Hanging , answer for PG level MD forensic level theorey and viva answer for the topic of hanging, broad classification, definitions, types, ipc vs bns, Autopsy dissection tech niques images where possible, neck dissection, signs of hanging (simonds haemorrhage etc), mechanism of death,mode and manner of death, cause of death, use reddy, parikh , knight, spitz and fischer,
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
This is a complete, PG/MD-level forensic medicine answer on Hanging, compiled directly from Reddy (2026), Parikh, Dikshit, and DiMaio. Here is a quick summary of what's covered:
What's Covered - Quick Map
| Section | Key Content |
|---|---|
| Definition | Reddy, Parikh, DiMaio verbatim |
| Classification | Complete/Partial, Typical/Atypical, Mode (Suicidal/Homicidal/Accidental/Judicial/Autoerotic/Lynching) |
| Mechanism of Death | 5 mechanisms + pressure values (Carotid 3.5 kg, Jugular 2 kg, Trachea 15 kg) |
| Mode / Manner / Cause of death | Clearly separated - important viva distinction |
| IPC vs BNS | S.309→S.226 BNS, S.302→S.103, S.174 CrPC→S.194 BNSS, S.176 CrPC→S.196 BNSS |
| Postmortem appearances | External (face, lividity, tongue, saliva) with clinical images |
| Ligature mark | Level (80/15/5%), direction, suspension peak, comparison table with strangulation |
| Autopsy neck dissection technique | Step-by-step; brain-first rule; carotid opening to mandible |
| Internal findings | Intimal tears, hyoid fracture, Simon's haemorrhages (lumbar disc), Tardieu spots |
| Antemortem vs Postmortem | Comparison table with all diagnostic criteria |
| Judicial hanging | Hangman's fracture, long drop, Table of Drops |
| Autoerotic hanging | Padding, scene features, accidental nature |
| Medicolegal questions | Suicide vs Homicide diagnostic criteria (both directions) |
| Key viva quick-facts | All high-yield numbers and exam traps |
Give me the 20 marks anser
HANGING — 20 Marks Answer (MD Forensic Medicine)
DEFINITION
Hanging is a form of violent mechanical asphyxia caused by suspension of the body by a ligature encircling the neck, the constricting force being the weight of the body itself.
(Reddy 2026): "Hanging is always suicidal in nature, unless contrary is proved beyond reasonable doubt."
The weight of the head alone (5-6 kg) is sufficient to occlude the carotid arteries (occluded by 3.5 kg) and cause death — full body suspension is NOT necessary.
CLASSIFICATION
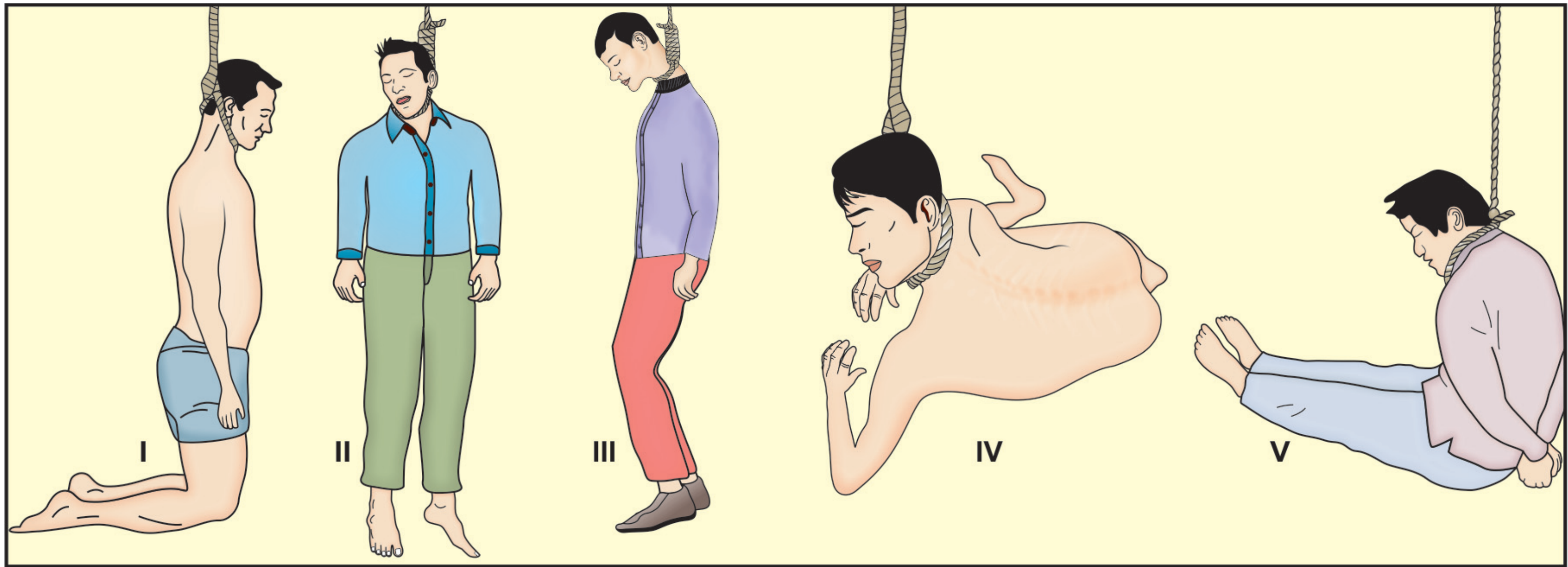
A. By Degree of Suspension (Position of Feet)
| Type | Description |
|---|---|
