Tonsillitis urgerry steps refer standard ent text book and give answers in image
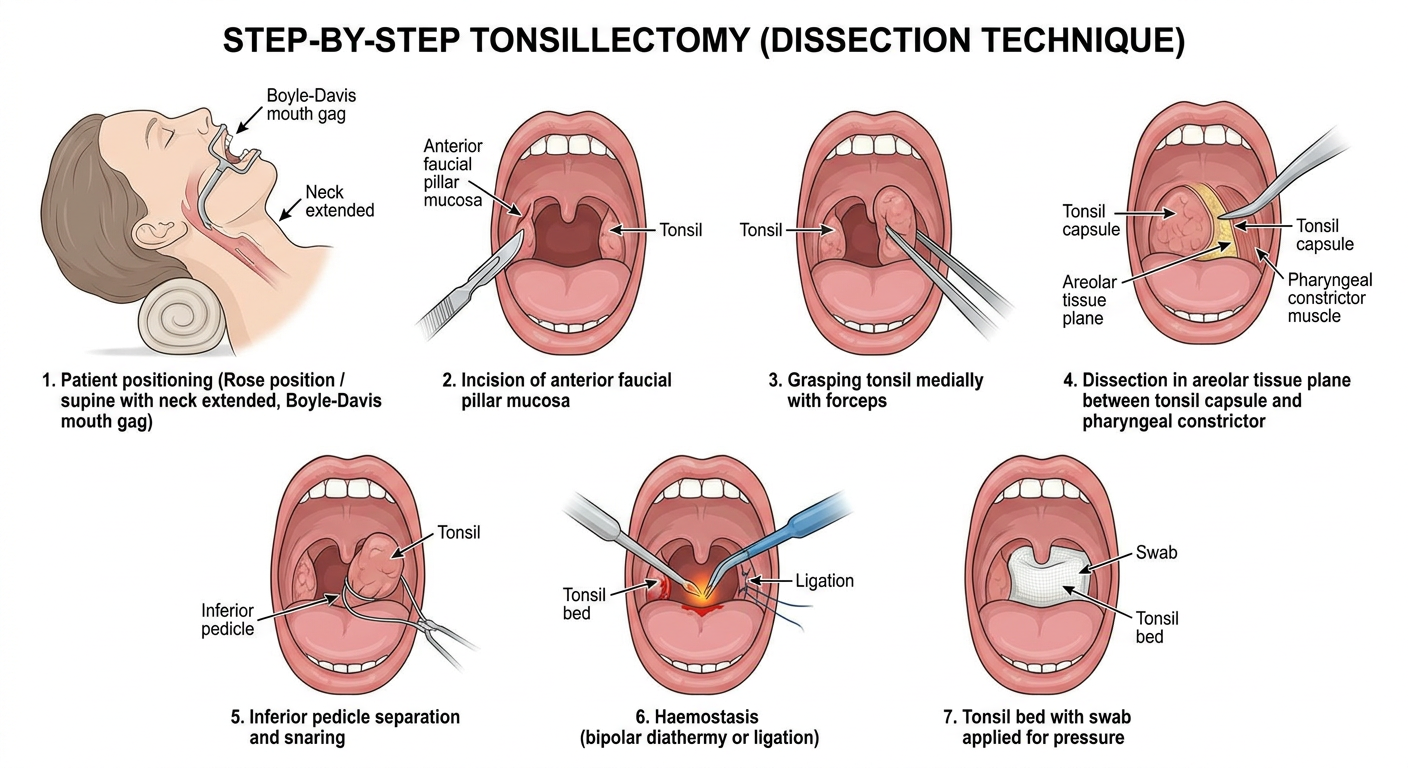
A detailed medical educational diagram showing the step-by-step surgical steps of tonsillectomy (dissection technique), labeled with numbered steps: 1. Patient positioning (Rose position / supine with neck extended, Boyle-Davis mouth gag), 2. Incision of anterior faucial pillar mucosa, 3. Grasping tonsil medially with forceps, 4. Dissection in areolar tissue plane between tonsil capsule and pharyngeal constrictor, 5. Inferior pedicle separation and snaring, 6. Haemostasis (bipolar diathermy or ligation), 7. Tonsil bed with swab applied for pressure. Clean anatomical cross-section illustration style with labels on white background.
