DOC for post menopausal breast cancer?
Reading File
Finding Sources
Searching PubMed
"breast cancer" AND "aromatase inhibitor" AND postmenopausal
Reading File
Reading File
Here is a complete, textbook-backed answer:
DOC for Post-Menopausal Breast Cancer
Hormone Receptor-Positive (ER+/PR+) - The Most Common Scenario
Drug of Choice: Aromatase Inhibitors (AIs)
After menopause, the ovaries stop producing estrogen. The main estrogen source shifts to peripheral conversion of adrenal androgens to estrogen via the enzyme CYP19 (aromatase) in adipose and mammary tissue. AIs block this conversion, causing profound estrogen deprivation in post-menopausal women.
Three approved third-generation AIs:
| Drug | Type | Dose |
|---|---|---|
| Anastrozole | Non-steroidal (reversible) | 1 mg/day |
| Letrozole | Non-steroidal (reversible) | 2.5 mg/day |
| Exemestane | Steroidal (irreversible) | 25 mg/day |
All three have similar efficacy and a similar side-effect spectrum - the choice is often based on tolerability.
Why AIs Over Tamoxifen in Post-Menopausal Women?
- AIs reduce recurrence rates by ~30% more (proportionately) compared to tamoxifen in post-menopausal ER+ breast cancer
- The EBCTCG meta-analysis of 31,920 post-menopausal women confirms AIs outperform tamoxifen for early breast cancer
- Tamoxifen carries risks of thromboembolic events and endometrial cancer (due to estrogen agonist effects) - these are avoided with AIs
- Adjuvant AI use in post-menopausal women has progressively limited tamoxifen to the premenopausal setting
Tamoxifen remains preferred in premenopausal women and men with breast cancer. AIs should NOT be used as monotherapy in premenopausal women (the ovaries would simply produce more estrogen in compensation).
Duration
- Standard: 5 years of adjuvant AI therapy
- Extended (10 years): Benefit beyond 5 years remains debated. A 2025 EBCTCG Lancet meta-analysis (PMID 40783288) analyzed 12 trials of extended AI use beyond 5 years of endocrine therapy in 22,031 post-menopausal women - the greatest benefit of longer therapy is prevention of contralateral breast cancer
Side Effects of AIs
- Postmenopausal symptoms (hot flashes, vaginal dryness)
- Osteoporosis and fractures (major concern - estrogen deprivation)
- Arthralgias / myalgias
- No increased risk of thromboembolic events or endometrial cancer (unlike tamoxifen)
Additional Combinations (High-Risk Disease)
- AI + CDK4/6 inhibitor (abemaciclib, ribociclib, palbociclib): Improves outcomes in high-risk early or advanced ER+ breast cancer
- AI + Everolimus (mTOR inhibitor): Improves progression-free survival in advanced disease previously treated with nonsteroidal AIs
- AI + LHRH agonist: For premenopausal women (not post-menopausal)
HER2-Positive or Triple-Negative Post-Menopausal Breast Cancer
- HER2+: Trastuzumab (anti-HER2 antibody) + chemotherapy; endocrine therapy added if also ER+
- Triple-negative (ER-/PR-/HER2-): AIs are not useful for receptor-negative cancer; chemotherapy is the mainstay
Summary: For the typical post-menopausal breast cancer scenario (HR+/HER2-), the DOC is an aromatase inhibitor (anastrozole, letrozole, or exemestane) for 5 years, preferred over tamoxifen due to greater efficacy and a safer side-effect profile in this population.
Sources: Goldman-Cecil Medicine (2023), Schwartz's Principles of Surgery 11th Ed., Harrison's Principles of Internal Medicine 22E (2025)
SIADH ?