| Complete (Total) | Body fully suspended; no part touches the ground; entire body weight acts as constricting force |
| Partial (Incomplete) | Only head and chest off ground; toes/feet/knees/buttocks touch the ground; weight of head (5-6 kg) acts as constricting force |
Subtypes of partial hanging:
- Partial standing (toes/feet on ground)
- Sitting position
- Kneeling position
- Reclining/prone position
B. By Position of Noose/Knot
| Type | Knot Position | Ligature Mark Character |
|---|---|---|
| Typical (Classical) | Nape of neck / occiput | Oblique V-shape, apex at back |
| Atypical | Lateral (ear), anterior (chin/throat), or unusual site | Direction varies |
C. By Mode / Manner
| Mode | Description |
|---|---|
| Suicidal | Most common (~95%); virtually all hangings |
| Accidental | Children (crib cords, blind cords); autoerotic |
| Homicidal | Extremely rare; includes lynching |
| Judicial | Official capital punishment |
| Autoerotic (Sexual asphyxia) | Masochistic young males; padding under noose |
| Lynching | Mob hanging; from Captain William Lynch, USA |
| Postmortem suspension | Body hanged after death to simulate suicide |
MECHANISM OF DEATH
Critical Pressure Values (Parikh / Reddy):
| Structure | Pressure to Occlude |
|---|---|
| Jugular veins | 2 kg |
| Carotid arteries | 3.5 kg |
| Trachea | 15 kg |
| Vertebral arteries | 16.6 kg |
Five Mechanisms:
1. Cerebral ischaemia and anoxia (Most common)
Carotid artery compression → obstruction of arterial supply to brain → cerebral ischaemia → death.
Evidence: (a) Persons with tracheostomy below the noose have hanged themselves — airway was patent yet death occurred; (b) Vomitus found in bronchi BELOW level of neck constriction.
2. Cerebral venous congestion
Jugular vein compression → venous outflow obstruction → raised ICP → engorgement → petechial haemorrhages → death.
3. Airway obstruction
Direct tracheal compression OR elevation/posterior displacement of tongue and floor of mouth against posterior pharyngeal wall; epiglottis folded over laryngeal inlet.
4. Vagal inhibition / Reflex cardiac arrest
Pressure on carotid sinus or vagus nerve → reflex cardiac arrest. Instantaneous death; no asphyxial signs found at autopsy (Knight: ~50% of mechanical asphyxia deaths in his series showed NO classical signs).
5. Spinal cord injury
Free fall and sudden jerk (judicial/long drop hanging) → fracture-dislocation at C2-C3 or C3-C4 → spinal cord stretching/tearing → instantaneous death. Heart may continue beating 15-20 minutes.
Any combination of the above may act simultaneously.
