human anatomy neurovascular structure from basic to clinical
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
Reading File
Searching the Web
neurovascular anatomy clinical correlations overview medical school 2024
Here is a comprehensive guide to human anatomy neurovascular structures - from basic to clinical - organized for medical school exam preparation.
Human Anatomy: Neurovascular Structures - Basic to Clinical
Sources: Neuroanatomy through Clinical Cases 3rd Ed., Gray's Anatomy for Students, Neuroscience: Exploring the Brain 5th Ed.
PART 1: FOUNDATIONAL CONCEPTS
What Is a Neurovascular Bundle?
A neurovascular bundle is the co-travelling group of a nerve, artery, and vein (often also lymphatics) that runs together in a common fascial sheath. They travel together because they develop together embryologically and share the same connective tissue pathways. Clinically, this means that trauma, tumors, or compression at one point often affects all components simultaneously.
Key Principles
- Nerves follow arteries, and both follow bony/fascial channels
- Most peripheral nerves carry motor, sensory, AND autonomic (sympathetic) fibers
- Venous drainage often parallels the arterial supply but may diverge (e.g., cerebral veins vs. arteries)
- Watershed zones between arterial territories are most vulnerable to ischemia
PART 2: BRAIN - ARTERIAL SUPPLY
Dual Circulation System
The brain receives blood from two paired systems:
| System | Source | Territory |
|---|---|---|
| Anterior circulation | Internal carotid arteries (ICA) | Cerebral hemispheres (anterior) |
| Posterior circulation | Vertebral arteries -> basilar artery | Brainstem, cerebellum, posterior cortex |
These two systems are linked by the Circle of Willis at the base of the brain.
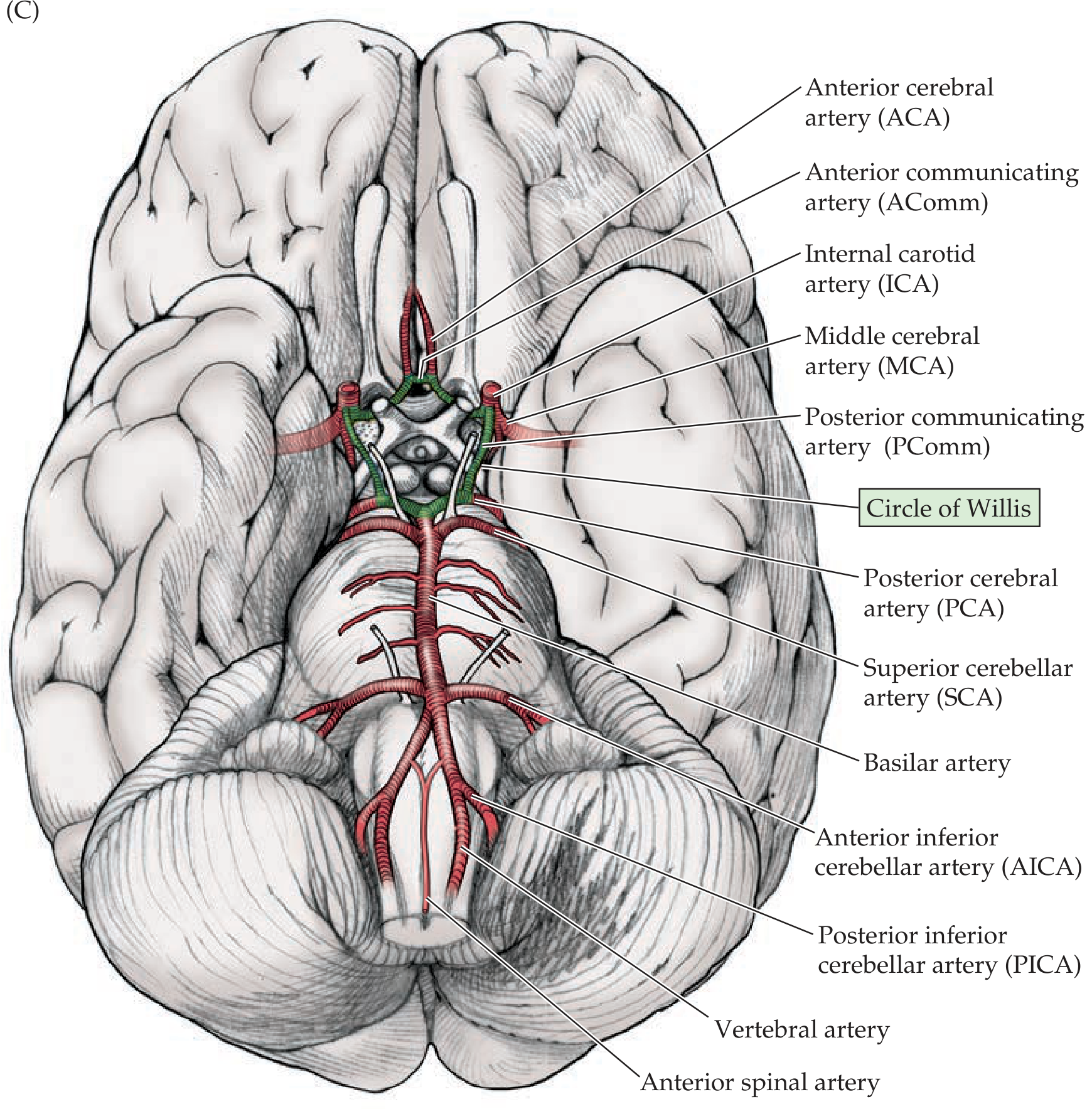
Circle of Willis - Anatomy
The circle is formed by:
- Anterior arch: ACA (left) -- AComm -- ACA (right)
- Lateral links: ICA -> PComm -> PCA (each side)
- Posterior arch: PCA (left) -- basilar -- PCA (right)
Important: A complete, full-caliber circle of Willis is present in only ~34% of individuals. Anatomical variants are common - this matters clinically during carotid surgery or occlusion.
