Diffused thyroiditis
Reading File
Finding Sources
Searching PubMed
thyroiditis classification pathology
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I have everything needed for a comprehensive answer. Here is the full write-up:
Diffuse Thyroiditis
"Diffuse thyroiditis" describes forms of thyroid inflammation where the entire gland is diffusely involved, as opposed to focal or nodular disease. The term most commonly points to Hashimoto thyroiditis (the prototype of diffuse autoimmune thyroiditis), but the full spectrum includes several clinically distinct entities. Below is a systematic overview.
Classification of Thyroiditis
Harrison's (22e) classifies thyroiditis by onset/duration and by presence or absence of pain:
| Category | Type | Key Feature |
|---|---|---|
| Acute | Suppurative (bacterial/fungal) | Rare; painful; fever |
| Subacute | Granulomatous (de Quervain's) | Painful; post-viral |
| Painless (lymphocytic/postpartum) | Autoimmune; transient | |
| Drug-induced (amiodarone, IFN, checkpoint inhibitors) | Variable | |
| Chronic | Hashimoto's (chronic lymphocytic) | Most common; autoimmune |
| Riedel's thyroiditis | Dense fibrosis; rare | |
| Atrophic thyroiditis | Autoimmune; no goiter |
- Harrison's Principles of Internal Medicine 22E, p. 3081
1. Hashimoto Thyroiditis (Chronic Autoimmune / Chronic Lymphocytic Thyroiditis)
The most important and common form of diffuse thyroiditis, and the leading cause of hypothyroidism in iodine-sufficient regions.
Epidemiology