MODE, MANNER AND CAUSE OF DEATH
Mode of Death (Physiological process)
- Cerebral ischaemia (most common)
- Asphyxia
- Vagal inhibition / cardiac arrest
- Spinal cord injury (judicial)
Manner of Death (Circumstances)
- Suicidal (most common)
- Accidental
- Homicidal (very rare)
Cause of Death (To be certified at autopsy)
- "Asphyxia due to hanging"
- Or: "Cerebral ischaemia due to compression of carotid vessels by ligature (hanging)"
- Judicial: "Fracture-dislocation of cervical spine with spinal cord injury due to hanging"
IPC vs BNS (Bharatiya Nyaya Sanhita 2023)
| Subject | Old IPC / CrPC | New BNS / BNSS | Provision |
|---|---|---|---|
| Attempt to suicide | S.309 IPC | S.226 BNS | Effectively decriminalised by Mental Healthcare Act 2017 (S.115) — presumption of severe stress; must refer to mental health care, not punish |
| Abetment of suicide | S.306 IPC | S.108 BNS | Up to 10 years + fine |
| Murder (homicidal hanging) | S.302 IPC | S.103 BNS | Punishment for murder |
| Culpable homicide | S.304 IPC | S.105 BNS | Culpable homicide not amounting to murder |
| Hurt | S.319 IPC | S.114 BNS | Definition of hurt |
| Police inquest (unnatural death) | S.174 CrPC | S.194 BNSS | Mandatory police inquest in all hanging deaths |
| Magistrate's inquest | S.176 CrPC | S.196 BNSS | Compulsory when death in police custody or if police inquest is unsatisfactory |
| Capital punishment method | S.354(5) CrPC | S.473(5) BNSS | Execution by hanging is the prescribed method |
Key viva point: Under Mental Healthcare Act 2017 Section 115, a person who attempts suicide is presumed to be under severe stress — the State has a duty to provide care and rehabilitation, NOT prosecution.
POSTMORTEM APPEARANCES
External Appearances
General asphyxial signs:
- Cyanosis of face, lips, fingernails (may be absent in rapid carotid compression)
- Petechial haemorrhages (Tardieu spots) — conjunctiva, sclera, face (especially in partial hanging)
- Congested, prominent eyeballs
- Tongue — protrudes, dark brown/black (venous congestion + drying)
- Bloody froth from nose/mouth (pulmonary oedema)
Specific to hanging:
- Neck stretched; head tilted to side opposite the knot
- Face pale in complete hanging (carotid compressed before jugular); face congested in partial hanging (jugular compressed, vertebral artery supply continues)
- Salivary dribble from corner of mouth on the side opposite to the knot (ligature pressure on salivary glands)
- Postmortem lividity in glove-and-stocking distribution (forearms, hands, legs) due to dependent position
- Scrotal/penile congestion; possible seminal emission
- Middle ear haemorrhage (rupture of small vessels)

The Ligature Mark
The single most important external sign.
Shape: Inverted V or U-shaped oblique furrow; directed upward toward the knot; does NOT completely encircle the neck — gap present at the knot site (Suspension Peak).
Level:
- 80% — above thyroid cartilage (between larynx and chin)
- 15% — at the level of thyroid cartilage
- 5% — below thyroid cartilage (partial hanging)
Appearance:
- Fresh: Pale, yellowish, parchment-like, dry, depressed furrow
- Later: Yellow-brown, firm, well-demarcated
- Rope: Deep, well-defined with mirror-image of weave pattern
- Soft material (dupatta, towel): Pale, poorly defined, no bruising
Edges: Narrow zone of congestion/haemorrhage above and below at the deepest point — this is due to lateral displacement of blood from under maximum pressure, NOT a sign of vital reaction.
Suspension Peak: Where the vertical rope leaves the neck — no mark present here. This is the key differential from ligature strangulation.


Ligature Mark: Hanging vs Strangulation (Exam Table)
| Feature | Hanging | Ligature Strangulation |
|---|---|---|
| Direction | Oblique, ascending to knot | Horizontal / transverse |
| Circumference | Incomplete (gap at knot) | Complete around neck |
| Level | Usually above thyroid cartilage | At or below thyroid cartilage |
| Suspension peak | Present | Absent |
| Knot impression | May be present | Usually at back |
| Ecchymoses | Rare | More common |
| Usual manner | Suicide / Accidental | Homicide |