ICA Segments - Mnemonic: OPAAM
The supraclinoid ICA gives off (in order):
- O - Ophthalmic artery (supplies retina via optic foramen)
- P - Posterior communicating artery (PComm)
- A - Anterior choroidal artery
- A - Anterior cerebral artery (ACA)
- M - Middle cerebral artery (MCA)
Three Main Cerebral Arteries & Their Territories
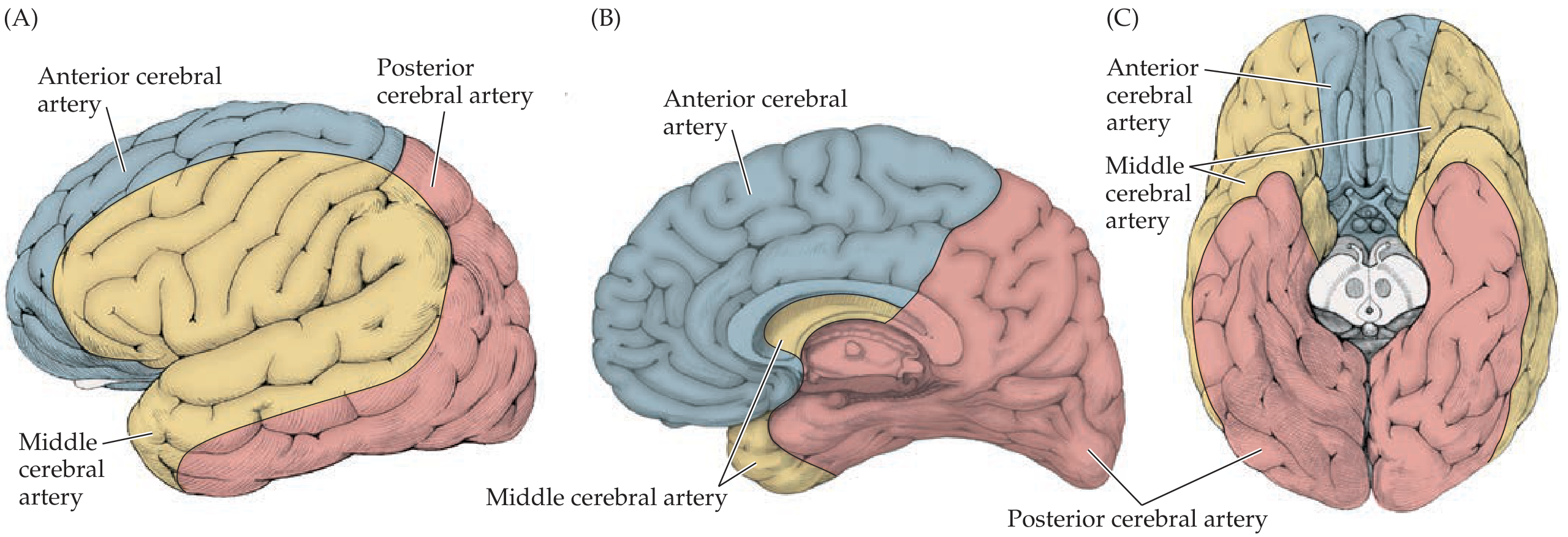
| Artery | Territory | Key Structures Supplied |
|---|---|---|
| ACA | Medial frontal + anterior parietal | Leg/foot sensorimotor cortex, supplementary motor area |
| MCA | Dorsolateral convexity | Face/arm motor/sensory, Broca's area (L), Wernicke's area (L) |
| PCA | Medial/inferior temporal + occipital | Primary visual cortex, thalamus (via perforators) |
Deep Perforating Vessels
- Lenticulostriate arteries - arise from MCA M1; supply basal ganglia + internal capsule
- Anterior choroidal artery - supplies posterior limb of internal capsule, globus pallidus, part of thalamus
- Thalamoperforator arteries - arise from proximal PCA; supply thalamus + midbrain
PART 3: SPINAL CORD - BLOOD SUPPLY
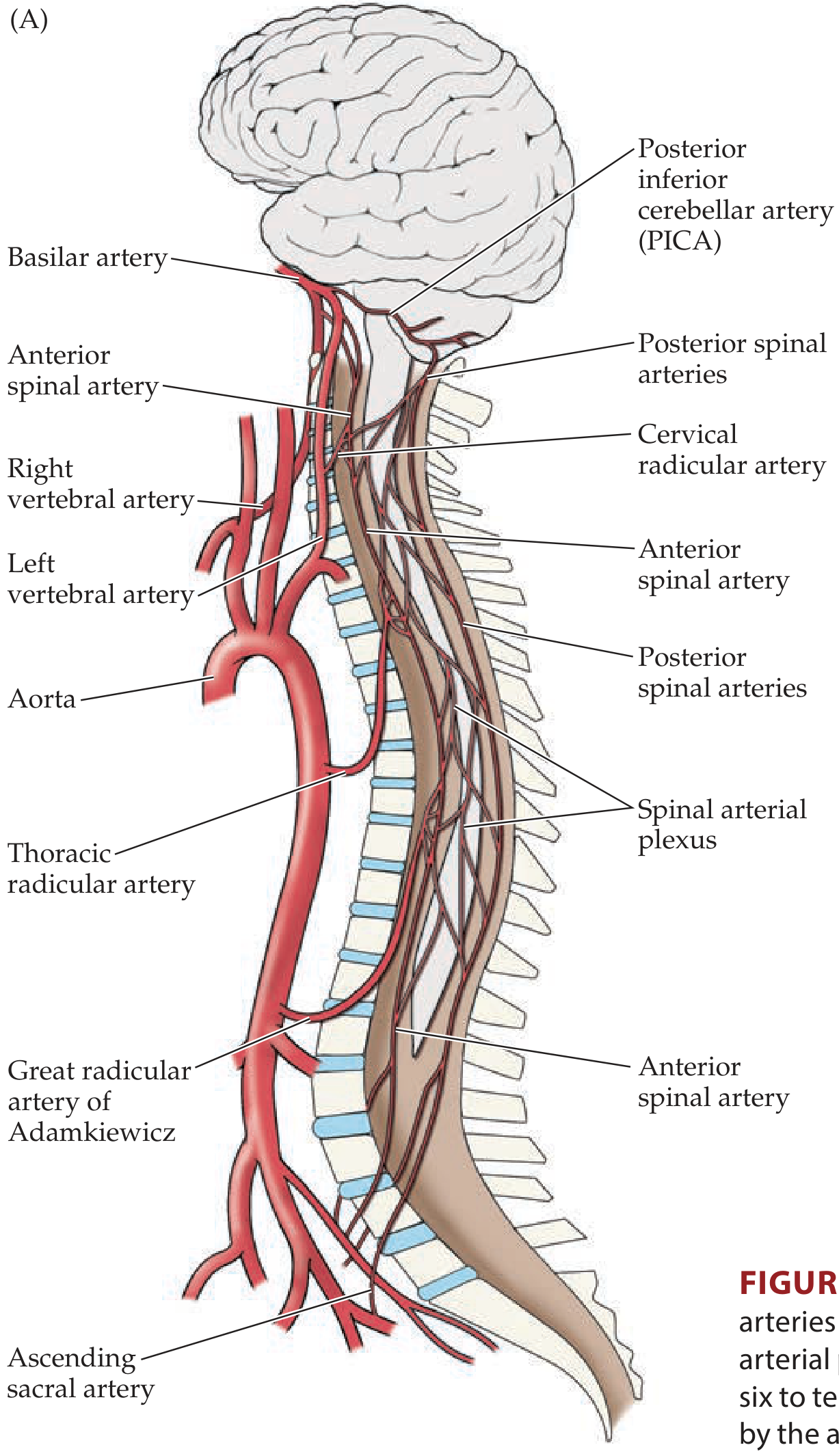
Arterial Supply
| Artery | Source | Territory |
|---|---|---|
| Anterior spinal artery (1) | Vertebral arteries | Anterior 2/3 of cord - anterior horns, lateral + anterior white matter |
| Posterior spinal arteries (2) | Vertebral or PICA | Posterior 1/3 - posterior columns + part of posterior horns |
| Radicular arteries (6-10) | Aorta, segmental branches | Reinforce spinal arteries at variable levels |
Artery of Adamkiewicz
- The great radicular artery (artery of Adamkiewicz) arises from the left side in 70-80% of people
- Located between T5-L3, most commonly at T9-T12
- Provides the major blood supply to the lumbar and sacral cord
- Clinical: Damage during thoracic aortic surgery is a leading cause of paraplegia
Vulnerable Zone
- T4-T8 is the watershed zone between the vertebral supply above and the aortic supply below
- Most susceptible to infarction during hypotension or aortic clamping
Batson's Plexus
- Epidural venous plexus (valveless) that drains the spinal cord
- Lack of valves allows retrograde flow during raised intra-abdominal pressure
- Provides a route for metastatic spread of pelvic tumors (prostate, bladder, rectal cancer) to the spine
PART 4: UPPER LIMB - BRACHIAL PLEXUS
Formation (Mnemonic: Robert Taylor Drinks Cold Beer)

Roots: Anterior rami of C5, C6, C7, C8, T1
- Pass between anterior and middle scalene muscles
- Receive gray rami communicantes from sympathetic trunk
Trunks:
- Superior = C5 + C6
- Middle = C7 alone
- Inferior = C8 + T1
Divisions: Each trunk -> anterior + posterior division (no direct peripheral nerves here)
Cords (named relative to axillary artery, 2nd part):
- Lateral cord = anterior divisions of superior + middle trunks (C5-C7)
- Medial cord = anterior division of inferior trunk (C8-T1)
- Posterior cord = all three posterior divisions (C5-T1)
Terminal Branches
| Nerve | Origin | Motor | Sensory | Injury |
|---|---|---|---|---|
| Musculocutaneous | Lateral cord (C5-C7) | Biceps, brachialis, coracobrachialis | Lateral forearm | Rare; coracobrachialis perforation |
| Median | Lateral + medial cords | Forearm flexors (except FCU + medial FDP), thenar muscles | Lateral 3.5 digits (palm) | Carpal tunnel; "ape thumb" |
| Ulnar | Medial cord (C8-T1) | FCU, medial FDP, hypothenar, interossei | Medial 1.5 digits | Medial epicondyle fracture; claw hand |
| Radial | Posterior cord (C5-T1) | All posterior compartments of arm + forearm | Posterior arm/forearm, dorsal hand | Humeral shaft fracture; wrist drop |
| Axillary | Posterior cord (C5-C6) | Deltoid, teres minor | Lateral shoulder (regimental badge area) | Shoulder dislocation |
Posterior cord mnemonic: STAR (Subscapularis, Thoracodorsal, Axillary, Radial)
Brachial Plexus Injuries - Clinical
| Injury | Roots | Mechanism | Deformity | Eponym |
|---|---|---|---|---|
| Upper trunk | C5-C6 | Shoulder-neck forceful separation (fall, motorcycle) | "Waiter's tip" (adducted, medially rotated, pronated arm) | Erb's palsy |
| Lower trunk | C8-T1 | Arm forceful abduction (birth, cervical rib) | Claw hand + Horner's syndrome | Klumpke's palsy |
| Axillary nerve | C5-C6 | Shoulder dislocation | Cannot abduct arm (deltoid); "regimental badge" sensory loss | - |
| Long thoracic nerve | C5-C6-C7 | Radical neck dissection, stab wound | Winging of scapula | - |
PART 5: LOWER LIMB - LUMBOSACRAL PLEXUS
Formation
- Lumbar plexus: L1, L2, L3, L4 (in psoas major)
- Sacral plexus: L4, L5, S1, S2, S3 (on piriformis)
- Together they form the lumbosacral plexus (L1-S4)
Key branches:
- Femoral nerve (L2-L4) - anterior compartment of thigh; exits under inguinal ligament lateral to artery
- Obturator nerve (L2-L4) - medial compartment (adductors); exits obturator foramen
- Sciatic nerve (L4-S3) - largest nerve in the body; exits greater sciatic foramen below piriformis; splits into tibial + common fibular (peroneal) nerves