Finding Sources
Searching PubMed
"SIADH" AND "hyponatremia" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a complete breakdown of SIADH:
SIADH - Syndrome of Inappropriate Antidiuretic Hormone Secretion
Definition & Pathophysiology
SIADH occurs when ADH (vasopressin) is secreted despite normal or low plasma osmolality and normal/expanded ECF volume - situations where ADH should normally be suppressed. This drives excess water reabsorption in the collecting ducts, causing:
- Dilutional (euvolemic) hyponatremia
- Expansion of total body water distributed across ECF and ICF (e.g., an extra 3 L splits ~1 L into ECF, 2 L into ICF)
- Subtle volume expansion triggers urinary sodium loss, keeping the patient clinically euvolemic despite water excess
- Decreased plasma protein concentration (dilutional); hematocrit unchanged (opposing effects of dilution vs. red cell swelling)
Causes (Mnemonic: MUDPILES-like - Neuro, Pulm, Drugs, Cancer, Post-op)
| Category | Examples |
|---|---|
| Neurologic (9-26%) | Subarachnoid hemorrhage, stroke, meningitis, tumors, head trauma |
| Intrathoracic (11-19%) | Pneumonia, TB, acute respiratory failure, positive-pressure ventilation |
| Malignancy (18-25%) | Small cell carcinoma of lung (most common), pancreatic cancer, lymphoma |
| Postoperative (7-11%) | Common cause, especially after major surgery |
| Drugs (8-18%) | Carbamazepine (20-30% of patients), oxcarbazepine, SSRIs, TCAs, antipsychotics, chlorpropamide, vincristine, cyclophosphamide, NSAIDs, opioids, DDAVP, nicotine, clofibrate |
| AIDS | PCP, CNS infections, HIV-related adrenal insufficiency |
| Miscellaneous | Temporal arteritis, hypothyroidism, idiopathic |
Most important drug causes to remember: Carbamazepine, SSRIs, chlorpropamide, vincristine, cyclophosphamide, DDAVP
Diagnostic Criteria (All must be met)
- Serum osmolality < 275 mOsm/L (hypoosmolality)
- Calculated as: Effective Osm = (2 × Na⁺) + (Glucose/18)
- Urine osmolality > 100 mOsm/L (usually > 300 mOsm/L) - inappropriately concentrated
- Urine sodium > 30 mEq/L (euvolemia = no sodium-retaining stimulus)
- Caveat: 13-42% of patients with low dietary sodium intake may have low urine Na - use FENa cautiously
- Clinical euvolemia (no edema, no dehydration)
- Not on diuretics
- Other causes excluded: hypothyroidism, psychogenic polydipsia, secondary adrenal insufficiency
- Secondary adrenal insufficiency mimics SIADH and is diagnosed in 3-4% of suspected SIADH - always exclude it (only 33-41% of patients are appropriately screened for it)
A Variant: Reset Osmostat
- ADH control resets to maintain Na at a lower set-point (Na 125-135 mEq/L)
- Hyponatremia is stable, not progressive
- Patient retains ability to dilute urine with water load (urine osm can drop to < 100 mOsm/L)
- Treatment: address underlying cause only
Treatment
Step 1: Treat the underlying cause
- Stop offending drugs
- CT chest + head to look for cancer/infection
- SIADH often resolves when the trigger is treated
- Recurrent SIADH in cancer patients suggests cancer recurrence
Step 2: Symptomatic/Specific Management
| Severity | Treatment |
|---|---|
| Mild/Asymptomatic | Fluid restriction < 800 mL/day (may fail if urine Osm > 500 mOsm/L) |
| Moderate | Salt tablets ± furosemide (furosemide reduces medullary solute gradient, facilitating water excretion) |
| Severe (confusion, lethargy) | 3% hypertonic saline with close monitoring |
| Critical (seizures, coma) | 3% hypertonic saline (emergency); rapid partial correction of ~1-2 mEq/L/hr initially |
| Chronic refractory | Vaptans (tolvaptan, conivaptan) - V2 receptor antagonists ("aquaretics"); or demeclocycline (rarely used due to nephrotoxicity/photosensitivity) |
Critical Warning - Osmotic Demyelination Syndrome (ODS)
- Do NOT correct sodium faster than 8-10 mEq/L/24 hours (or 18 mEq/L/48 hours)
- Rapid overcorrection causes ODS (central pontine myelinolysis) - irreversible
- Frequent sodium monitoring is essential
- Normal saline alone can WORSEN hyponatremia in SIADH - ADH retains water while sodium is excreted; don't give isotonic saline without furosemide
Recent Evidence
A 2025 systematic review and meta-analysis (PMID 39362395) in American Journal of Kidney Disease found that oral urea is an effective and inexpensive option for treating SIADH-related hyponatremia, with a favorable safety profile compared to vaptans - gaining increased attention as an alternative, especially where tolvaptan cost is prohibitive.