Tonsillectomy - Surgical Steps
Indications (Bailey & Love, Table 52.1)
| Absolute | Relative |
|---|---|
| Sleep apnoea / airway obstruction | Recurrent acute tonsillitis (Paradise criteria) |
| Suspected tonsillar malignancy | Chronic tonsillitis |
| Cor pulmonale | Peritonsillar abscess (quinsy) |
| Febrile convulsions, diphtheria carriers |
Pre-operative Points
- Procedure ideally done when tonsils are not acutely infected
- Check bleeding history and coagulation status
- Type & screen blood in children under 15 kg
- General anaesthesia (endotracheal intubation with a south-facing RAE tube)
Step-by-Step: Dissection Tonsillectomy (Cold Steel - Standard Technique)
STEP 1 - Patient Positioning
- Rose position (supine) with neck extended over a shoulder roll
- Head ring to stabilize the head
- Boyle-Davis mouth gag inserted to retract the tongue and keep the mouth open; suspended from a Draffin bipod or Boyle-Davis stand
STEP 2 - Exposure
- The surgeon sits at the head of the table
- The soft palate and uvula are retracted superiorly
- Both tonsils are visualized simultaneously
STEP 3 - Incision of Anterior Faucial Pillar
- The mucosa of the anterior faucial pillar is incised with a curved scissors or scalpel at the junction of the pillar with the tonsil
- This exposes the tonsil capsule
STEP 4 - Grasping the Tonsil
- The tonsil is grasped with Allis forceps or a tonsil-holding forceps and pulled medially to stretch the mucosa taut and open the dissection plane
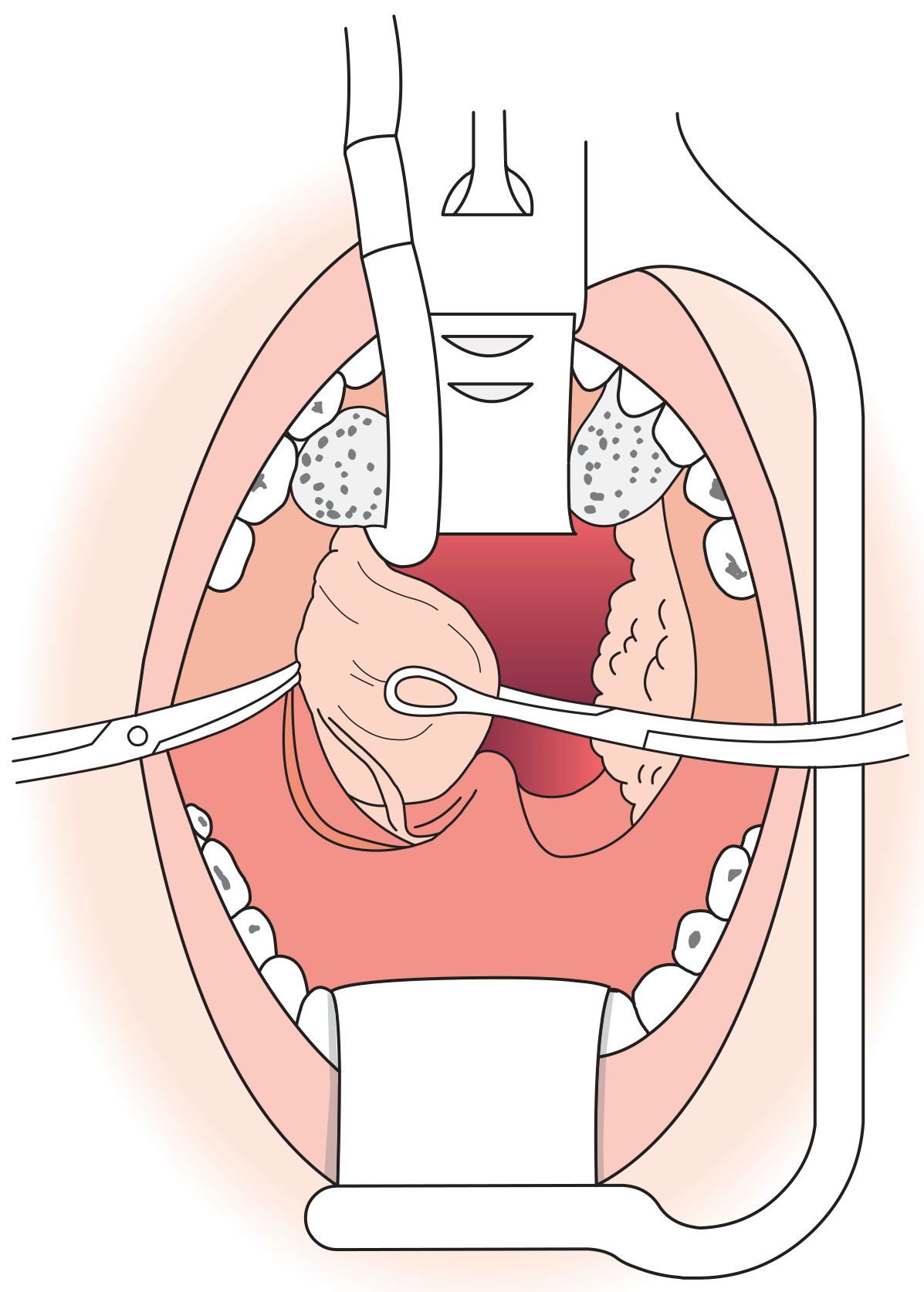
STEP 5 - Dissection in the Peritonsillar Plane
- Blunt dissection (with a Mollison's or St. Clair Thompson's dissector or pledget of gauze) proceeds in the plane of loose areolar tissue between the tonsil capsule and the pharyngeal constrictor muscles
- Dissection begins at the superior pole and proceeds inferiorly
- This plane is largely avascular except at the poles
- The tonsil is progressively separated from its bed, staying outside the capsule at all times
STEP 6 - Division of the Inferior Pedicle
- Once dissection is complete, a small inferior pedicle remains connecting the tonsil to the lingual tonsil / tongue base