- Tibial nerve - posterior leg + sole of foot (plantar flexion, inversion)
- Common fibular (peroneal) nerve - wraps around fibular neck; anterior + lateral leg (dorsiflexion, eversion); very vulnerable to injury here
- Pudendal nerve (S2-S4) - perineum, external anal/urethral sphincters; genitalia
Phrenic nerve (C3, C4, C5) - cervical plexus branch; sole motor supply to diaphragm
Lower Limb Injuries
| Nerve | Common Injury | Clinical Sign |
|---|---|---|
| Femoral | Femoral triangle trauma, pelvic fracture | Cannot extend knee; weak hip flexion; absent knee jerk |
| Obturator | Obturator hernia, pelvic surgery | Weak adduction; medial thigh sensory loss |
| Sciatic | Hip dislocation (posterior), deep IM injection | Combined foot drop + hamstring weakness |
| Common fibular | Fibular neck fracture, prolonged pressure (leg crossing) | Foot drop (cannot dorsiflex/evert); high stepping gait |
| Tibial | Popliteal fossa injury | Cannot plantar flex/invert; clawing of toes |
| Pudendal | Prolonged cycling, obturic surgery | Perineal pain, incontinence, erectile dysfunction |
PART 6: HEAD & NECK NEUROVASCULAR STRUCTURES
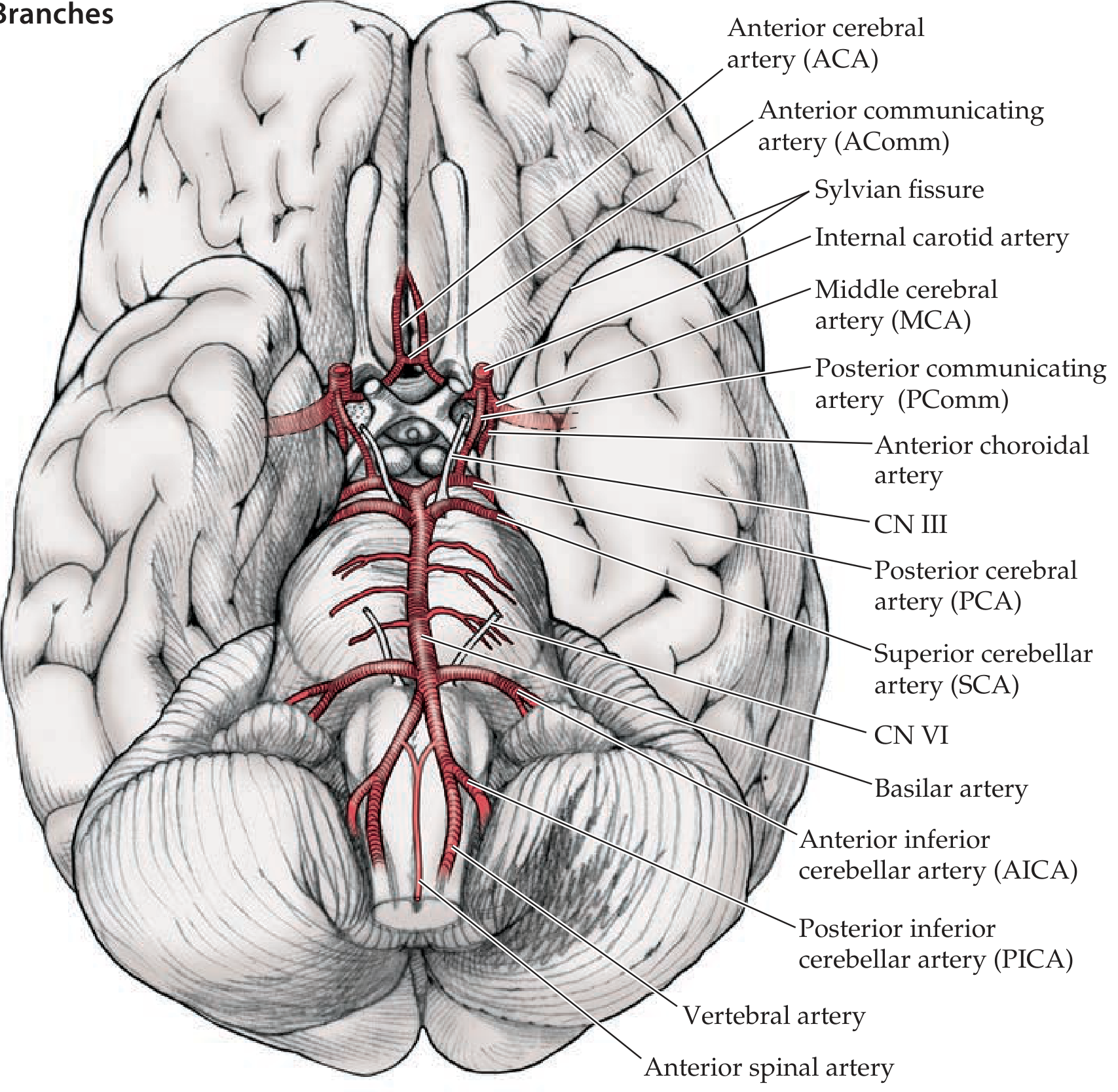
Cranial Nerve-Vessel Relationships
| CN | Artery Adjacent/Companion | Clinical Relevance |
|---|---|---|
| CN II (Optic) | Ophthalmic artery (from ICA) | Ophthalmic artery occlusion -> monocular blindness; ICA aneurysm can compress CN II |
| CN III (Oculomotor) | PComm (adjacent at PComm-ICA junction) | Posterior communicating artery aneurysm -> painful CN III palsy with pupil dilation |
| CN V (Trigeminal) | Superior cerebellar artery (SCA) loops near root | Vascular compression -> Trigeminal neuralgia (tic douloureux) |
| CN VII (Facial) | AICA forms loop near facial nerve in internal acoustic meatus | AICA aneurysm/compression -> facial palsy + deafness |
| CN VIII (Vestibulocochlear) | AICA | AICA occlusion -> lateral pontomedullary syndrome |
Carotid Sheath
Contains (lateral to medial):
- Internal/common carotid artery
- Internal jugular vein
- Vagus nerve (CN X) - lies posteriorly between artery and vein
Subclavian Artery
- Right: branch of brachiocephalic trunk
- Left: direct branch of aortic arch
- Passes between anterior and middle scalene muscles with brachial plexus trunks
- Gives off vertebral artery, thyrocervical trunk, internal thoracic artery, costocervical trunk
- Clinical: Cervical rib can compress the subclavian artery + inferior trunk of brachial plexus (thoracic outlet syndrome)
PART 7: THORAX & ABDOMEN
Intercostal Neurovascular Bundle
- Runs in the costal groove on the inferior border of each rib (from superior to inferior: VAN = Vein, Artery, Nerve)
- Needle procedures (thoracentesis, chest drain) should be placed at the upper border of the rib below to avoid the bundle
Aorta and Its Branches (Clinical)
- Celiac trunk (T12): Liver, stomach, spleen - collateral-rich, rarely infarcted
- Superior mesenteric artery (L1): Whole of small bowel, right colon - SMA occlusion -> massive intestinal infarction
- Inferior mesenteric artery (L3): Left colon, sigmoid, rectum
- Renal arteries (L1-L2): End arteries to kidneys - renal artery stenosis -> renovascular hypertension
Autonomic Supply
- Sympathetic: T1-L2 (thoracolumbar outflow) - "fight or flight"
- Parasympathetic: Cranial (CN III, VII, IX, X) + Sacral (S2-4) - "rest and digest"
- Vagus nerve (CN X) provides parasympathetic supply to heart, lungs, and abdominal viscera down to the splenic flexure
- Pelvic splanchnic nerves (S2-4) supply pelvic viscera
PART 8: CLINICAL CORRELATIONS SUMMARY TABLE
| Condition | Structure Involved | Mechanism | Key Signs |
|---|---|---|---|
| Ischemic stroke (MCA) | MCA territory | Thromboembolism | Contralateral face/arm paresis > leg; aphasia if dominant hemisphere |
| Ischemic stroke (ACA) | ACA territory | Thromboembolism | Contralateral leg paresis > arm; frontal lobe signs |
| PCA stroke | PCA territory | Posterior circulation occlusion | Homonymous hemianopia (cortical blindness) |
| Lacunar infarct | Lenticulostriate arteries / internal capsule | Hypertensive small vessel disease | Pure motor hemiplegia (posterior limb internal capsule) |
| Anterior spinal artery syndrome | Anterior spinal artery | Aortic surgery, hypotension | Bilateral loss of motor function + pain/temperature (spinothalamic); preserved proprioception/vibration |
| Posterior spinal artery occlusion | Posterior spinal arteries | Rare | Loss of proprioception + vibration; motor spared |
| Subarachnoid hemorrhage | Circle of Willis aneurysm (most common: AComm, PComm, MCA bifurcation) | Aneurysm rupture | "Thunderclap" worst headache of life; CN III palsy (PComm) |
| Trigeminal neuralgia | CN V root / SCA | Vascular loop compression | Lancinating facial pain, triggered by touch/chewing |
