stye or hordeolum.
Reading File
Finding Sources
Searching PubMed
hordeolum stye treatment management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full write-up:
Hordeolum (Stye)

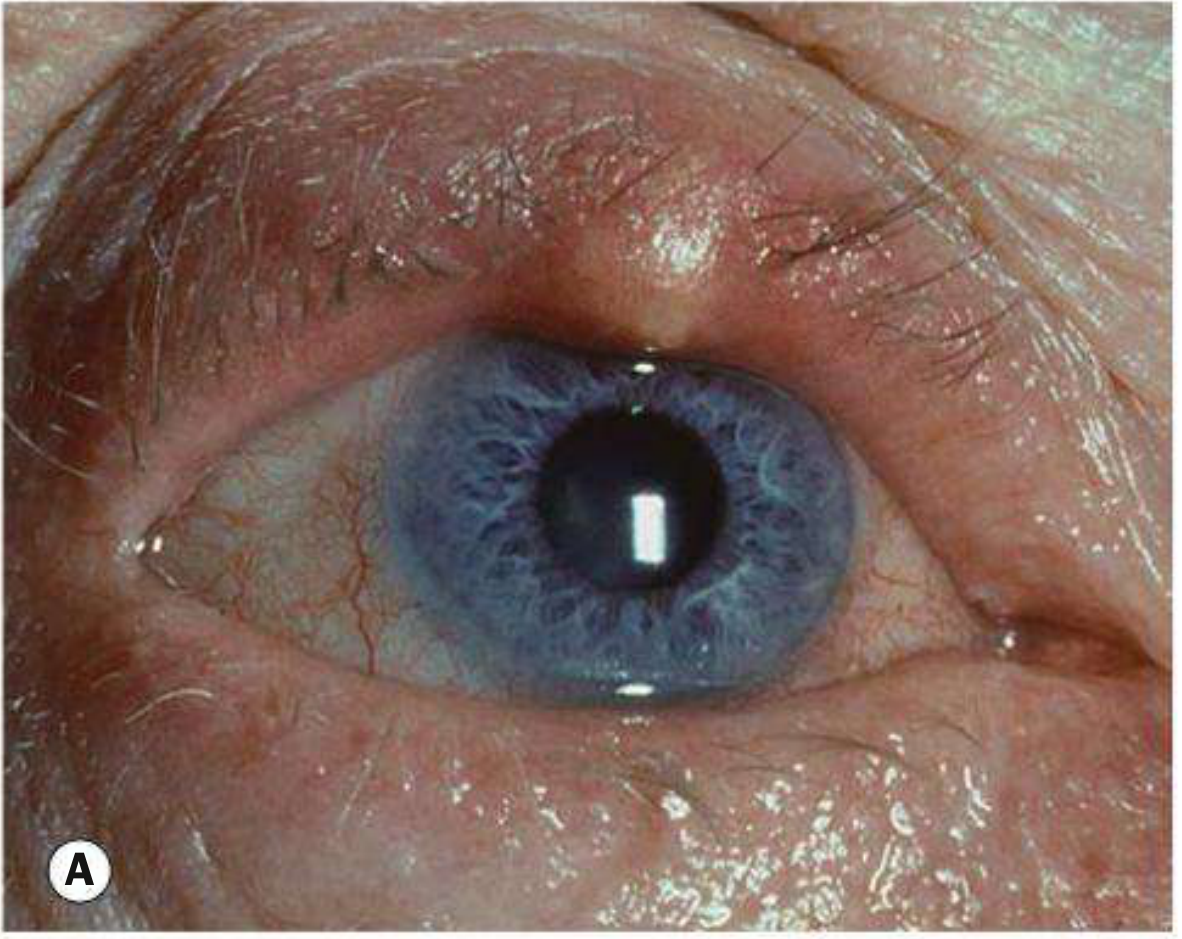
Definition
A hordeolum is an acute, tender, purulent infection (abscess) of an oil gland or hair follicle of the eyelid. It comes in two forms:
| Feature | External Hordeolum (Stye) | Internal Hordeolum |
|---|---|---|
| Gland involved | Gland of Zeis (sebaceous) or gland of Moll (sweat) - associated with lash follicle | Meibomian gland (tarsal gland) |
| Location | Lid margin, pointing anteriorly through skin; lash often at apex | Inner surface of the tarsal plate (conjunctival side) |
| Appearance | Visible pustule at lash line | Pustule on inner lid surface; eyelid must be everted to visualize |
| Common in | Children and young adults | Any age |
The causative organism is almost always Staphylococcus aureus (or occasionally other Staphylococcus species).