AUTOPSY DISSECTION TECHNIQUE — NECK
Pre-dissection:
- Do NOT remove the noose before scene documentation and photography
- Document noose: nature, composition, width, type of knot, mode of application
- To remove: cut opposite to the knot, preserve both cut ends with tape; do NOT untie the knot — it is evidence
- Slip noose over the head or cut it; submit with body to mortuary
Order of Dissection (Critical):
Remove brain FIRST — then dissect neck (to drain cranial blood and prevent artefactual haemorrhage into neck structures from brain weight)
Layer-by-Layer Neck Dissection:
- Skin and superficial fascia — examine groove, measure width, depth, colour, direction
- Platysma — look for tears/haemorrhage
- Sternomastoid and strap muscles — tears, haemorrhage
- Carotid sheath and arteries — open fully up to mandible — look for intimal tears (horizontal, multiple, at different levels, near knot — traction type — DIAGNOSTIC of antemortem hanging)
- Internal jugular veins — congestion
- Vagus nerve — note any contusion
- Larynx and trachea — petechiae, hyperaemia, compression
- Hyoid bone — fracture at junction of inner 2/3 and outer 1/3 of greater cornu (rare below 40 yrs)
- Thyroid cartilage — superior horns
- Intervertebral discs (lumbar) — Simon's haemorrhages
INTERNAL FINDINGS
Neck:
- Platysma / sternomastoid: Torn fibres (especially in judicial hanging)
- Carotid intimal tears: Horizontal traction tears with subintimal haemorrhage — diagnostic of antemortem hanging; multiple levels; seen especially with long drop
- Lymph nodes above and below ligature: Congested, haemorrhagic — vital reaction indicator
- Hyoid bone fracture: 0-20% average; junction of inner 2/3 and outer 1/3 of greater cornu; displaced outward; periosteum torn on inner side only; blood clot at fracture site if antemortem
- Thyroid cartilage: Posterior horn fractures from pressure on thyrohyoid ligament
- Deep muscles at base of tongue: Bruising (crushing against hard palate by ligature)
- Epiglottis / larynx / trachea: Petechiae, hyperaemia, congestion
Brain:
- Usually normal; or pale (carotid occlusion) or congested (jugular occlusion)
- Subarachnoid effusions common
- Cerebral oedema variable
Lungs:
- Congested, oedematous; bloody serum on section
- Subpleural ecchymoses (Tardieu spots)
- Pale if constriction at end of inspiration
Heart:
- Right side — distended with dark fluid blood
- Left side — relatively empty
- Subpericardial ecchymoses possible
Simon's Haemorrhages (High-yield viva):
Bleeding into the outer layers (annulus fibrosus) of intervertebral discs of lumbar vertebrae — seen as red stripes between vertebral bodies in bodies suspended for a prolonged period. Due to gravitational stretching of the spinal column. Seen in both antemortem and prolonged postmortem suspension.
(Reddy 2026, p.339)
Spinal Column (Judicial Hanging):
- Hangman's fracture — fracture-dislocation at C2-C3 or C3-C4
- Spinal cord stretched, torn, lacerated
- Pons and medulla may be contused
ANTEMORTEM vs POSTMORTEM HANGING
| Indicator | Antemortem Hanging | Postmortem Suspension |
|---|---|---|
| Carotid intimal tears | Present (traction-type, horizontal) | Absent |
| Subintimal haemorrhage | Present | Absent |
| Lymph node congestion above/below mark | Present | Absent |
| Deep muscle haemorrhage under groove | Present | Absent (dry, white, bloodless zone) |
| Hyperaemia of trachea/epiglottis | Present | Absent |
| Petechiae on serous surfaces | Present | Absent |
| Skin petechiae on limbs | Present | Present (postmortem hypostasis) |
| Histology of groove | Vital reaction (neutrophils, vascular response) | No vital reaction |
| Simon's haemorrhages | Present (prolonged) | Can be present |
Key: Postmortem petechiae can only appear on skin of limbs (due to dependent blood pooling); petechiae on serous surfaces (pleura, pericardium) indicate antemortem asphyxia.
MEDICOLEGAL QUESTIONS
1. Was death due to hanging?
(i.e., was the suspension antemortem or postmortem?)
Diagnose antemortem hanging by:
- Carotid intimal tears + subintimal haemorrhage
- Vital reaction in neck groove (histology)