- A tonsil snare or scissors is used to sever this pedicle
- The tonsil is then fully removed
STEP 7 - Haemostasis
- A tonsil swab (rolled gauze) is placed in the tonsillar fossa and pressure applied for several minutes
- Bleeding points are then controlled by:
- Ligation (silk ties) - traditional preferred method
- Bipolar diathermy - commonly used
- Cold steel + ties has the lowest secondary haemorrhage rate (NPTA data)
STEP 8 - Inspection of the Bed
- Both fossae inspected for residual bleeding
- Mucosa of pillars may be approximated if needed (rare)
- Throat pack (if used) is removed and counted
Surgical Steps Diagram (Generated Reference)
Alternative Techniques (Scott-Brown's, p. 482)
| Technique | Notes |
|---|---|
| Cold steel + ties/packs | Lowest secondary bleed rate (1.0%) - GOLD STANDARD |
| Cold steel + bipolar diathermy | Primary bleed 0.5%, secondary 2.3% |
| Bipolar diathermy forceps | Primary bleed 0.4%, secondary 4.3% |
| Coblation | Probe coagulates + cuts; NPTA found unacceptably high post-op bleed rates; less post-op pain claimed |
| Ultrasonic dissection | Oscillating blade cuts + coagulates; pain benefit unproven |
| Laser | CO2 or KTP laser; rarely used now |
Post-operative Care
- Recovery position (tonsillar position) - lateral decubitus (see figure below) to prevent aspiration of blood
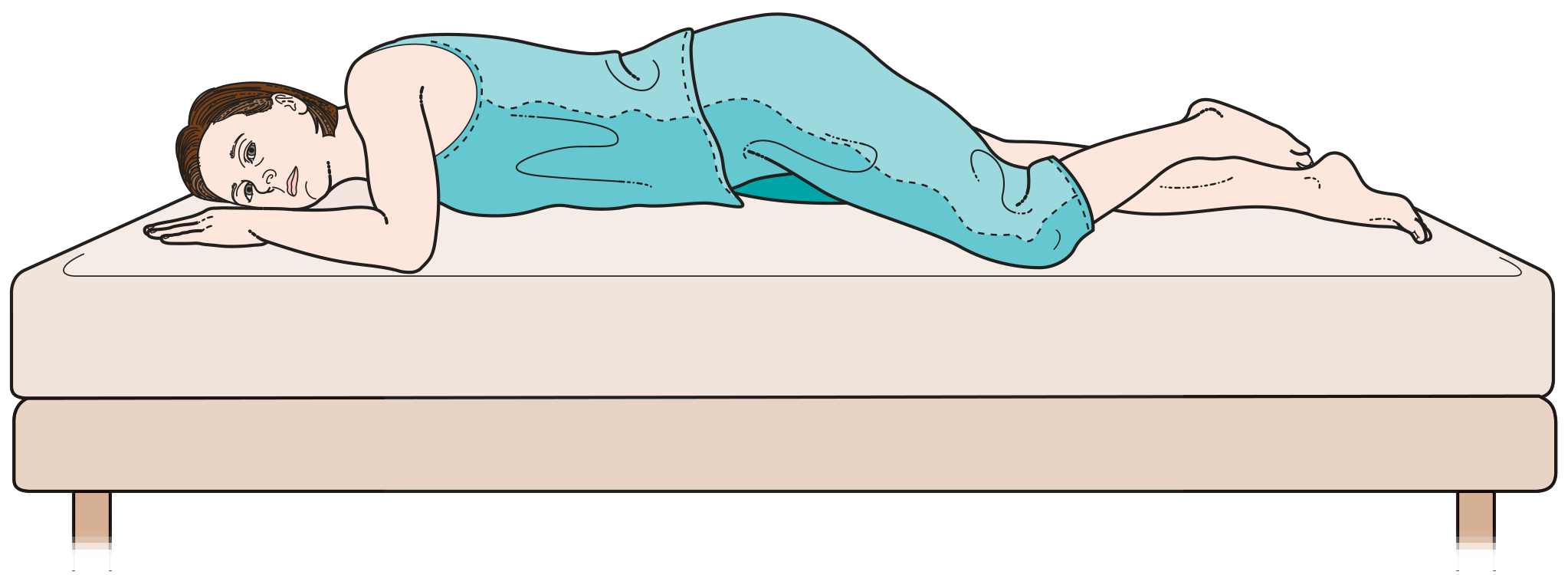
- Monitor pulse and blood pressure closely - excessive swallowing = sign of bleeding
- Encourage normal diet and oral analgesics
- Warn about referred otalgia (via glossopharyngeal nerve) - this is normal
- Secondary haemorrhage can occur up to 10 days post-op (usually infective)
Complications (Bailey & Love, Summary Box 52.6)
- Primary haemorrhage (within 24 hrs) - reactionary; requires return to theatre
- Secondary haemorrhage (days 5-10) - infective; IV antibiotics + possible re-operation
- Post-op pain and otalgia
- Airway obstruction
- Velopharyngeal insufficiency
- Injury to teeth, lips, or oropharyngeal structures
- Nasopharyngeal stenosis (rare)