Quick Summary Table
| Feature | SIADH |
|---|---|
| Volume status | Euvolemic |
| Serum Na | Low (< 135 mEq/L) |
| Serum Osm | Low (< 275 mOsm/L) |
| Urine Osm | High (> 100, usually > 300 mOsm/L) |
| Urine Na | High (> 30 mEq/L) |
| BUN/Creatinine | Normal or low (dilutional) |
| Uric acid | Low (hypouricemia - useful clue) |
Sources: Symptom to Diagnosis 4th Ed., Costanzo Physiology 7th Ed., Henry's Clinical Diagnosis & Lab Methods
Diabetes insipidus ?
Finding Sources
Searching PubMed
"diabetes insipidus" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Here is a complete guide to Diabetes Insipidus:
Diabetes Insipidus (DI)
Definition
DI is the excretion of large volumes of hypotonic, insipid (tasteless) urine - typically > 50 mL/kg/day (> 3-4 L/day) - due to a defect in ADH (vasopressin) action. Key features: polyuria + polydipsia, with normal or elevated serum osmolality.
- Prevalence: ~1:25,000 (rare)
Classification & Pathophysiology
1. Central DI (Neurogenic DI)
- Cause: Failure of hypothalamus/posterior pituitary to synthesize or secrete vasopressin
- As few as 10-15% of normal vasopressinergic neurons is sufficient to maintain normal urine volume - loss of just a few more triggers symptomatic polyuria
- Plasma vasopressin: unmeasurably low or inappropriately low for plasma osmolality
Causes of Central DI:
| Category | Examples |
|---|---|
| Tumors | Craniopharyngioma (most common benign), germinoma, pinealoma, pituitary adenoma with suprasellar extension, metastases (lung, breast, melanoma) |
| Trauma | Head injury, deceleration injury (shearing of pituitary stalk), basilar skull fracture, neurosurgical resection |
| Granulomatous | Sarcoidosis, Langerhans cell histiocytosis, TB |
| Autoimmune | Lymphocytic infundibuloneurohypophysis (postpartum female; thickened stalk + absent bright spot on MRI) |
| Infiltrative | Leukemia, lymphoma |
| Idiopathic | ~50% (presumed autoimmune); do NOT label idiopathic until 4 years of follow-up with annual MRI |
| Hereditary | Autosomal dominant; defect in signal peptide or neurophysin of pre-prohormone; onset in childhood |
MRI finding: Absence of the normal T1 "bright spot" in the posterior pituitary (normally reflects stored vasopressin/oxytocin granules) + pituitary stalk thickening
2. Nephrogenic DI
- Cause: Renal resistance to vasopressin - ADH levels are normal or elevated, but the kidney doesn't respond
- Defects in: V2 receptor (X-linked, 90% of congenital nephrogenic DI) or Aquaporin-2 water channels
Causes of Nephrogenic DI:
| Category | Examples |
|---|---|
| Drugs | Lithium (most common acquired cause), demeclocycline, amphotericin B, foscarnet |
| Metabolic | Hypercalcemia, hypokalemia |
| Renal disease | Sickle cell nephropathy, pyelonephritis, multiple myeloma, analgesic nephropathy, sarcoidosis |
| Congenital | X-linked (V2 receptor mutation) - 4-8 per million male births |