- Congested/haemorrhagic lymph nodes above and below mark
- Hyperaemia of epiglottis/trachea
- Exclusion of other cause of death at autopsy
2. Was it Suicidal, Homicidal, or Accidental?
Features of Suicide (Parikh / Reddy):
- No signs of struggle at scene or on body
- Accessible ligature and suspension point (person could have reached it)
- Knot within reach (lateral or anterior neck)
- Suicide note in ~25% of cases
- History of depression, mental illness (psychological autopsy)
- Face and hands free (may tie hands to prevent change of mind — does NOT exclude suicide)
- Farewell arrangements made by deceased
Features Suspicious of Homicide (Reddy / Parikh):
- Signs of struggle — disturbed furniture, defensive wounds
- Knot at back of neck (inaccessible to deceased)
- Mouth gagged
- Limbs tied (especially hands behind back)
- Injuries inconsistent with self-infliction
- Evidence of stupefaction by drugs/alcohol (toxicology)
- Torn or disarranged clothing
- Crescentic abrasions near ligature (throttling attempts)
- Other injuries suggesting assault before suspension
Accidental hanging: Children (cord entanglement), autoerotic individuals (padding under noose, pornographic material at scene, partial nudity)
JUDICIAL HANGING
- Method of capital punishment — S.473(5) BNSS (formerly S.354(5) CrPC)
- Table of Drops used — drop length inversely proportional to body weight
- Knot at angle of jaw (sub-auricular position gives best results)
- Drop of 6-8 feet; momentum causes fracture-dislocation of C2-C3
- Hangman's fracture — bilateral pedicle fractures of C2
- Death instantaneous; heart continues 15-20 minutes; muscle jerks persist
- Extensive sternomastoid tears; transverse carotid intimal tears
FATAL PERIOD
| Condition | Fatal Period |
|---|---|
| Judicial hanging (long drop) | Instantaneous (heart beats 15-20 min) |
| Suicidal hanging (no drop) | 5-8 minutes |
| Loss of consciousness | Within 10-15 seconds of complete carotid compression |
HIGH-YIELD VIVA QUICK FACTS
| Fact | Answer |
|---|---|
| Most common cause of death in hanging | Cerebral ischaemia (NOT asphyxia) |
| Most common manner | Suicide |
| Carotid occlusion pressure | 3.5 kg |
| Jugular occlusion pressure | 2 kg |
| Tracheal compression pressure | 15 kg |
| Weight of head | 5-6 kg |
| Ligature mark above thyroid | 80% of cases |
| Hyoid fracture average | 0-20% (recent series: rare) |
| Hyoid fracture site | Junction of inner 2/3 and outer 1/3 of greater cornu |
| Simon's haemorrhages | Lumbar intervertebral disc haemorrhage; prolonged suspension |
| Suspension peak | Absent ligature mark at knot site |
| Saliva dribble direction | Opposite side to the knot |
| Pale face vs congested face | Complete hanging → pale; Partial hanging → congested |
| Neck dissection rule | Remove brain first, then neck |
| Carotids opened up to | Level of mandible |
| IPC 309 → BNS | Section 226 (effectively decriminalised) |
| IPC 174 CrPC → BNSS | Section 194 BNSS (police inquest) |
| Capital punishment method BNS | Hanging (S.473(5) BNSS) |
| Knight's observation | 50% mechanical asphyxia deaths had NO classical signs (cardiac arrest) |
| Hanging is always... | Suicidal unless contrary proved beyond reasonable doubt |
Sources: KS Narayan Reddy — Essentials of Forensic Medicine & Toxicology, 36th ed. 2026, pp. 334-342 | Parikh's Textbook of Medical Jurisprudence, pp. 202-210 | PC Dikshit Textbook of FMT, pp. 291-302 | DiMaio's Forensic Pathology 3rd ed. | Knight's Forensic Pathology
how to document ligature material, mention also opinion for post mortem report, explain modes of death better
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have everything needed. Let me compile the focused, detailed answer.
DOCUMENTATION OF LIGATURE MATERIAL, POSTMORTEM REPORT OPINION & MODES OF DEATH IN HANGING
PART 1 — DOCUMENTATION OF LIGATURE MATERIAL
This is a medico-legally critical step. A ligature is primary physical evidence and must be documented with the same precision as a wound.
Step 1 — At the Scene (Before Touching the Body)
Before the body is cut down or the noose removed, record the following in the inquest report / scene notes:
- Type of material — rope, electrical cord, wire, dupatta, sari, belt, tie, trouser cord, dhoti, bedsheet, nylon cord, chain, etc.
- Where it is attached — ceiling fan hook, roof beam, window grill, door handle, tree branch, etc. (note accessibility)
- Position of the knot — lateral, posterior, anterior, or sub-auricular
- Direction of suspension — whether rope goes vertically upward or obliquely
- Height of suspension point from ground (measure)
- Height of body from ground to feet (measure)
- Photograph — full view and close-up of noose in situ, knot, and suspension point
Step 2 — Removing the Ligature (Critical Technique)
Golden Rule: Never untie the knot. Never remove the noose by pulling over the head.