- Peak prevalence: 45-65 years
- Female:male ratio = 10:1 to 20:1
- Also a major cause of non-endemic goiter in children
Pathogenesis
Caused by breakdown of self-tolerance to thyroid autoantigens. Key immune mechanisms:
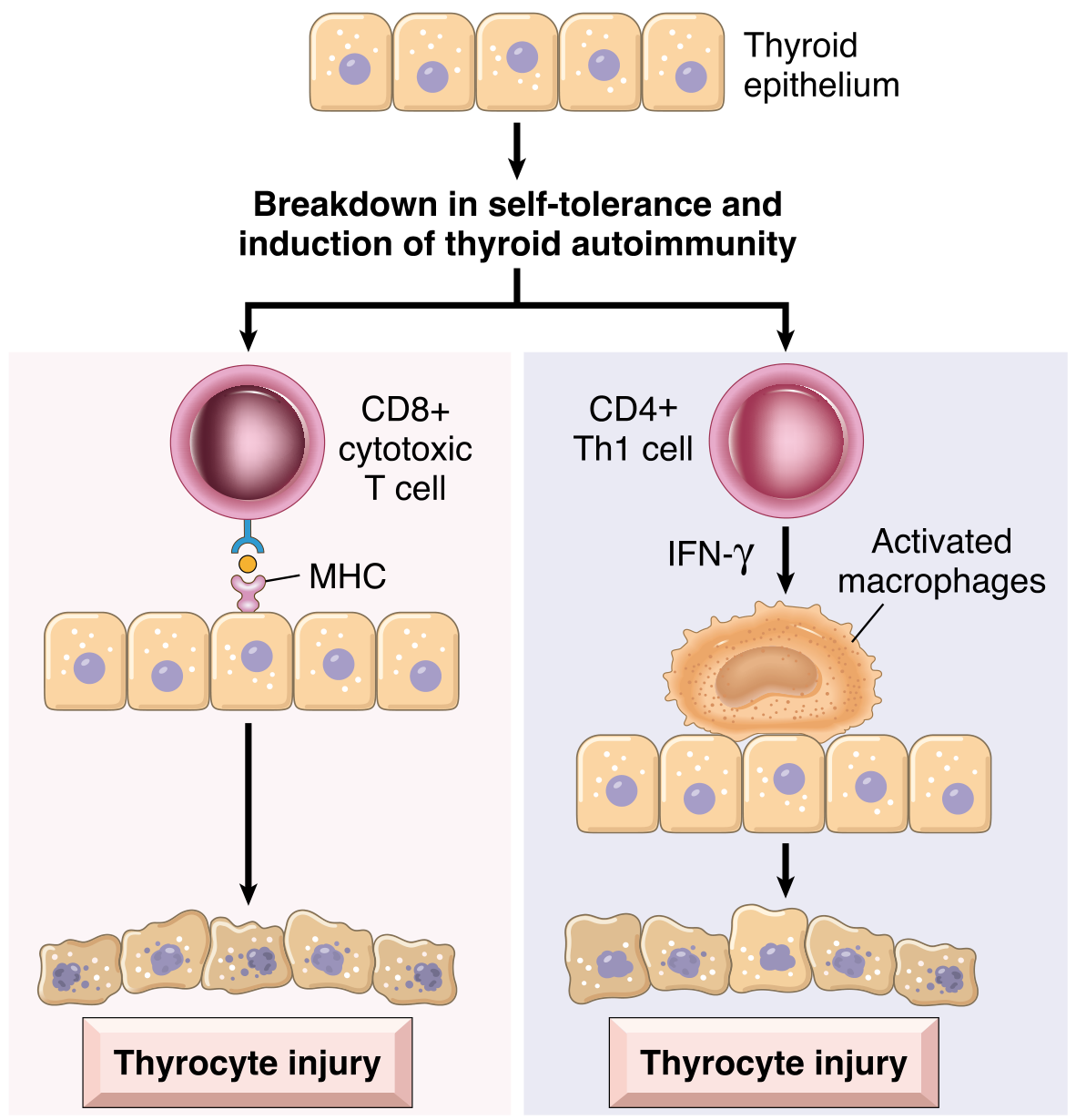
Fig. Pathogenesis of Hashimoto thyroiditis (Robbins & Kumar Pathologic Basis of Disease)
- CD8+ cytotoxic T cells directly kill thyroid follicular cells via MHC-restricted recognition
- Cytokine-mediated injury: CD4+ Th1 cells release IFN-γ, activating macrophages and damaging follicles
- Autoantibodies: anti-thyroglobulin and anti-thyroid peroxidase (TPO) antibodies cause antibody-dependent cytotoxicity and complement-mediated follicular damage
Genetic risk loci include CTLA4, PTPN22, and IL2RA polymorphisms - all regulators of T-cell responses.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 998
Morphology
- Thyroid is diffusely enlarged, well-demarcated, pale yellow-tan, firm, and somewhat nodular
- Extensive lymphoplasmacytic infiltration with germinal centers
- Atrophic follicles lined by oncocytes (Hürthle cells) - metaplastic eosinophilic cells
- Interstitial fibrosis (not extending beyond the capsule - distinguishes it from Riedel's)
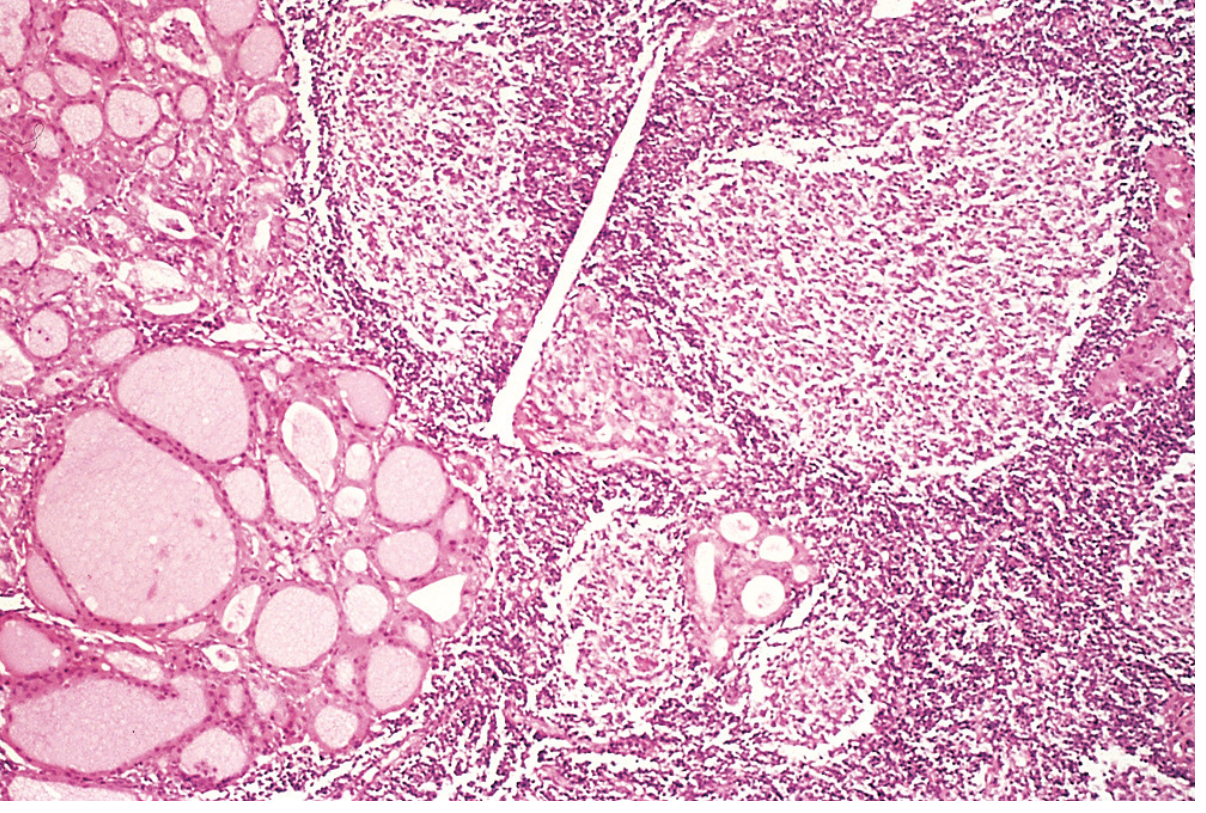
Fig. Hashimoto thyroiditis - lymphocytic infiltrate with germinal centers; residual follicles lined by oncocytic (Hürthle) cells. (Robbins, Cotran & Kumar Pathologic Basis of Disease)
FNA biopsy findings: oncocytes + heterogeneous lymphocytes = characteristic Hashimoto pattern.