3. Primary Polydipsia (Dipsogenic / Psychogenic)
- Excessive water intake (not a true DI) - but chronic polydipsia washes out the medullary concentrating gradient, causing partial inability to concentrate urine
- Low plasma osmolality and serum Na (key difference from true DI)
- Dipsogenic DI: reset thirst threshold below ADH secretion threshold
- Psychogenic polydipsia: compulsive drinking in psychiatric illness
4. Osmoreceptor Dysfunction (Variant of Central DI)
- Damaged hypothalamic osmoreceptors fail to trigger ADH despite hyperosmolality
- Can also occur in reverse: persistent ADH despite low osmolality
5. Gestational DI
- Excess placental vasopressinase degrades ADH during pregnancy
- A 2025 systematic review (PMID 40440645) characterizes this as a rare but important pregnancy complication
- Responds to desmopressin (which resists vasopressinase)
Clinical Features
- Polyuria: massive (up to 20 L/day in severe DI)
- Polydipsia: secondary to hyperosmolality stimulating thirst
- If thirst mechanism is intact: patient compensates by drinking; serum Na stays normal
- If thirst mechanism is impaired (e.g., hypothalamic damage): severe hypernatremia and hyperosmolality - can cause irreversible brain damage
- Childhood onset: massive dilatation of renal pelvis, ureters, and bladder
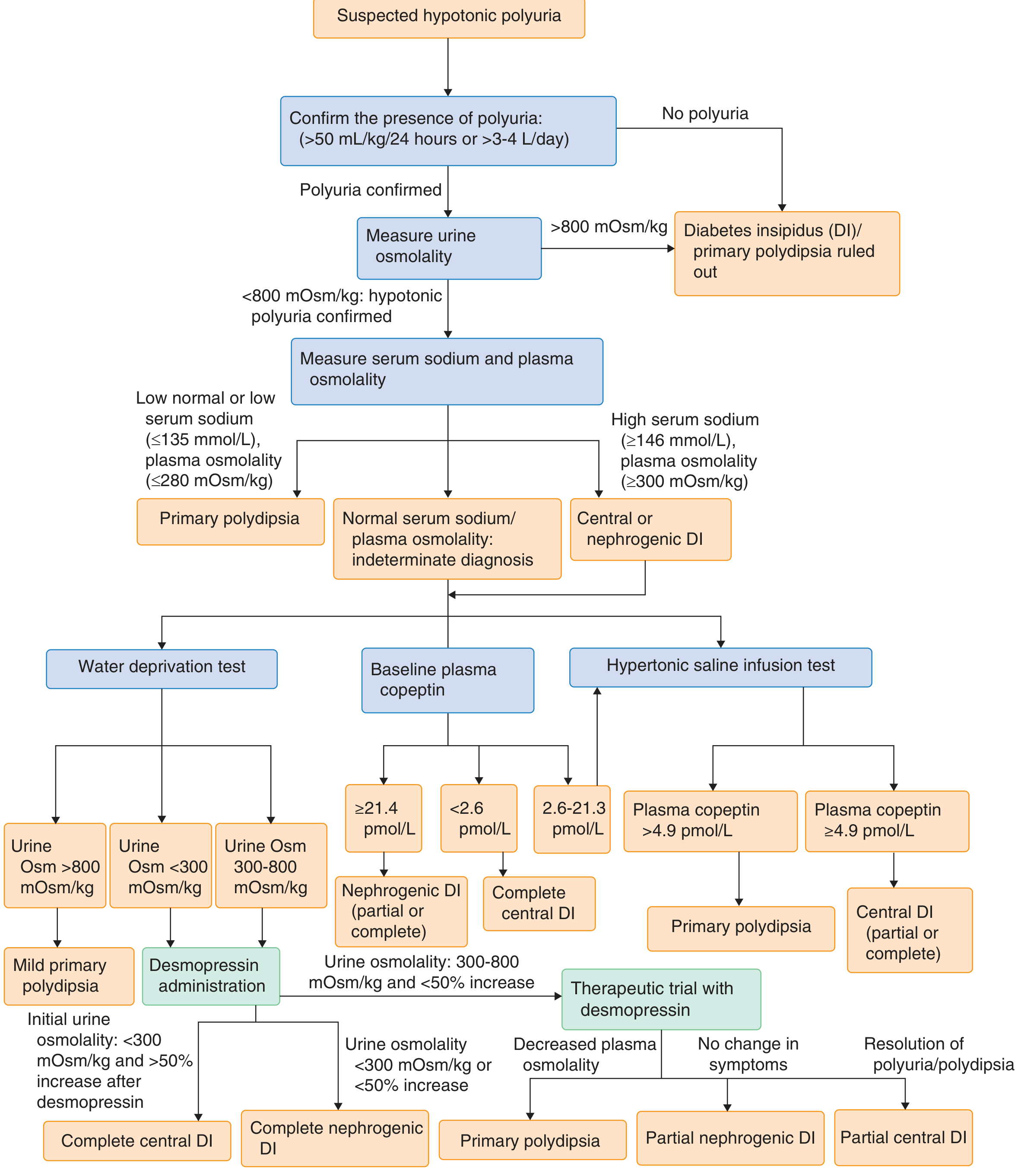
Diagnosis
Step 1: Confirm polyuria
- Urine output > 50 mL/kg/day or > 3-4 L/day
Step 2: Measure urine osmolality
- Urine Osm > 800 mOsm/kg → DI ruled out (urine is concentrated)
- Urine Osm < 800 mOsm/kg → hypotonic polyuria confirmed → proceed
Step 3: Measure serum Na and plasma osmolality
- Low serum Na + low plasma Osm (Na ≤135, Posm ≤280) → Primary polydipsia likely
- High serum Na + high plasma Osm (Na ≥146, Posm ≥300) → Central or Nephrogenic DI
Step 4: Plasma Copeptin (modern approach - replacing older water deprivation test)
Copeptin is the C-terminal segment of pre-pro-AVP, secreted in equimolar amounts with AVP - more stable and easier to measure:
| Copeptin Level | Interpretation |
|---|---|
| ≥ 21.4 pmol/L (baseline) | Nephrogenic DI (partial or complete) |
| < 2.6 pmol/L (baseline) | Complete central DI |
| 2.6 - 21.3 pmol/L | Indeterminate - proceed to water deprivation or hypertonic saline test |
| > 4.9 pmol/L after hypertonic saline | Primary polydipsia |
| ≥ 4.9 pmol/L after hypertonic saline (with copeptin <4.9 before) | Central DI (partial or complete) |
Water Deprivation Test (classic; done when copeptin indeterminate)
Withhold fluids → dehydrate until urine Osm plateaus or 3-5% body weight lost → give desmopressin 2 µg IV/SC → measure urine Osm response:
| Condition | Urine Osm after dehydration | After Desmopressin |
|---|---|---|
| Normal | > 800 mOsm/kg | < 10% further rise |
| Complete Central DI | < 300 mOsm/kg | > 50% increase |
| Partial Central DI | 300-800 mOsm/kg | 10-50% increase |