Clinical Features
Symptoms:
- Acute eyelid lump, tenderness, swelling
- Pain, erythema
Signs:
- Focal, tender, erythematous nodule or pustule at or near the lid margin
- Eyelid edema
- May "come to a head" - visible pointing with mucopurulent discharge
- Occasionally the entire lid margin is involved with multiple lesions
Hordeolum vs. Chalazion
These are often confused. Key distinctions:
| Hordeolum | Chalazion | |
|---|---|---|
| Nature | Acute bacterial infection | Chronic sterile granulomatous inflammation |
| Pain | Acutely tender | Usually painless or minimally tender |
| Onset | Rapid | Subacute to chronic |
| Cause | Bacterial (Staph) abscess | Obstruction/lipogranuloma of meibomian gland |
| Relationship | Can evolve into chalazion | May develop from an old hordeolum |
Clinical differentiation of an acute chalazion from an internal hordeolum may be impossible, but treatment is the same. - Tintinalli's Emergency Medicine
Differential Diagnosis
- Preseptal (periorbital) cellulitis - diffuse eyelid erythema, edema, warmth; more systemic signs; requires urgent management
- Chalazion - subacute, non-infectious, non-tender nodule
- Pyogenic granuloma - benign, deep-red pedunculated conjunctival lesion, often follows chalazion or trauma
- Sebaceous carcinoma - suspect in older patients with recurrent chalazia, madarosis (lash loss), or chronic unilateral blepharitis; must biopsy
- Dacryocystitis - infection of the lacrimal sac, medial to the eye
- Impetigo - superficial skin infection, honey-colored crusts
- Forniceal foreign body - especially in contact lens wearers
Treatment
First-line (conservative)
- Warm compresses for 10-15 minutes, as frequently as possible (q.i.d. recommended) with gentle massage over the lesion - this is the mainstay of treatment
- Topical antibiotics - erythromycin ointment, bacitracin, or tobramycin b.i.d. for 1-2 weeks (applied to lid margin)
Epilation
- Removing the offending eyelash may facilitate drainage and speed resolution
Incision and drainage (I&D)
- If a pustule is clearly pointing, nicking it with a 25-gauge needle (or small scalpel blade) and expressing pus produces faster cure
- For internal hordeolum: evert the lid to find the pustule on the inner surface and nick with a needle
- More formal I&D may be needed for lesions unresponsive to conservative therapy
- If considering I&D, refer to ophthalmology unless experienced with the procedure
Systemic antibiotics
- Usually not needed
- Indicated if there is significant surrounding lid cellulitis
- Antistaphylococcal agents: dicloxacillin, cephalosporins (e.g., cephalexin)
- If hordeolum worsens or progresses to preseptal cellulitis, manage accordingly
Recurrent/multiple lesions
- Consider chronic low-dose doxycycline 20-50 mg orally daily to b.i.d. for its antibacterial and anti-inflammatory properties
- Evaluate for underlying acne rosacea or blepharitis
Complications
- Preseptal (periorbital) cellulitis - most important complication; spread of infection beyond the hordeolum
- Internal hordeolum evolving into a chronic chalazion
- Rarely, post-septal (orbital) cellulitis
When to Refer
- Lesion fails to respond to conservative therapy in 3-4 weeks
- Significant surrounding cellulitis
- Suspected sebaceous carcinoma (recurrent, atypical, or in older patients)
- I&D required (unless the clinician is trained)
- Any concern for preseptal or orbital cellulitis
Sources: Wills Eye Manual 6.2 | Tintinalli's Emergency Medicine, p.1581 | Kanski's Clinical Ophthalmology, p.81 | Roberts & Hedges' Clinical Procedures in Emergency Medicine, p.1511 | Rosen's Emergency Medicine, p.893
Do it requqred medecin if it is normal
Finding Sources
The content from the previous session is sufficient to answer this directly and accurately.
