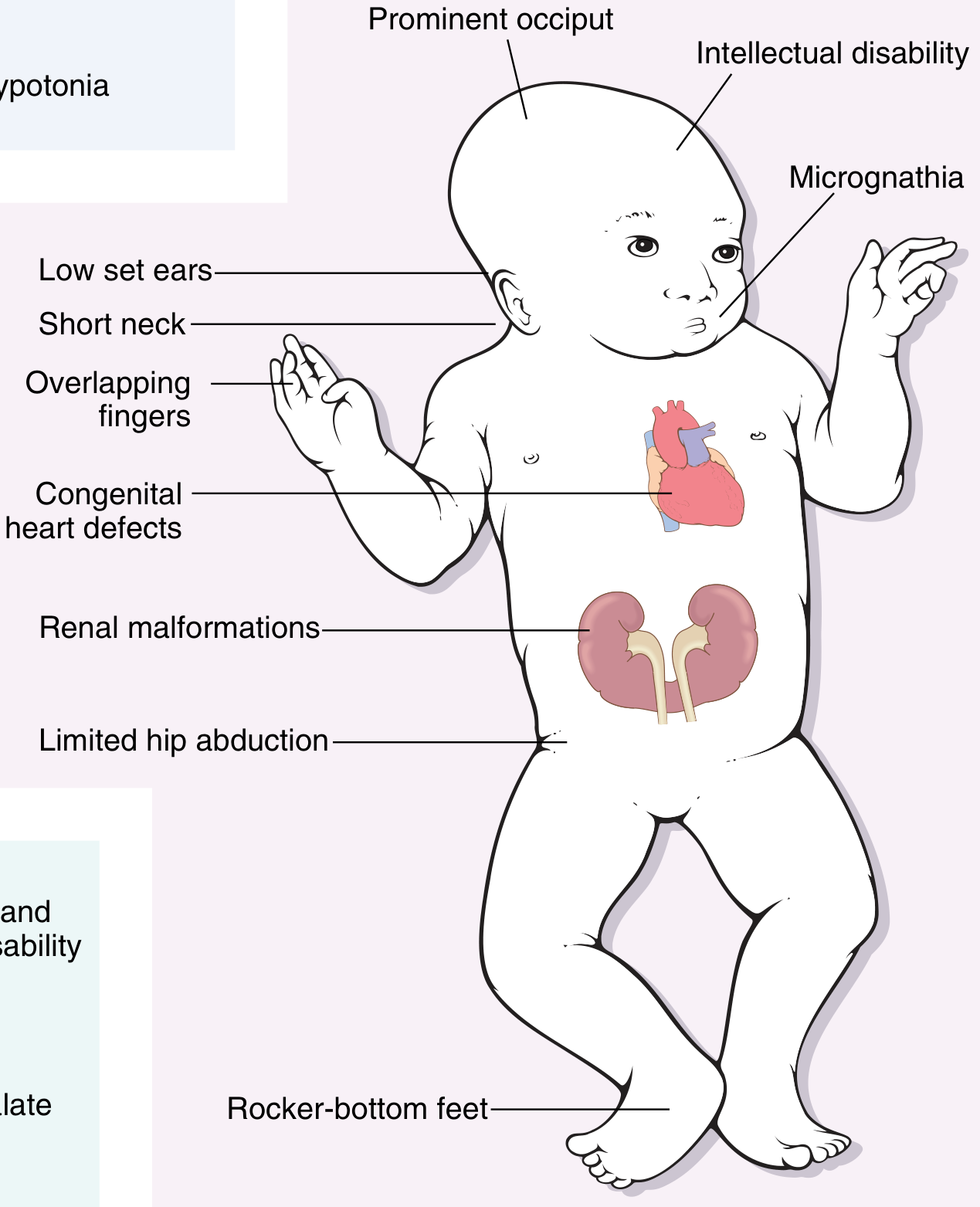
Clinical findings in downsyndrome
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive, well-illustrated answer. Here it is:
Clinical Findings in Down Syndrome (Trisomy 21)
Incidence: ~1 in 700 live births | Karyotype: 47,XX/XY,+21 (trisomy); also translocation and mosaic forms
1. Dysmorphic Facial Features
The classic facial features are usually recognizable at birth:
| Feature | Description |
|---|---|
| Flat facial profile | Depressed nasal bridge with flat midface |
| Oblique palpebral fissures | Upward-slanting eye openings |
| Epicanthic folds | Skin fold over the inner corner of each eye |
| Brushfield spots | Speckled iris (white/grey spots) |
| Brachycephaly | Flat occiput, round head |
| Low-set ears | Small, dysplastic pinnae |
| Macroglossia | Large tongue, often protruding |
| Short neck | With loose skin on the nape |
2. Musculoskeletal / Body
- Hypotonia - often the first abnormality noticed in the newborn; generalized muscle floppiness
- Short stature - slow growth throughout childhood
- Short, broad hands with a single transverse palmar crease (simian crease)
- Fifth finger clinodactyly - incurved 5th digit
- Sandal gap - wide space between 1st and 2nd toes
- Limited hip abduction
- Atlanto-axial instability (cervical C1-C2 laxity) - risk of spinal cord compression
3. Neurological / Intellectual
- Intellectual disability - the leading single genetic cause; ranges from moderate to mild. May not be obvious in early infancy but becomes apparent by end of first year.