Clinical Features
-
Painless symmetric diffuse goiter
-
Gradual onset of hypothyroidism (low T4/T3, elevated TSH)
-
Transient early thyrotoxicosis ("hashitoxicosis") due to follicle disruption and hormone release
-
Associated autoimmune diseases: type 1 diabetes, autoimmune adrenalitis, SLE, myasthenia gravis, Sjögren syndrome
-
Increased risk of extranodal marginal zone B-cell lymphoma of the thyroid (rare)
-
Controversial association with papillary thyroid carcinoma
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 999
2. Subacute Granulomatous Thyroiditis (de Quervain's Thyroiditis)
- Also called: viral thyroiditis, painful thyroiditis, giant-cell thyroiditis
- Etiology: Post-viral (mumps, coxsackie, influenza, adenovirus, echovirus; also reported with SARS-CoV-2 and COVID vaccination)
- Female:male = 5:1; age 20-60
Clinical Course (Triphasic)
- Thyrotoxic phase - follicle disruption releases preformed hormone; TSH suppressed
- Hypothyroid phase - depleted hormone stores; transient hypothyroidism
- Recovery - euthyroidism in most patients
Key Features
- Painful, tender, firm thyroid - often referred to throat or ears
- Elevated ESR (hallmark), low/absent anti-TPO antibodies
- Low radioactive iodine uptake (RAIU)
- Granulomatous inflammation on histology (giant cells engulfing colloid)
- Self-limited; NSAIDs for pain; corticosteroids for severe cases
3. Subacute Lymphocytic (Painless) Thyroiditis
Includes postpartum thyroiditis and sporadic painless thyroiditis.