| Horner's syndrome | Sympathetic chain (T1-T2 root, stellate ganglion) | Pancoast tumor, carotid dissection | Ptosis, miosis, anhidrosis (same side) |
| Thoracic outlet syndrome | Subclavian artery + inferior brachial plexus trunk | Cervical rib / scalene hypertrophy | Klumpke-pattern weakness + vascular compromise in arm |
| Meralgia paresthetica | Lateral femoral cutaneous nerve | Compression at ASIS / inguinal ligament | Burning thigh pain; no motor deficit |
| Foot drop | Common fibular nerve | Fibular neck fracture or prolonged pressure | Cannot dorsiflex foot; high-stepping gait; sensory loss on dorsum of foot |
| Saturday night palsy | Radial nerve in spiral groove | Prolonged arm compression | Wrist drop; intact brachioradialis; spared triceps |
PART 9: HIGH-YIELD EXAM MNEMONICS
| Mnemonic | Meaning |
|---|---|
| Robert Taylor Drinks Cold Beer | Brachial plexus levels: Roots, Trunks, Divisions, Cords, Branches |
| STAR | Posterior cord branches: Subscapularis, Thoracodorsal, Axillary, Radial |
| BBC | Musculocutaneous nerve muscles: Biceps, Brachialis, Coracobrachialis |
| OPAAM | ICA branches: Ophthalmic, Posterior communicating, Anterior choroidal, ACA, MCA |
| VAN | Intercostal bundle order (top to bottom): Vein, Artery, Nerve |
| C3, 4, 5 keeps the diaphragm alive | Phrenic nerve roots |
| S2, 3, 4 keeps the pee off the floor | Pudendal nerve roots (micturition control) |
| "2 above, 4 below" | Intercostal nerve: needle above rib below to avoid neurovascular bundle |
PART 10: VENOUS DRAINAGE - KEY POINTS
Brain:
- Venous drainage by internal jugular veins bilaterally
- Cerebral veins drain into dural venous sinuses (superior sagittal, transverse, sigmoid, cavernous)
- Cavernous sinus: contains ICA, CN III, IV, V1, V2, VI - thrombosis produces painful ophthalmoplegia
Spinal cord: via epidural Batson's plexus (valveless - metastatic spread route)
Limbs: Deep veins accompany arteries; superficial veins (cephalic/basilic in arm; great/small saphenous in leg) drain independently into deep system
Sources: Neuroanatomy through Clinical Cases, 3rd Ed. (Blumenfeld) | Gray's Anatomy for Students | Neuroscience: Exploring the Brain, 5th Ed. | Neuroanatomy through Clinical Cases is cited as the primary reference for vascular territories and plexus schematics throughout.
human anatomy neurovascular structure from basic to clinical
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Here is a fully illustrated, exam-ready guide to Human Anatomy Neurovascular Structures - from basic to clinical - sourced from Neuroanatomy through Clinical Cases 3rd Ed. (Blumenfeld), Gray's Anatomy for Students, and Neuroscience: Exploring the Brain 5th Ed.
Human Anatomy: Neurovascular Structures
Basic to Clinical - Complete Medical School Guide
PART 1 - FOUNDATIONAL CONCEPTS
What Is a Neurovascular Bundle?
A neurovascular bundle is the co-travelling unit of an artery, vein, and nerve within a common fascial sheath. They travel together because they share the same embryological development pathways and connective tissue channels. This has a critical clinical implication: trauma, compression, or tumor at any single point injures all three components simultaneously - nerve function, arterial inflow, and venous outflow are affected together.
Core Principles
- Nerves follow arteries - peripheral nerves track alongside their named companion arteries
- Most peripheral nerves are mixed - carrying motor, sensory, AND autonomic (sympathetic) fibers
- Watershed zones between two arterial territories are the most vulnerable to ischemia when perfusion pressure drops
- Venous drainage often diverges from arterial supply (e.g., cerebral veins vs. arteries)
- Valveless venous plexuses (e.g., Batson's plexus) allow bidirectional flow and act as routes for metastatic spread
PART 2 - BRAIN: ARTERIAL SUPPLY
The Two-Circulation System
The brain is supplied by two paired arterial systems that unite at the base of the brain:
| System | Arteries | Origin |
|---|---|---|
| Anterior circulation | Internal carotid arteries (ICAs) | Common carotid arteries (from aorta / brachiocephalic trunk) |
| Posterior circulation | Vertebral arteries → Basilar artery | Subclavian arteries; vertebrals ascend through foramina transversaria of C1-C6, enter foramen magnum, and join to form the basilar |
The Circle of Willis
The two circulations meet at an anastomotic ring at the base of the brain called the Circle of Willis. This provides collateral flow pathways, but a complete full-caliber ring is present in only ~34% of individuals - anatomical variants are the rule, not the exception.
Composition of the Circle:
- Anterior arch: ACA (left) - AComm - ACA (right)
- Lateral bridges: ICA → PComm → PCA (each side)
- Posterior arch: PCA (left) ← basilar artery → PCA (right)
ICA Course and Segments
The ICA has four segments: cervical → petrous (in carotid canal) → cavernous (S-shaped carotid siphon in cavernous sinus) → supraclinoid (intracranial).