Correct method:
- Support the body before cutting
- Cut the ligature at the point diametrically opposite to the knot (so the knot remains fully intact)
- Secure the two cut ends separately with adhesive tape or string — label them "cut end A" and "cut end B"
- Slip the loop over the head OR cut and remove; preserve knot intact
- Submit the entire ligature with the body to the mortuary as a sealed exhibit
Step 3 — Detailed Description at Autopsy (What to Record)
Describe the ligature under the following 9 parameters (DiMaio / Dikshit):
| Parameter | What to Record |
|---|---|
| 1. Nature / material | Rope, cloth, wire, cord, belt, dupatta, electrical wire, etc. |
| 2. Composition / texture | Natural (cotton, jute, hemp) / synthetic (nylon, polyester); braided, twisted, woven, flat; smooth or rough surface |
| 3. Colour | Single or multicolour; any staining (blood, saliva, paint) |
| 4. Width / diameter | Measure in centimetres (width of flat material or diameter of rope) |
| 5. Length | Total length of the loop; length from knot to suspension point |
| 6. Type of noose | Fixed loop (non-adjustable) or running/slip-knot (tightens with weight) |
| 7. Knot type and position | Simple knot, reef knot, slip knot, granny knot; position on neck (lateral/posterior/anterior); number of turns |
| 8. Mode of application | Single loop or multiple turns around neck; does it completely encircle or partially? |
| 9. Condition | Intact, frayed, broken, stained with blood/saliva/foreign material |
Also note:
- Any fibres, paint, or debris on the ligature (transfer evidence from beam/hook)
- Any fingerprints (refer to fingerprint expert)
- Any knot complexity — a complex or unusual knot inconsistent with the victim's skill level raises suspicion of homicide
- Whether there is a single noose or double/triple application
Step 4 — Match Ligature to Ligature Mark
After documenting the ligature, compare it with the mark on the neck:
- Width of ligature vs width of groove — should approximately match
- Pattern of weave/texture vs impression on skin — mirror image in a rope groove
- If rope broke and body found on ground — match the free rope ends to confirm continuity
- Look for groove marks on the beam/hook matching the texture/width of the rope
Step 5 — Preservation as Exhibit
- Dry the ligature gently at room temperature (do NOT use heat)
- Place in a brown paper bag (NOT plastic — plastic causes decomposition and artefact)
- Seal, label, and sign with: case number, date, body identification, and autopsy surgeon's name
- Hand over to the Investigating Officer under proper receipt/acknowledgment
- Document in the column of "Articles Handed Over" in the postmortem report
PART 2 — OPINION IN THE POSTMORTEM REPORT
The postmortem report must answer the three medico-legal questions clearly and concisely in the Opinion column.
Structure of Opinion (Standard Format)
A well-written PM opinion in hanging cases should state:
"In my opinion, death in this case was due to asphyxia as a result of hanging [or: cerebral ischaemia due to compression of neck vessels by ligature/hanging].
The manner of death appears to be suicidal [or: consistent with suicide / cannot be excluded as homicidal — depending on findings].
The cause of death is: Asphyxia due to hanging."
The Three Opinions Required:
Opinion 1 — Cause of Death
State the immediate cause and the underlying mechanism:
| Scenario | COD Statement |
|---|---|
| Typical suicidal hanging (no drop) | "Asphyxia due to hanging" |
| When carotid compression is dominant | "Cerebral ischaemia due to compression of carotid arteries by ligature (hanging)" |
| When vagal inhibition suspected (sudden death, no asphyxial signs) | "Cardiac inhibition (vagal) due to hanging" |
| Judicial/long drop hanging | "Fracture-dislocation of cervical vertebrae (C2-C3) with spinal cord injury due to judicial hanging" |
| Delayed death after rescue | "Hypoxic encephalopathy/aspiration pneumonia — complication of hanging" |
Opinion 2 — Manner of Death
State whether: Suicidal / Homicidal / Accidental — and support it:
"The findings are consistent with suicidal hanging in view of:
(a) oblique ligature mark with suspension peak; (b) no signs of struggle or defensive injuries; (c) ligature knot accessible to the deceased; (d) postmortem lividity consistent with hanging posture; (e) no other injuries indicative of assault."
OR
"Homicidal hanging cannot be excluded in view of: (a) ligature knot tied at the back of neck, (b) presence of injuries inconsistent with self-infliction, (c) hands tied behind back."
Opinion 3 — Time Since Death (Estimated)
Based on: postmortem changes (rigor mortis, lividity, decomposition), stomach contents, ambient temperature.