- Hypotonia contributes to motor delay
- Alzheimer disease - virtually all patients with trisomy 21 older than age 40 develop neuropathologic changes of Alzheimer disease; amyloid-beta precursor gene on chromosome 21 is implicated
- Behavioral phenotype: typically placid, cheerful, and cooperative in childhood; may become more behaviorally complex in adolescence
4. Cardiovascular (Most Common Cause of Early Death)
Congenital heart disease occurs in ~40-50% of patients. Distribution:
| Defect | Frequency |
|---|---|
| Atrioventricular septal defect (AVSD) | 43% |
| Ventricular septal defect (VSD) | 32% |
| Atrial septal defect (ASD) | 19% |
| Tetralogy of Fallot | 6% |
Cardiac complications are responsible for most deaths in infancy and early childhood.
5. Gastrointestinal
- Duodenal atresia ("double bubble" sign on X-ray) - much more common than in other disorders
- Tracheo-esophageal fistula / esophageal atresia
- Hirschsprung disease (intestinal aganglionosis)
- Intestinal stenosis
6. Hematological / Oncologic
- 20-fold increased risk of precursor B-cell acute lymphoblastic leukemia (ALL)
- 500-fold increased risk of acute myeloid leukemia (AML)
- Transient myeloproliferative disorder (TMD): up to 10% of Down syndrome newborns develop peripheral leukocytosis with blasts and megakaryoblasts - usually resolves spontaneously but progresses to acute megakaryoblastic leukemia in 23-30% of cases. Caused by somatic mutations in the GATA1 gene acquired during fetal life.
7. Immunological
- Abnormal immune responses, predominantly affecting T-cell function
- Predisposition to serious infections, especially pulmonary infections
- Thyroid autoimmunity - Hashimoto thyroiditis
- Hypothyroidism develops in up to 50% of patients older than 40 years
8. Ophthalmologic
- Cataracts (congenital or early-onset)
- Refractive errors (myopia common)
- Strabismus
- Nystagmus
9. ENT / Respiratory
- Obstructive sleep apnea (OSA) - high prevalence due to midface hypoplasia, macroglossia, and hypotonia
- Hearing loss (both conductive and sensorineural)
- Recurrent otitis media
10. Urological
- Cryptorchidism
- Hypospadias
- Renal malformations
Summary Table of Key Features
| System | Key Finding |
|---|---|
| Face | Flat profile, epicanthic folds, oblique palpebral fissures |
| Neurology | Intellectual disability (moderate-mild), Alzheimer after age 40 |
| Muscle | Hypotonia (first sign at birth) |
| Hands | Single palmar crease, clinodactyly, short broad hands |
| Heart | AV septal defect (most common CHD), VSD, ASD |
| GI | Duodenal atresia, Hirschsprung disease |
| Blood | 500x risk AML, 20x risk ALL; transient myeloproliferative disorder |
| Immune | Recurrent infections, thyroid autoimmunity, hypothyroidism |
| Eyes | Cataracts, Brushfield spots |
| Ear/Airway | OSA, hearing loss |
Karyotypic Variants and Their Clinical Significance
| Type | Karyotype | Notes |
|---|---|---|
| Standard trisomy 21 | 47,XX,+21 | ~95% of cases; maternal nondisjunction; risk increases with maternal age |
| Robertsonian translocation | 46,XX,der(14;21)(q10;q10),+21 | ~4% of cases; can be familial; maternal age irrelevant |
| Mosaic | 46,XX/47,XX,+21 | ~1% of cases; milder phenotype; may have near-normal intelligence |
Prognosis: Improved medical care has extended median survival to 47-60 years (up from 25 years in 1983), though Alzheimer disease and recurrent infections remain major long-term concerns.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology; Thompson & Thompson Genetics and Genomics in Medicine, 9th ed.; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.