Pseudophakia
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Here is a comprehensive overview of pseudophakia drawn from authoritative ophthalmology textbooks.
Pseudophakia
Definition
Pseudophakia (Greek: pseudo = false + phakos = lens) describes an eye in which the natural crystalline lens has been surgically removed and replaced by an artificial intraocular lens (IOL). It is the standard state of an eye after successful modern cataract surgery (phacoemulsification + IOL implantation). It is distinct from aphakia, in which no lens is present at all.
Context and Significance
The majority of cataract surgeries worldwide result in pseudophakia. The artificial IOL is typically placed in the posterior chamber (within the capsular bag), though anterior chamber and sulcus-fixated IOLs are also used. The IOL corrects the high hyperopia that would otherwise result from lens removal.
Gonioscopic finding: A wide-open anterior chamber angle (Grade 4, 35-45°) is characteristic of pseudophakia, similar to myopic eyes, due to the altered lens-iris relationships. - Kanski's Clinical Ophthalmology, 10th ed.
Optical Properties
- Pseudophakic eyes have fixed-focus optics - the IOL cannot accommodate like the natural lens
- Patients typically need reading glasses for near vision (unless a multifocal or accommodating IOL was used)
- Visual symptoms include glare and halos around lights (especially around bright lights at night), even without complications, due to the optics of the IOL
Clinical Associations and Complications
1. Posterior Capsule Opacification (PCO) - "Secondary Cataract"
The most common late complication. Residual lens epithelial cells proliferate on the posterior capsule, causing visual blurring. Treatment is Nd:YAG laser capsulotomy, which creates a central opening in the cloudy capsule. - Textbook of Family Medicine, 9th ed.
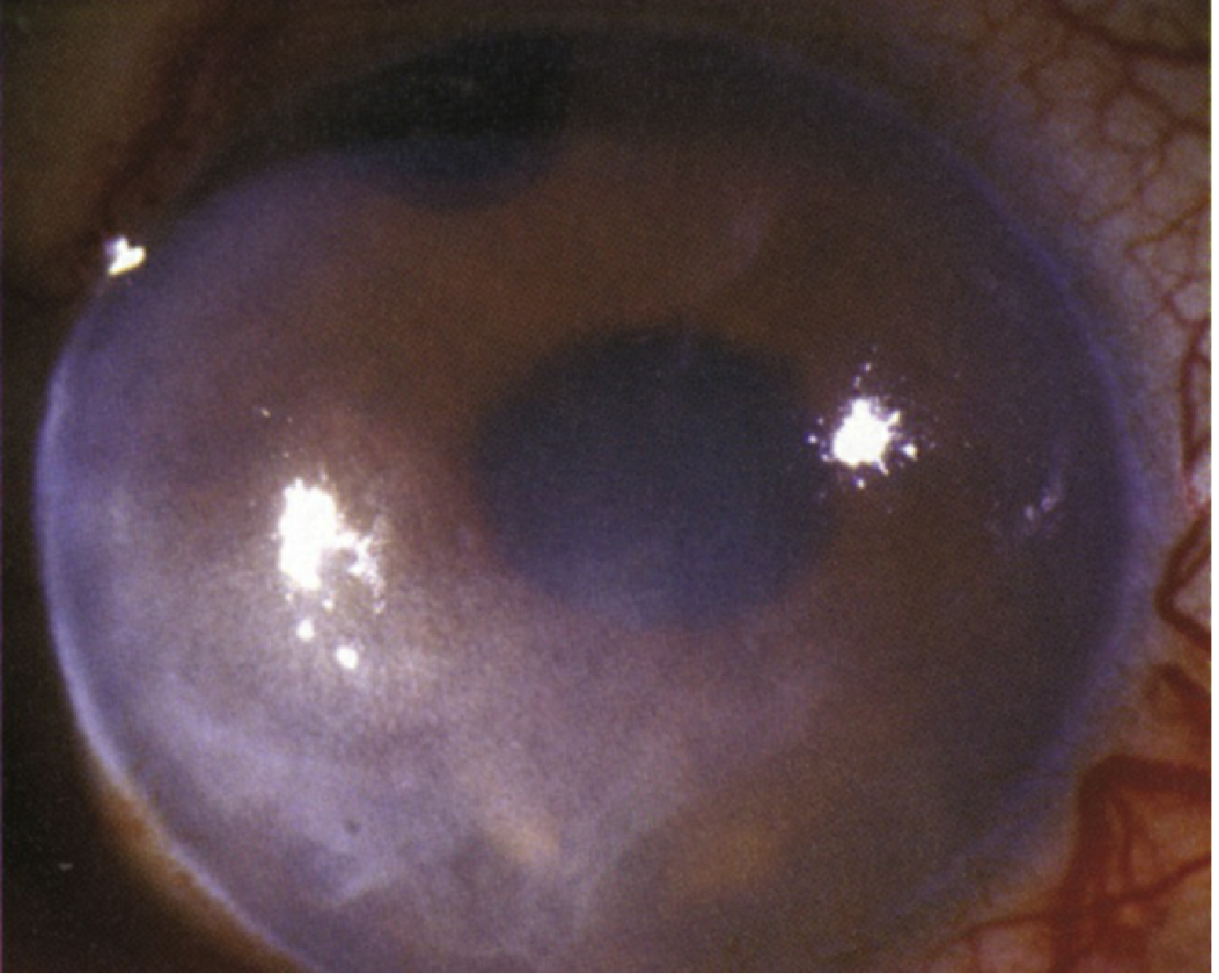
2. Pseudophakic Bullous Keratopathy (PBK)
A serious corneal complication:
- Symptoms: Decreased vision, pain, tearing, foreign body sensation, photophobia, redness
- Signs: Corneal edema in an eye from which the native lens has been removed; corneal bullae, Descemet folds, subepithelial haze/scarring, corneal neovascularization; cystoid macular edema (CME) may coexist
- Etiology: Multifactorial - corneal endothelial damage, intraocular inflammation, vitreous or subluxed IOL or tube shunt touching the cornea, preexisting endothelial dysfunction, glaucoma
