gomes-Pires et al., BMJ Case Rep 2025, PMID: 40713069
This is a shared conversation. Sign in to Orris to start your own chat.