Mnemonic - Supraclinoid ICA branches: OPAAM
- O - Ophthalmic artery (enters optic canal with CN II → retinal supply)
- P - Posterior communicating artery (PComm)
- A - Anterior choroidal artery
- A - Anterior cerebral artery (ACA)
- M - Middle cerebral artery (MCA)
The Three Main Cerebral Arteries and Their Territories
| Artery | Course | Cortex Supplied | Key Structures | Stroke Syndrome |
|---|---|---|---|---|
| ACA | Passes forward into interhemispheric fissure, sweeps over corpus callosum | Medial frontal + anterior parietal | Leg/foot sensorimotor cortex, supplementary motor area | Contralateral leg > arm weakness; frontal lobe signs |
| MCA | Turns lateral into Sylvian fissure; divides into superior + inferior divisions | Dorsolateral convexity | Face + arm motor/sensory, Broca's area (L dominant), Wernicke's area (L dominant) | Contralateral face/arm > leg weakness; aphasia (dominant); neglect (non-dominant) |
| PCA | Arises from top of basilar; curves over inferior temporal lobe | Medial/inferior temporal + occipital | Primary visual cortex, inferior temporal cortex | Homonymous hemianopia; alexia without agraphia (L PCA); visual agnosia |
Deep Perforating Vessels (High-Yield for Exams)
The deep brain structures (basal ganglia, thalamus, internal capsule) are supplied by small penetrating arteries that arise from the proximal segments of the major vessels:
| Vessel | Origin | Territory | Clinical Relevance |
|---|---|---|---|
| Lenticulostriate arteries | MCA (M1 segment) | Basal ganglia, internal capsule (posterior limb) | Rupture in hypertension → intracerebral hemorrhage; occlusion → lacunar infarct → pure motor hemiplegia |
| Anterior choroidal artery | ICA (supraclinoid) | Globus pallidus, putamen, posterior limb internal capsule, lateral geniculate nucleus | Infarct → contralateral hemiparesis + hemisensory loss + homonymous hemianopia (3 Hs) |
| Recurrent artery of Heubner | ACA (A1/A2 junction) | Head of caudate, anterior putamen, anterior internal capsule | Infarct → face + arm > leg weakness |
| Thalamoperforators | Proximal PCA (P1) | Thalamus, midbrain | Infarct → "thalamic syndrome" - hemisensory loss, thalamic pain |
PART 3 - SPINAL CORD: BLOOD SUPPLY
Arterial Supply
| Artery | Number | Source | Cord Territory |
|---|---|---|---|
| Anterior spinal artery | 1 (single, midline) | Vertebral arteries (cervical); reinforced by radicular arteries | Anterior 2/3 of cord: anterior horns (LMNs), corticospinal tract, spinothalamic tract |
| Posterior spinal arteries | 2 (paired) | Vertebral arteries or PICA | Posterior 1/3: posterior columns (proprioception, vibration), part of posterior horns |
| Radicular arteries | 6-10 total | Segmental branches from aorta at variable levels | Reinforce the longitudinal spinal arteries |
Artery of Adamkiewicz (Great Radicular Artery)
- Arises from the left side in ~70-80% of individuals
- Level: T5-L3, most commonly T9-T12
- Provides the major blood supply to the lumbar and sacral cord
- Damage during thoracic aortic surgery or aortic dissection → paraplegia
Vulnerable Watershed Zone
- T4-T8 lies between the vertebral supply above and the aortic supply below
- This mid-thoracic watershed is most susceptible to infarction during:
- Hypotension / cardiac arrest
- Thoracic aortic clamping or aneurysm repair
Anterior Spinal Artery Syndrome (Clinical)
- Cause: Aortic surgery, thromboembolism, aortic dissection, hypotension
- Result: Infarction of anterior 2/3 of cord
- Signs: Bilateral motor loss (corticospinal) + pain/temperature loss (spinothalamic) BELOW the level; posterior columns preserved (proprioception/vibration intact)
- This dissociation distinguishes anterior from posterior cord injury
Batson's Venous Plexus
- Epidural valveless venous network draining the spinal cord