Articles to Be Mentioned in PM Report:
At the end of the opinion, always mention:
"The following articles are handed over to the Investigating Officer under receipt: 1. Ligature material (rope/dupatta/etc.) — sealed in paper envelope 2. Viscera — preserved in saturated saline for chemical analysis [if poisoning suspected/routine] 3. Blood sample — for alcohol/toxicology 4. Nail clippings, hair samples [if struggle suspected]"
PART 3 — MODES OF DEATH IN HANGING (Detailed Explanation)
The term "Mode of Death" refers to the physiological/pathophysiological process by which the vital functions cease. It is distinct from:
- Cause of death — the disease or injury that started the chain (e.g., hanging)
- Manner of death — the circumstances (suicide/homicide/accident)
Mode 1 — Cerebral Ischaemia (Most Common Mode)
Mechanism:
- The ligature compresses the carotid arteries (occluded by just 3.5 kg pressure)
- This occurs BEFORE the airways close (trachea needs 15 kg to compress)
- Reduced arterial blood reaching the brain → cerebral ischaemia → anoxic brain injury → unconsciousness → death
- Consciousness lost in 10-15 seconds; death in 3-5 minutes
Autopsy clues:
- Brain may appear pale (bloodless)
- Relatively less asphyxial signs (face may be pale)
- Carotid intimal tears with subintimal haemorrhage
- Petechiae may be absent or sparse
Proof this is the dominant mechanism (Parikh):
- (a) Cases of persons with permanent tracheostomy below the noose who died by hanging — airway was completely patent throughout, yet death occurred
- (b) Vomitus found in bronchi BELOW the level of neck constriction — proves airway was open, breathing occurred below the noose even while dying
Why does this happen fast? — The noose, once applied above the larynx (which is the most common position), compresses both carotids simultaneously with only the body weight. The vertebral arteries, buried deep between cervical vertebrae, are partly protected — but even partial reduction of cerebral blood flow rapidly produces unconsciousness.
Mode 2 — Cerebral Venous Congestion
Mechanism:
- Jugular veins are occluded by just 2 kg (even less than carotid pressure)
- Venous outflow from brain blocked → venous blood accumulates in cranial cavity → raised intracranial pressure
- Simultaneously arterial inflow continues (vertebral arteries) → blood pools in the head → capillaries rupture → petechial haemorrhages (Tardieu spots)
- Progressive venous engorgement → cerebral oedema → brain herniation → death
When is this the dominant mode?
- In partial hanging — the noose is applied with less force (only head weight); jugular veins are compressed first/more than carotids; vertebral artery supply continues
- In atypical hanging with soft, broad material that cannot compress the deeper carotids effectively
Autopsy clues:
- Congested, cyanosed face
- Prominent petechiae — conjunctiva, face, sclera, skin of neck above ligature
- Congested, bulging eyeballs
- Protruding, congested tongue — dark, cyanotic
- Lungs — congested and oedematous
- Brain — engorged, venous
Key teaching point: In complete hanging, the carotid (arterial) occlusion dominates — face is pale. In partial hanging, the jugular (venous) occlusion dominates — face is congested and petechiae are prominent. This is why the face appearance differs between complete and partial hanging.
Mode 3 — Asphyxia (Airway Obstruction)
Mechanism:
- The noose forces the root of tongue upward and backward against the posterior pharyngeal wall
- The epiglottis folds over the laryngeal inlet, blocking the airway
- Alternatively, direct tracheal compression (requires 15 kg — rarely achieved in non-judicial hanging)
- Result: Air cannot enter the lungs → oxygen in blood falls → carbon dioxide rises → respiratory distress → convulsive stage → exhaustion → death
Stages of death by asphyxia (classical teaching):
- Dyspnoea (increased respiratory effort, cyanosis begins) — 0-60 sec
- Convulsive stage (tonic-clonic seizures, loss of consciousness) — 1-2 min
- Apnoea (respiratory failure) — 2-3 min
- Terminal gasping (agonal breaths) — brief
- Cardiac arrest — 4-5 minutes total
Autopsy clues:
- Classical asphyxial triad — cyanosis + petechiae + congestion
- Lungs — pale if noose caught at end of inspiration; congested/oedematous if at end of expiration
- Subpleural/subpericardial Tardieu spots (ecchymoses from rupture of distended capillaries)
- Dark, fluid, unclotted blood in right heart
- Bladder may be emptied (relaxation of sphincters)
- Seminal emission (relaxation of reproductive sphincters)
Why is asphyxia NOT the most common mode in hanging? (Exam trap):
- The trachea requires 15 kg pressure to compress
- In most hangings the body weight acts obliquely; the larynx is displaced but not mechanically crushed
- The carotid arteries and jugular veins are occluded long before the trachea is effectively compressed
- Hence pure airway obstruction as the sole mode is relatively rare
Mode 4 — Vagal Inhibition (Reflex Cardiac Arrest)
Mechanism:
- Pressure on the carotid sinus (at carotid bifurcation) or vagus nerve sheath by the noose
- Stimulation of baroreceptors in the carotid sinus → reflex vagal outflow → sudden cardiac arrest
- Alternatively: catecholamine surge (fear, struggling, apprehension) sensitizes the myocardium to vagal stimulation
- Alcohol intoxication, hypersensitive carotid sinus, emotion all predispose
Key features:
- Instantaneous or very rapid death — faster than asphyxia
- Few or NO classical asphyxial signs — no petechiae, no cyanosis, no congestion (Knight's observation: ~50% of mechanical asphyxia deaths in his series showed NO classical signs)
- No significant hypoxia has time to develop
- Blood remains fluid, heart is found in near-normal state
Why important?