- Autoimmune etiology (anti-TPO antibodies are high, unlike de Quervain's)
- Painless diffuse/nodular goiter
- Same triphasic course as de Quervain's but painless
- ESR is normal
- Histology: lymphocytic infiltration without granulomas
- Postpartum variant: occurs within 1 year of delivery in ~5-10% of women; may recur with subsequent pregnancies
4. Acute (Suppurative) Thyroiditis
- Rare bacterial/fungal infection of the thyroid
- Common organisms: Staphylococcus, Streptococcus, Enterobacter; in immunocompromised: fungi, mycobacteria, Pneumocystis
- In children: often due to a piriform sinus fistula (left-sided; remnant of 4th branchial pouch)
- Features: acute painful thyroid, fever, dysphagia, erythema; leukocytosis + elevated ESR; thyroid function usually normal
- Management: antibiotics guided by FNA culture; surgery if abscess forms (CT/US to localize)
5. Riedel's Thyroiditis (Fibrous Thyroiditis)
- Rare; replaces thyroid parenchyma with dense, invasive fibrosis that extends beyond the capsule into surrounding neck structures (differentiating it from Hashimoto's)
- "Woody, hard" thyroid on examination
- Can cause tracheal/esophageal compression and hypoparathyroidism
- Associated with IgG4-related disease in some cases
- TPO antibodies may be present
- Treatment: tamoxifen, corticosteroids; surgery for decompression
Comparative Summary (Scott-Brown's Classification)
| Feature | Hashimoto's | Postpartum/Painless | de Quervain's | Suppurative | Riedel's |
|---|---|---|---|---|---|
| Sex ratio (F:M) | 8-9:1 | - | 5:1 | 1:1 | 3-4:1 |
| Pain | No | No | Yes | Yes | No |
| Cause | Autoimmune | Autoimmune | Unknown (viral) | Infectious | Unknown |
| TPO antibodies | High | High | Low | Absent | Present |
| ESR | Normal | Normal | High | High | Normal |
| Thyroid function | Hypothyroid | Mixed | Mixed | Euthyroid | Euthyroid |
| Gross pathology | Symmetrical diffuse enlargement, firm, pale | Firm, nodular | Firm, nodular | Abscess | Rock-hard, adherent |
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Table 58.4
Drug-Induced Thyroiditis
Several drugs can cause diffuse thyroid inflammation:
- Amiodarone - type 1 (iodine-induced hyperthyroidism) or type 2 (destructive thyroiditis)
- Lithium - inhibits thyroid hormone release
- Interferon-alpha, interleukin-2 - trigger autoimmune thyroiditis
- Tyrosine kinase inhibitors and immune checkpoint inhibitors - increasingly recognized causes
Diagnosis at a Glance
| Test | Hashimoto's | de Quervain's | Painless | Suppurative |
|---|---|---|---|---|
| TSH | High (usually) | Variable | Variable | Normal |
| Anti-TPO | ++++ | +/- | +++ | - |
| ESR | Normal | Very high | Normal | High |
| RAIU | Low | Very low | Low | Normal |
| FNA | Oncocytes + lymphocytes | Giant cells + granulomas | Lymphocytes | PMNs + organisms |
| Ultrasound | Diffuse heterogeneous, hypoechoic | Diffuse hypoechoic | Variable | Abscess |
Almost all euthyroid diffuse goiters in the US are due to Hashimoto thyroiditis, confirmable by anti-TPO antibody measurement. - Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.