| Complete Nephrogenic DI | < 300 mOsm/kg | < 10% increase |
| Partial Nephrogenic DI | 300-800 mOsm/kg | > 10% but incomplete increase |
| Primary Polydipsia | May reach > 800 mOsm/kg | < 10% increase |
Etiologic Workup (once type confirmed)
- MRI of hypothalamus, pituitary stalk, posterior pituitary (look for bright spot, stalk thickening, masses)
- CSF: tumor markers (β-HCG for germinoma, ACE for sarcoid)
- Genetic testing if family history
- If "idiopathic": annual CT/MRI for ≥4 years to catch occult tumors
Diagnostic Algorithm (from Goldman-Cecil Medicine)
Treatment
Central DI - Drug of Choice: Desmopressin (DDAVP)
- Synthetic vasopressin V2 agonist - no V1 (pressor) activity
- Routes: oral (0.1 mg tablets), intranasal spray (10 µg/spray), IV/SC
- Start low at bedtime; titrate to 1-2x/day dosing (duration of action 6-24 hours)
- Goal: reduce polyuria to tolerable level without causing hyponatremia
- Caution: Overtreatment → water retention → hyponatremia
Alternative agents for Central DI (if desmopressin not available):
- Chlorpropamide (sulfonylurea - potentiates ADH action)
- Carbamazepine / clofibrate (stimulate ADH release)
- Thiazide diuretics (paradoxical effect - see below)
Nephrogenic DI
No direct treatment except addressing the cause. Specific measures:
- Remove offending drug (e.g., stop lithium if possible)
- Low-sodium, low-protein diet (reduces solute load → less obligatory free water loss)
- Thiazide diuretics (paradoxical effect: cause mild volume depletion → ↑ proximal tubular Na/water reabsorption → less water reaches collecting duct → reduces polyuria by ~50%)
- NSAIDs (indomethacin - inhibit prostaglandins that antagonize ADH)
- Amiloride (specifically for lithium-induced nephrogenic DI - blocks lithium entry into collecting duct cells via ENaC channels)
Primary Polydipsia
- Treat underlying psychiatric disorder
- Behavioral therapy, fluid restriction
- Note: A 2021 RCT (Grade A evidence) showed GLP-1 agonist dulaglutide reduced polydipsia in primary polydipsia patients
Key Comparisons at a Glance
| Feature | Central DI | Nephrogenic DI | Primary Polydipsia |
|---|---|---|---|
| Serum Na | High | High | Low/normal |
| Plasma Osm | High | High | Low/normal |
| Urine Osm | Low (< 300) | Low (< 300) | Variable |
| ADH level | Low | High/Normal | Low/normal |
| Response to desmopressin | Yes (>50% ↑ Uosm) | No (<10%) | No |
| Copeptin | Very low | Very high (≥21.4) | Normal |
Recent evidence: A 2024 meta-analysis (PMID 38996052) in European Journal of Endocrinology found that post-pituitary surgery central DI is common but often transient - permanent central DI occurs in a significant subset and requires long-term desmopressin.
Sources: Goldman-Cecil Medicine 2-Vol Set, Henry's Clinical Diagnosis & Lab Methods, Tietz Textbook of Laboratory Medicine 7th Ed., Brenner & Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.