- Explains cases where a person is found dead after a very short time of hanging with minimal external signs
- Explains deaths in children who get briefly caught in a cord
- Explains some karate-blow and mugging deaths (carotid sinus pressure without ligature)
- Explains why the absence of asphyxial signs does NOT exclude death by hanging
Autopsy findings:
- Minimal or absent petechiae
- Face may be pale or normally coloured
- Ligature mark present (important)
- Cause of death is established by exclusion (ligature mark + position + no other cause)
Mode 5 — Spinal Cord Injury / Brainstem Injury
Mechanism (Judicial / Long Drop Hanging):
- Drop of 5-8 metres creates significant momentum
- Sudden stop at the end of the drop → violent extension and lateral flexion of the neck
- Fracture-dislocation at C2-C3 or C3-C4 ("Hangman's fracture" — bilateral fracture of pedicles/neural arch of C2)
- Spinal cord is stretched, lacerated, or transected
- Brainstem (pons, medulla) may be directly contused
- Instantaneous unconsciousness and death
Features:
- Heart may continue to beat for 15-20 minutes (cardiac centre in medulla preserved transiently or via residual activity)
- Limb twitching and muscle jerks occur after death (spinal reflex activity below the lesion)
- Massive tearing of neck muscles and vessels
- Neck may be elongated dramatically; occasionally near-decapitation if drop is excessive
- No asphyxial signs (death is instantaneous)
Table of Drops (judicial hanging):
| Body weight | Drop length |
|---|---|
| Heavier person | Shorter drop |
| Lighter person | Longer drop |
| (Inverse relationship to deliver consistent energy to the neck) |
Summary Comparison Table — Modes of Death in Hanging
| Mode | Speed of Death | Asphyxial Signs | Face Appearance | Mechanism | Most common in |
|---|---|---|---|---|---|
| Cerebral ischaemia (carotid) | 10-15 sec unconscious; death ~3-5 min | Mild or absent | Pale | Arterial occlusion | Complete hanging (most common overall) |
| Cerebral venous congestion (jugular) | Slower | Prominent petechiae | Congested, cyanosed | Venous occlusion | Partial hanging |
| Asphyxia (airway) | ~4-5 min | Classical triad present | Cyanosed | Airway block | Rare in isolation; combined |
| Vagal inhibition | Instantaneous | Absent | Pale / normal | Reflex cardiac arrest | Sensitive carotid sinus; fear/alcohol |
| Spinal cord injury | Instantaneous | Absent | Normal | Cord transection | Judicial hanging / long drop only |
Delayed Causes of Death After Rescue from Hanging (Reddy 2026):
When a person is rescued from hanging but dies later, the mode of death changes:
- Aspiration pneumonia (vomitus/blood aspirated)
- Pulmonary oedema (neurogenic or hypoxic)
- Laryngeal oedema (post-compression swelling — may cause delayed airway obstruction)
- Hypoxic encephalopathy (brain damaged from period of ischaemia)
- Cerebral infarction (from carotid dissection)
- Cerebral abscess / softening
- Retropharyngeal abscess, cervical cellulitis
- Epileptiform convulsions, amnesia, dementia (sequelae)
Le Faci's Sympathicae (Bonus Viva Point)
A sign mentioned by Reddy — "Le Faci's sympathicae" — refers to asymmetry of the face/pupils due to pressure on the cervical sympathetic chain by the noose, producing a unilateral Horner's syndrome (partial ptosis, miosis, anhidrosis) on the side of the knot. This is a sign of antemortem hanging.
Sources: KS Narayan Reddy 36th ed. 2026, pp. 334-342 | Parikh's Textbook of Medical Jurisprudence, pp. 202-210 | PC Dikshit Textbook of FMT, pp. 291-302 | DiMaio's Forensic Pathology 3rd ed.
This is a shared conversation. Sign in to Orris to start your own chat.