- No valves → elevated intra-abdominal/intrathoracic pressure reverses flow
- Route for metastatic spread of prostate, breast, lung, and pelvic cancers to the spine
- Also pathway for spread of pelvic infections to epidural space
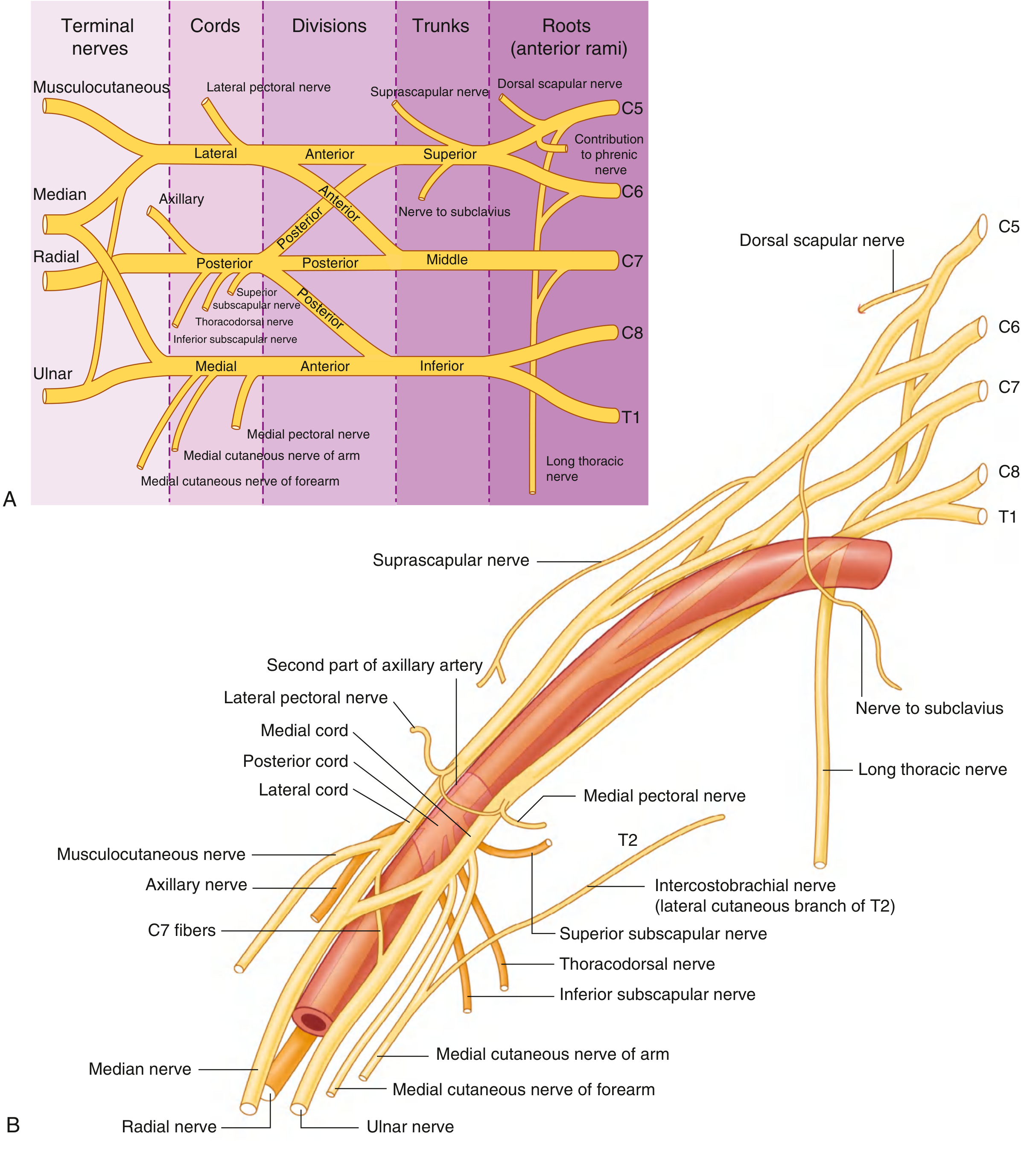
PART 4 - UPPER LIMB: BRACHIAL PLEXUS
Formation
Mnemonic: "Robert Taylor Drinks Cold Beer" = Roots, Trunks, Divisions, Cords, Branches
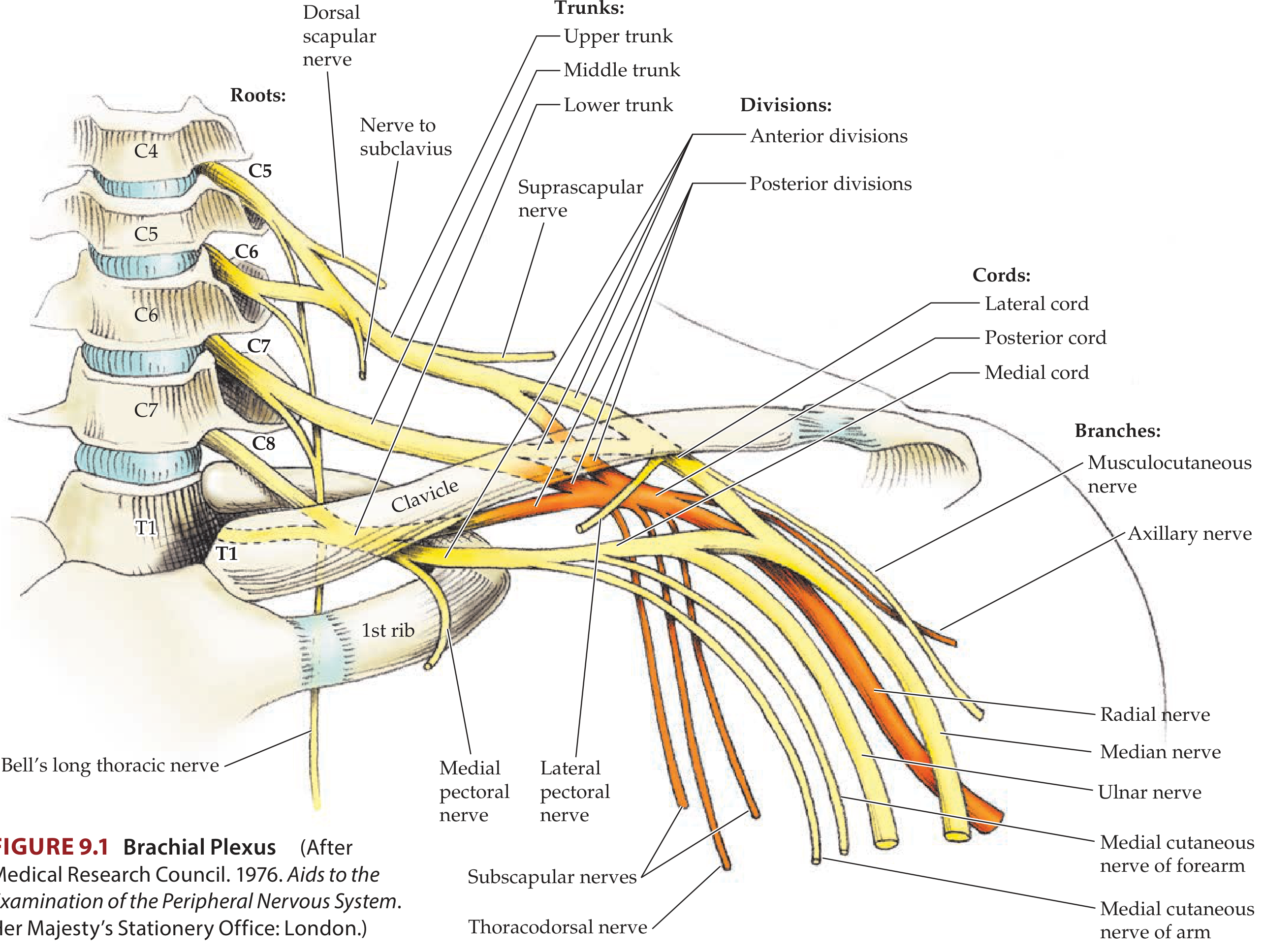
Roots (C5, C6, C7, C8, T1 - anterior rami):
- Pass between anterior and middle scalene muscles
- Receive gray rami communicantes from the sympathetic trunk (postganglionic sympathetic fibers to periphery)
- Lie posterior to the subclavian artery in the posterior triangle of the neck
Trunks (pass over 1st rib into axilla):
- Superior = C5 + C6
- Middle = C7 alone
- Inferior = C8 + T1 (lies on 1st rib, posterior to subclavian artery)
Divisions (each trunk → anterior + posterior):
- No peripheral nerves arise directly from divisions
- Anterior divisions → supply flexor/anterior compartments
- Posterior divisions → supply extensor/posterior compartments
Cords (named by position relative to 2nd part of axillary artery):
- Lateral cord = anterior divisions of superior + middle trunks (C5-C7)
- Medial cord = anterior division of inferior trunk (C8-T1)
- Posterior cord = all three posterior divisions (C5-T1)
Posterior cord mnemonic: STAR (Subscapularis, Thoracodorsal, Axillary, Radial) or ARTS
Terminal Branches - The Five Clinically Critical Nerves
| Nerve | Origin | Roots | Motor | Sensory | Injury Site | Classic Deformity |
|---|---|---|---|---|---|---|
| Radial | Posterior cord | C5-T1 | Extension of elbow, wrist, fingers; supination; thumb abduction | Posterior arm/forearm; dorsal hand (lateral) | Humeral shaft fracture (spiral groove) | Wrist drop |
| Median | Lateral + medial cords | C6-T1 | Thumb flexion/opposition; flexion digits 2-3; wrist flexion/abduction; pronation | Lateral 3.5 digits (palmar); thenar | Carpal tunnel; supracondylar fracture | "Ape thumb" (thenar wasting + loss of opposition) |
| Ulnar | Medial cord | C8-T1 | Finger adduction/abduction; thumb adduction; flexion digits 4-5; wrist adduction | Medial 1.5 digits | Medial epicondyle fracture; cubital tunnel | Claw hand (4th/5th digits) |
| Axillary | Posterior cord | C5-C6 | Deltoid (abduction); teres minor (lateral rotation) | Lateral shoulder ("regimental badge" area) | Shoulder dislocation; neck of humerus fracture | Cannot abduct arm |
| Musculocutaneous | Lateral cord | C5-C7 | Biceps, brachialis, coracobrachialis (BBC) | Lateral forearm | Rare; coracobrachialis penetration | Weak elbow flexion |
Brachial Plexus Injuries - Exam Favorites
| Injury | Roots | Mechanism | Deformity | Eponym |
|---|---|---|---|---|
| Upper trunk | C5-C6 | Shoulder-neck forced separation (motorcycle fall, difficult delivery) | "Waiter's tip": arm adducted, medially rotated, pronated, wrist flexed | Erb-Duchenne palsy |
| Lower trunk | C8-T1 | Forced arm abduction (birth - arm over head; cervical rib; Pancoast tumor) | Claw hand + Horner's syndrome (ptosis, miosis, anhidrosis - sympathetic chain affected at T1) | Klumpke's palsy |
| Long thoracic nerve (C5-C6-C7) | C5-C7 | Radical neck dissection; stab wound; carrying heavy loads | Winging of scapula (serratus anterior paralysis) | - |
| Axillary nerve | C5-C6 | Shoulder dislocation | Cannot abduct beyond 15°; sensory loss regimental badge area | - |
PART 5 - LOWER LIMB: LUMBOSACRAL PLEXUS
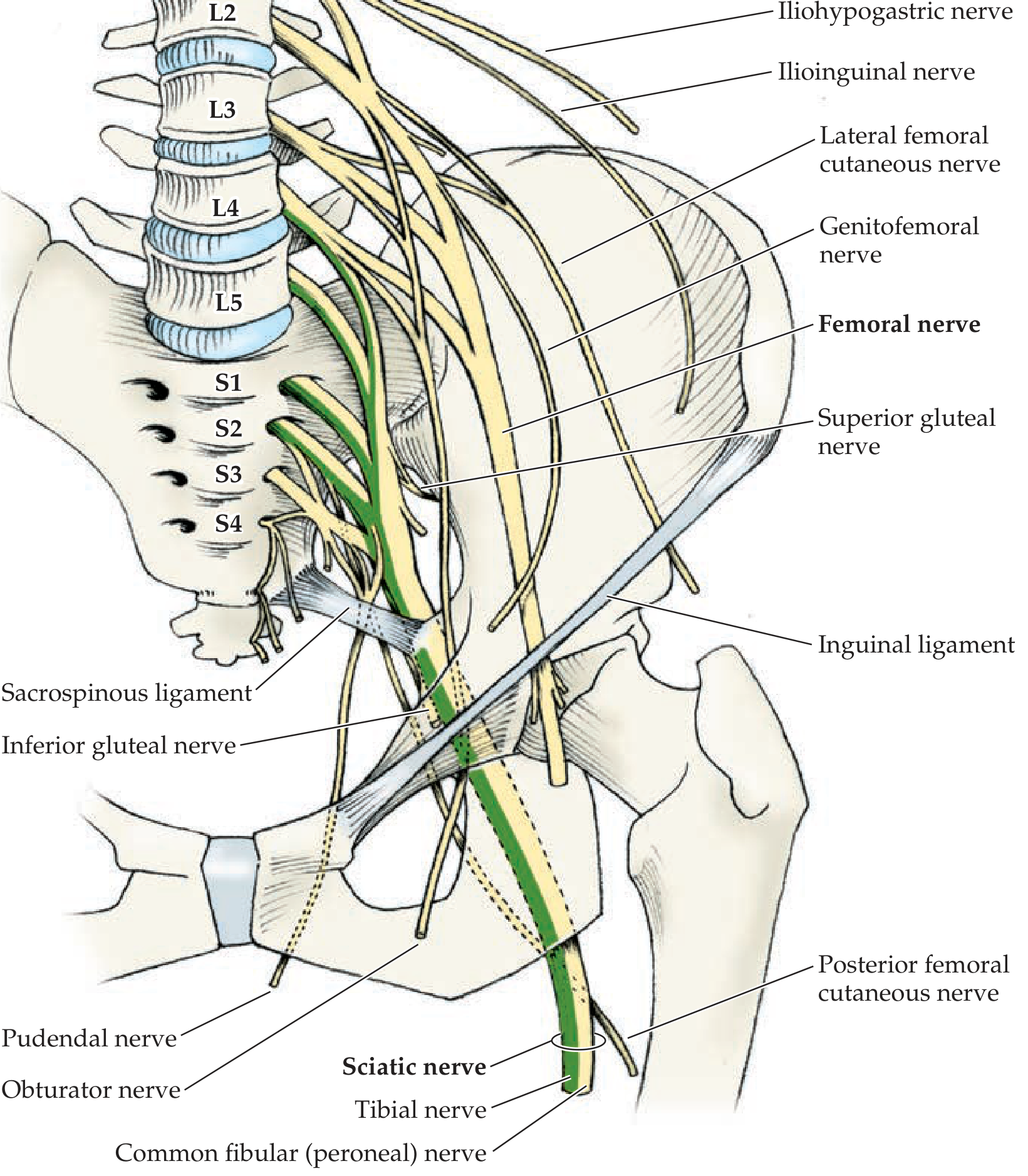
Formation
| Division | Roots | Location of Formation |
|---|---|---|
| Lumbar plexus | L1-L4 | Within psoas major muscle |
| Sacral plexus | L4-S3 | On piriformis muscle, posterior pelvis |
| Pudendal nerve | S2-S4 | Below sacrospinous ligament |
Five Key Nerves to Know
| Nerve | Roots | Exit Route | Motor | Sensory | Common Injury | Sign |