Does a Normal Stye Need Medicine?
No - for a typical, uncomplicated stye, medicine is NOT required.
The single most important treatment is:
Warm compresses - applied for 10-20 minutes, 4 times a day. This softens the blockage, promotes drainage, and allows the stye to heal on its own.
Most styes resolve completely within 7-14 days with warm compresses alone.
When Medicine IS Added
Topical antibiotics (e.g., erythromycin ointment) are often prescribed but evidence for their benefit in an uncomplicated stye is limited. They are considered optional in mild cases. Medicine becomes necessary in specific situations:
| Situation | What is needed |
|---|---|
| Stye is not improving after 1-2 weeks | Topical antibiotic ointment (erythromycin, bacitracin) |
| Surrounding eyelid is red, warm, swollen (cellulitis starting) | Oral antibiotics (e.g., cephalexin, dicloxacillin) |
| Multiple styes or frequent recurrences | Low-dose doxycycline (oral, long course) |
| Spreading infection / preseptal cellulitis | Oral or IV antibiotics urgently |
| Stye won't drain and is large | Incision and drainage (by a doctor) |
Simple Summary
| Uncomplicated stye | Complicated stye |
|---|---|
| Warm compresses only | Add topical or oral antibiotics |
| Resolves in 1-2 weeks | May need drainage or specialist referral |
| No medicine needed | Medicine is necessary |
Do NOT squeeze or try to pop a stye yourself - this can spread the infection.
If the stye does not improve after 2 weeks of warm compresses, or if the eyelid becomes increasingly red and swollen, see a doctor.
- Wills Eye Manual, Section 6.2 | Tintinalli's Emergency Medicine, p.1581 | Kanski's Clinical Ophthalmology, p.81
Causes?
Finding Sources
Finding Sources
Reading File
Reading File
Here is a complete breakdown of the causes of a hordeolum:
Causes of a Stye (Hordeolum)
Primary Cause - The Bacteria
The direct cause is almost always Staphylococcus aureus - a bacterium that normally lives on the skin. When it infects a blocked or inflamed eyelid gland, a stye forms.
Occasionally other Staphylococcus species are involved.
What Gets Infected - The Glands
The bacteria target specific glands in the eyelid:
| Gland | Type | Leads to |
|---|---|---|
| Gland of Zeis | Sebaceous (oil) gland at lash follicle | External hordeolum |
| Gland of Moll | Sweat gland at lash follicle | External hordeolum |
| Meibomian gland | Large oil gland inside the tarsal plate | Internal hordeolum |
Risk Factors - What Makes It More Likely
These conditions predispose a person to getting styes:
Eyelid conditions:
- Blepharitis (chronic eyelid margin inflammation) - the most common predisposing condition; bacteria overgrow along the lid margin
- Meibomian gland dysfunction - blocked gland orifices allow bacteria to accumulate
Skin conditions:
- Acne rosacea - associated with chronic meibomian gland inflammation; patients often get recurrent styes and chalazia
- Seborrheic dermatitis - linked to blepharitis and eyelid overgrowth of Staph
Behavioral/hygiene factors:
- Touching or rubbing the eyes with unwashed hands - directly inoculates bacteria
- Wearing old or contaminated makeup - mascara and eyeliner can harbor Staphylococcus
- Not removing eye makeup before sleep - blocks gland orifices
- Wearing contact lenses improperly - can introduce organisms
Systemic conditions:
- Diabetes mellitus - impaired immunity makes infections more frequent and slower to resolve
- Immunocompromised states - any cause of reduced immunity (HIV, chemotherapy, steroids)
- High stress / poor sleep - weakens local immune defenses
Previous styes - having had one increases the risk of recurrence, especially if the underlying blepharitis or rosacea is untreated.
In Simple Terms
A stye happens when Staph bacteria get into a blocked or inflamed oil gland at the eyelid, usually because of poor lid hygiene, chronic blepharitis, or simply touching the eye with dirty hands.
Sources: Wills Eye Manual, Section 6.2 | Kanski's Clinical Ophthalmology, p.81 | Rosen's Emergency Medicine, p.893 | Tintinalli's Emergency Medicine, p.1581
This is a shared conversation. Sign in to Orris to start your own chat.