- [Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol 2), pp. 481-482](Scott-Brown's Vol 2, Chapter 38) - Tonsillectomy Technique
- [Bailey & Love's Short Practice of Surgery 28th Ed, pp. 807-808](Bailey & Love, Chapter 52) - Tonsillectomy
- Cummings Otolaryngology Head and Neck Surgery - Palatine Tonsillectomy
Create a detailed surgical guide PDF on tonsillectomy complications and management
Medical educational infographic showing tonsillectomy complications classification. Two main branches: PRIMARY haemorrhage (within 24 hours, reactionary, intraoperative causes) and SECONDARY haemorrhage (days 5-10, infective, slough separation). Include statistics: overall haemorrhage rate 0.1-3%, readmission 4.57%, return to theatre 1.44%. Clean clinical chart style with red color coding for bleeding, amber for infection, blue for airway complications.
Medical step-by-step flowchart for management of post-tonsillectomy haemorrhage. Steps: 1. Assessment (ABC, vitals, blood loss estimate), 2. Resuscitation (IV access, fluids, cross-match), 3. Primary bleed - return to theatre for haemostasis, 4. Secondary bleed - IV antibiotics plus examination, 5. Haemostasis methods: suture ligation, bipolar diathermy, haemostatic gauze. Green boxes for stable patient, red boxes for emergency. Professional clinical algorithm flowchart style on white background.
Medical educational poster showing all complications of tonsillectomy organized by timing. Section 1 IMMEDIATE (0-24h): Primary haemorrhage, airway obstruction, anaesthetic complications. Section 2 EARLY (1-10 days): Secondary haemorrhage, infection, dehydration, pain, referred otalgia. Section 3 LATE (weeks-months): Velopharyngeal insufficiency, nasopharyngeal stenosis, TMJ dysfunction, Grisel syndrome. Color-coded timeline bar at top. Clean medical illustration style.
mkdir -p /home/daytona/workspace/tonsillectomy-guide && ls /home/daytona/workspa…
Failed to create session: bad request: failed to resolve container IP after 3 attempts: no IP address found. Is the Sandbox started?
We encountered an error while processing your request. Please try again or reach out to us for help.