|---|---|---|---|---|---|---|
| Femoral | L2-L4 | Under inguinal ligament (lateral to femoral artery - NAVEL order: Nerve, Artery, Vein, Empty space, Lymphatics) | Quadriceps (knee extension); iliopsoas (hip flexion) | Anterior/medial thigh; medial leg (saphenous nerve) | Femoral triangle trauma; pelvic fracture; hematoma | Cannot extend knee; absent knee jerk (L3-L4) |
| Obturator | L2-L4 | Through obturator foramen | Adductors of thigh | Medial thigh | Obturator hernia; pelvic surgery | Weak thigh adduction |
| Sciatic | L4-S3 | Below piriformis through greater sciatic foramen | Hamstrings (hip extension, knee flexion); all muscles below knee via tibial + common fibular | Posterior thigh; all below knee | Posterior hip dislocation; deep IM injection (avoid upper medial quadrant!) | Combined foot drop + hamstring weakness |
| Common fibular (peroneal) | L4-S2 | Winds around head/neck of fibula | Dorsiflexion (deep branch); eversion (superficial branch) | Dorsum of foot; lateral leg | Fibular neck fracture; leg cast; leg crossing; prolonged squatting | Foot drop (cannot dorsiflex); high-stepping gait; sensory loss dorsum foot |
| Tibial | L4-S3 | Popliteal fossa → posterior leg | Plantar flexion (gastrocnemius, soleus); toe flexion; foot inversion; intrinsic foot muscles | Sole of foot | Popliteal fossa injuries; posterior compartment syndrome | Cannot plantar flex/invert; clawing of toes |
Pudendal nerve (S2-S4): Mnemonic: "S2, 3, 4 keeps the pee off the floor" - supplies perineum, external urethral and anal sphincters, erectile tissue. Injury in prolonged cycling, childbirth, or perineal surgery → perineal pain, urinary/fecal incontinence, erectile dysfunction.
Other notable nerves:
- Lateral femoral cutaneous nerve (L2-L3): pure sensory; compressed at ASIS under inguinal ligament → meralgia paresthetica (burning/numbness lateral thigh, no motor deficit)
- Superior gluteal nerve (L4-L5-S1): gluteus medius/minimus + tensor fascia lata; injury → Trendelenburg gait (pelvis drops on opposite side when standing on affected leg)
PART 6 - HEAD AND NECK NEUROVASCULAR STRUCTURES
Key Neurovascular Relationships
| CN/Structure | Adjacent Vessel | Clinical Correlation |
|---|---|---|
| CN II (Optic) | Ophthalmic artery (from ICA) | Ophthalmic artery occlusion → amaurosis fugax (transient monocular blindness); herald of carotid disease |
| CN III (Oculomotor) | PComm artery passes adjacent | PComm aneurysm → painful CN III palsy with pupil dilation (surgical third nerve palsy) |
| CN V (Trigeminal) | Superior cerebellar artery (SCA) loops near trigeminal root | Vascular compression → trigeminal neuralgia (tic douloureux): lancinating face pain triggered by touch/eating |
| CN VII (Facial) | AICA forms a loop near facial nerve in internal acoustic meatus | AICA aneurysm/compression → ipsilateral facial palsy + deafness |
| CN IX, X, XI | Internal jugular vein | Jugular foramen syndrome (Vernet's): mass at jugular foramen compresses all three simultaneously |
Carotid Sheath Contents (mnemonic: I Am Very Nervous = ICA/CCA, Artery, Vein, Nerve)
- Internal/Common Carotid artery (medial)
- Vagus nerve (CN X): lies posteriorly between artery and vein
- Internal Jugular vein (lateral)
The vagus nerve is at risk during carotid endarterectomy, central line placement in the internal jugular, and radical neck dissection.
Cavernous Sinus (Neurovascular Crossroads)
The cavernous sinus contains some of the most densely packed neurovascular structures in the body:
- ICA (passes through its center - cavernous segment)
- CN III, IV, V1, V2 (in the lateral wall)
- CN VI (within the sinus lumen - most vulnerable to raised ICP)
Cavernous sinus thrombosis: painful ophthalmoplegia + proptosis + chemosis; CN VI palsy is often the first sign (lateral gaze palsy = diplopia on looking laterally).