- Treatment:
- Topical sodium chloride 5% drops QID + ointment at bedtime for epithelial edema
- IOP reduction (avoid epinephrine derivatives and prostaglandins if CME is present)
- Ruptured epithelial bullae: topical antibiotic + cycloplegic; bandage contact lens; anterior stromal micropuncture or excimer laser PTK for recurrent cases
- Advanced disease: full-thickness corneal transplant or endothelial keratoplasty (DMEK or DSEK), possibly with IOL repositioning/replacement and/or vitrectomy
- Follow-up: Every 1-3 days if ruptured bullae until healed; otherwise every 1-6 months depending on symptoms
- Wills Eye Manual; Robbins & Cotran Pathologic Basis of Disease
PBK and Fuchs endothelial dystrophy are the two leading indications for corneal transplantation - they share the same final common pathway of corneal edema. - Robbins & Kumar Basic Pathology
3. Retinal Detachment Risk
Pseudophakia is a recognized predisposing condition for retinal breaks and detachment, listed alongside high myopia, lattice degeneration, aphakia, and family history. The mechanism relates to altered vitreous dynamics after lens removal and the increased mobility of the vitreous. - Wills Eye Manual
4. Glare and Halos
Pseudophakia can cause:
- Glare (along with cataract, posterior capsular opacity, corneal edema, pharmacologic dilation, altered pupillary structure, and post-refractive surgery status)
- Halos around lights (along with posterior capsular opacity, corneal edema from any cause)
- Wills Eye Manual
5. CME Note
CME is less likely with posterior chamber or open-loop anterior chamber IOLs than with closed-loop anterior chamber IOLs (which are no longer used). - Wills Eye Manual
Summary Table
| Feature | Details |
|---|---|
| Definition | Eye with artificial IOL replacing native lens |
| Common cause | Cataract surgery (phacoemulsification) |
| IOL position | Posterior chamber (usual), anterior chamber, sulcus |
| Angle | Wide (Grade 4 gonioscopy) |
| Late complication | Posterior capsule opacification (PCO) - Rx: YAG laser |
| Corneal complication | Pseudophakic bullous keratopathy (PBK) |
| Retina risk | Increased risk of retinal break/detachment |
| Visual symptoms | Glare, halos, fixed focus (no accommodation) |
| vs. Aphakia | Aphakia = no lens at all; pseudophakia = IOL present |
This is a shared conversation. Sign in to Orris to start your own chat.