Subclavian Artery and Thoracic Outlet
The subclavian artery + brachial plexus roots pass together between the anterior and middle scalene muscles (the scalene triangle). A cervical rib or scalene hypertrophy can compress both, producing:
- Klumpke-pattern neurological deficit (C8-T1: small hand muscles, claw hand)
- Subclavian artery compression: reduced pulse, Raynaud's phenomenon, digital ischemia
- Horner's syndrome (T1 sympathetic fibers compressed)
- This combination = Thoracic Outlet Syndrome
PART 7 - THORAX AND BODY WALL
Intercostal Neurovascular Bundle
The intercostal vessels and nerve run together in the costal groove on the inferior border of each rib, in the order (from superior to inferior):
Mnemonic: VAN = Vein, Artery, Nerve
Clinical: For thoracentesis, chest drain (intercostal drain), or rib block, always insert the needle at the upper border of the lower rib to avoid the neurovascular bundle. Damage causes:
- Hemorrhage (intercostal artery laceration - can be life-threatening)
- Pneumothorax
- Intercostal neuralgia
Aorta and Visceral Branches
| Branch | Level | Territory | Clinical Importance |
|---|---|---|---|
| Celiac trunk | T12 | Liver, stomach, spleen, pancreas (head) | Rich collaterals; rarely causes bowel ischemia alone |
| Superior mesenteric artery (SMA) | L1 | Entire small bowel + right colon | SMA occlusion → acute mesenteric ischemia (surgical emergency); "food fear" in chronic stenosis |
| Inferior mesenteric artery (IMA) | L3 | Left colon, sigmoid, rectum | IMA territory most vulnerable during aortic surgery; watershed at splenic flexure |
| Renal arteries | L1-L2 | Kidneys (end arteries) | Renal artery stenosis → renovascular hypertension + ischemic nephropathy |
PART 8 - AUTONOMIC NEUROVASCULAR SYSTEM
| Division | Origin | Outflow | Transmitter | Effect |
|---|---|---|---|---|
| Sympathetic | T1-L2 (thoracolumbar) | Via sympathetic chain → gray rami → peripheral nerves | Noradrenaline (periphery) | Vasconstriction, tachycardia, pupil dilation, sweating |
| Parasympathetic | CN III, VII, IX, X + S2-S4 (craniosacral) | Via cranial nerves or pelvic splanchnics | Acetylcholine | Vasodilation, bradycardia, pupil constriction, secretion |
Vagus nerve (CN X): Parasympathetic supply to heart, lungs, esophagus, stomach, small bowel, and large bowel to splenic flexure. Pelvic splanchnic nerves (S2-S4) take over from the splenic flexure distally.
Horner's Syndrome (lesion of sympathetic pathway at any level):
- Ptosis (superior tarsal muscle paralysis)
- Miosis (pupil constriction)
- Anhidrosis (ipsilateral face)
- Enophthalmos (apparent)
- Causes by level: Hypothalamus/brainstem (1st order) → Pancoast tumor/cervical rib/thyroid (2nd order, T1) → Carotid dissection/cavernous sinus (3rd order)
PART 9 - VENOUS DRAINAGE (KEY STRUCTURES)
| Region | Drainage Pathway | Clinical Point |
|---|---|---|
| Brain cortex | Cerebral veins → dural sinuses (superior sagittal, transverse, sigmoid) → internal jugular veins | Dural sinus thrombosis: headache, papilledema, seizures |
| Cavernous sinus | Receives ophthalmic veins; drains to sigmoid sinus / IJV | Danger triangle of face (nasolabial fold): facial vein drains retrogradely to cavernous sinus - facial infections can cause cavernous sinus thrombosis |
| Spinal cord | Anterior/posterior spinal veins → epidural Batson's plexus | Valveless; metastatic route for prostate, breast, and pelvic cancers |
| Upper limb | Deep veins follow arteries; superficial: cephalic (lateral), basilic (medial) → axillary vein | Basilic vein used for PICC line insertion; cephalic for IV access |
| Lower limb | Deep veins follow arteries; superficial: great saphenous (medial) and small saphenous (posterior) | Great saphenous used for bypass grafts; CABG and peripheral vascular surgery |
PART 10 - CLINICAL CORRELATIONS MASTER TABLE
| Condition | Neurovascular Structure | Mechanism | Key Clinical Signs |
|---|---|---|---|
| MCA stroke | Middle cerebral artery | Thromboembolism | Contralateral face/arm > leg paresis + sensory loss; aphasia (dominant); neglect (non-dominant) |
| ACA stroke | Anterior cerebral artery | Thromboembolism | Contralateral leg > arm paresis; frontal disinhibition; urinary incontinence |
| PCA stroke | Posterior cerebral artery | Thromboembolism | Contralateral homonymous hemianopia; +/- thalamic pain; alexia without agraphia (L) |
| Lacunar infarct | Lenticulostriate / internal capsule perforators | Hypertensive small-vessel disease | Pure motor hemiplegia; pure hemisensory loss; ataxic hemiparesis - no cortical signs |
| PComm aneurysm | Posterior communicating artery | Berry aneurysm rupture | Sudden severe headache ("thunderclap") + CN III palsy with dilated pupil |
| Anterior spinal artery syndrome | Anterior spinal artery | Aortic surgery, hypotension | Bilateral motor loss + spinothalamic loss below level; posterior columns (proprioception/vibration) preserved |
| Adamkiewicz injury | Artery of Adamkiewicz (T9-T12) | Thoracic aortic surgery | Paraplegia |
| Erb's palsy | C5-C6 brachial plexus (upper trunk) | Shoulder-neck stretch | "Waiter's tip": adducted arm, medially rotated, pronated |
| Klumpke's palsy | C8-T1 brachial plexus (lower trunk) | Cervical rib, Pancoast tumor | Claw hand + Horner's syndrome |
| Wrist drop | Radial nerve (spiral groove) | Humeral shaft fracture / "Saturday night palsy" | Cannot extend wrist/fingers; brachioradialis intact; triceps intact |
| Carpal tunnel | Median nerve (wrist) | Flexor retinaculum compression | Thenar wasting; loss of opposition; Tinel's + Phalen's signs |
| Claw hand | Ulnar nerve (medial epicondyle) | Medial epicondyle fracture | Ring and little finger clawed; Froment's sign |
| Foot drop | Common fibular nerve (fibular neck) | Fibular neck fracture; prolonged leg crossing | Cannot dorsiflex or evert foot; high-stepping gait; sensory loss dorsum of foot |
| Trendelenburg gait | Superior gluteal nerve | Hip surgery, pelvic fracture | Pelvis drops to opposite side when standing on affected leg |
| Meralgia paresthetica | Lateral femoral cutaneous nerve | Compression at ASIS / inguinal ligament | Burning/numbness lateral thigh; NO motor deficit |
| Horner's syndrome | Sympathetic pathway (T1) | Pancoast tumor, carotid dissection | Ptosis + miosis + anhidrosis (ipsilateral) |
| Thoracic outlet syndrome | Subclavian artery + inferior brachial plexus | Cervical rib, scalene hypertrophy | Klumpke-pattern hand weakness + vascular signs in arm + Horner's |
| Cavernous sinus thrombosis | Cavernous sinus + CN III, IV, V1, V2, VI | Facial/dental infection; sinus thrombosis | Painful ophthalmoplegia + proptosis; CN VI palsy often first sign |
| Trigeminal neuralgia | CN V + SCA | Vascular loop compression at trigeminal root | Lancinating unilateral face pain; triggered by touch/chewing; no sensory loss between attacks |
PART 11 - HIGH-YIELD MNEMONICS SUMMARY
| Mnemonic | Meaning |
|---|---|
| Robert Taylor Drinks Cold Beer | Brachial plexus: Roots, Trunks, Divisions, Cords, Branches |
| STAR / ARTS | Posterior cord branches: Subscapularis, Thoracodorsal, Axillary, Radial |
| BBC | Musculocutaneous nerve muscles: Biceps, Brachialis, Coracobrachialis |
| OPAAM | Supraclinoid ICA branches: Ophthalmic, PComm, Anterior choroidal, ACA, MCA |
| VAN | Intercostal order (top to bottom): Vein, Artery, Nerve |
| NAVEL | Femoral triangle (lateral to medial): Nerve, Artery, Vein, Empty, Lymphatics |
| C3, C4, C5 keeps the diaphragm alive | Phrenic nerve roots |
| S2, S3, S4 keeps the pee off the floor | Pudendal nerve roots (micturition control) |
| "Upper border of lower rib" | Where to place thoracentesis needle (avoids VAN bundle) |
| "Danger triangle of the face" | Nasolabial fold area - facial infections can spread retrogradely to cavernous sinus |
Sources: Neuroanatomy through Clinical Cases, 3rd Ed. (Blumenfeld) | Gray's Anatomy for Students (Drake et al.) | Neuroscience: Exploring the Brain, 5th Ed. (Bear, Connors, Paradiso)
This is a shared conversation. Sign in to Orris to start your own chat.