Basal gangliea physilogy mbbs long questiin
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content. Let me compile the complete MBBS long question answer on Basal Ganglia Physiology.
Basal Ganglia - Physiology (MBBS Long Question)
Sources: Ganong's Review of Medical Physiology 26th Ed, Costanzo Physiology 7th Ed, Kandel's Principles of Neural Science 6th Ed
1. Introduction
The basal ganglia (also called basal nuclei) are a group of deep subcortical nuclei that play a central role in the control of voluntary movement, motor planning, procedural learning, and certain cognitive and limbic functions. They act as a "gating system" - facilitating desired movements while suppressing unwanted ones.
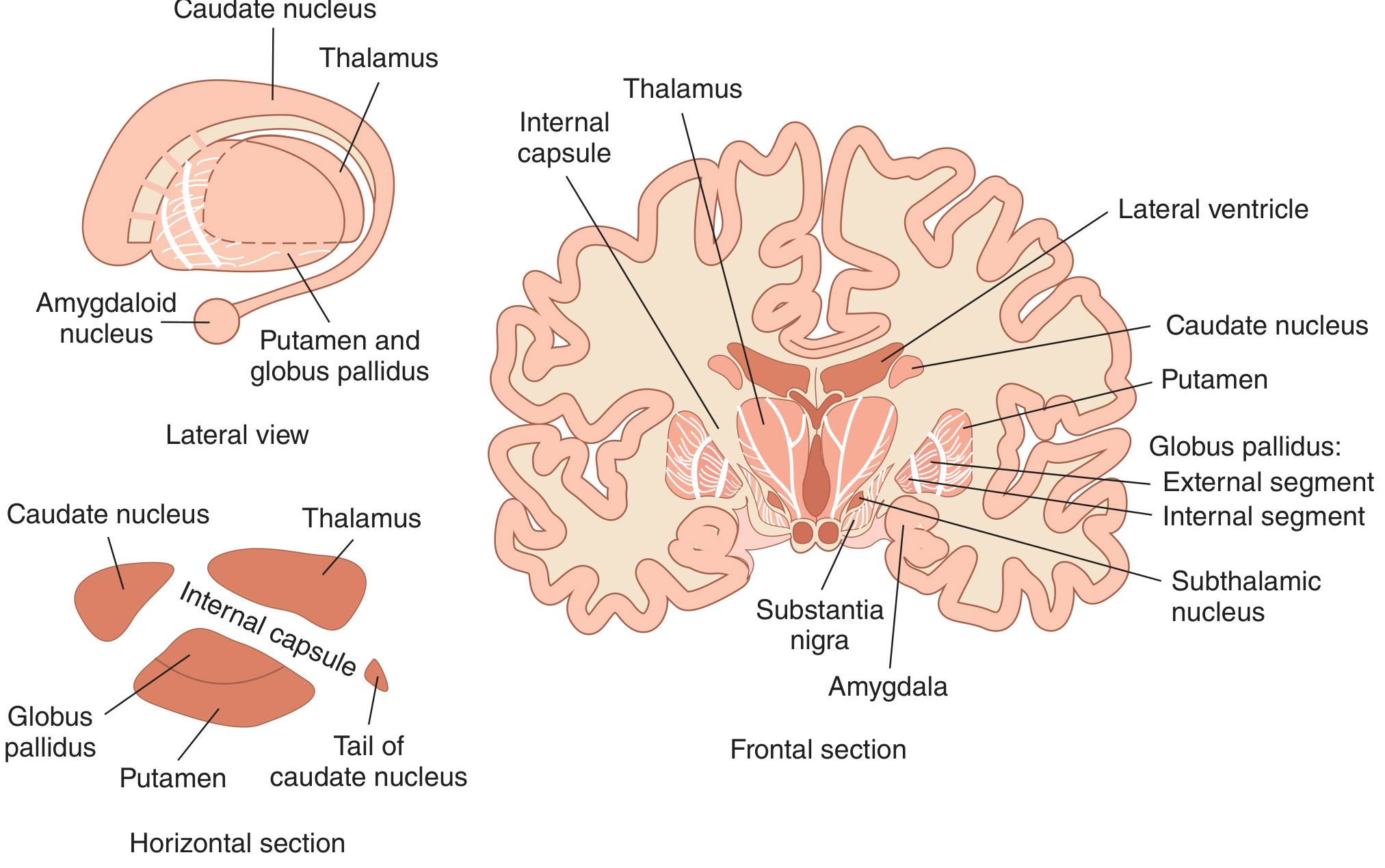
2. Components / Anatomy
The basal ganglia consist of 5 interactive structures on each side:
| Structure | Division | Notes |
|---|---|---|
| Caudate nucleus | Striatum | C-shaped; wraps around thalamus |
| Putamen | Striatum + Lenticular nucleus | Largest nucleus; receives motor cortex input |
| Globus pallidus (GP) | Lenticular nucleus | Divided into GPe (external) and GPi (internal) |
| Subthalamic nucleus (STN) | Diencephalon | Key modulator; only excitatory output |
| Substantia nigra (SN) | Midbrain | SNpc (pars compacta) and SNpr (pars reticulata) |
Key groupings:
- Striatum = Caudate + Putamen (main input nucleus)
- Lenticular nucleus = Putamen + Globus pallidus
- Corpus striatum = Caudate + Lenticular nucleus
3. Neurotransmitters
| Structure | Neurotransmitter |
|---|---|
| Striatum (95% medium spiny neurons) | GABA (inhibitory) |
| Striatum interneurons (large aspiny) | Acetylcholine |
| Striatum interneurons (medium aspiny) | Somatostatin |
| GPe and GPi | GABA (inhibitory) |
| SNpr | GABA (inhibitory) |
| SNpc | Dopamine |
| Subthalamic nucleus | Glutamate (excitatory) |
| Cortex → Striatum input | Glutamate (excitatory) |
4. Inputs and Outputs
Inputs to Basal Ganglia (both excitatory/glutamatergic, both to striatum):
- Corticostriate pathway - from wide areas of cerebral cortex (most importantly motor cortex)
- Thalamostriatal pathway - from intralaminar nuclei of thalamus
Outputs of Basal Ganglia (both inhibitory/GABAergic, both to thalamus):
- From GPi (internal globus pallidus)
- From SNpr (substantia nigra pars reticulata)
The thalamus then sends excitatory (glutamatergic) fibers back to the prefrontal and premotor cortex, completing the cortico-basal ganglia-thalamo-cortical loop.
5. Internal Circuitry - Direct and Indirect Pathways
The key concept is that basal ganglia output is tonically inhibitory to the thalamus. Movements occur when this inhibition is reduced (disinhibition).
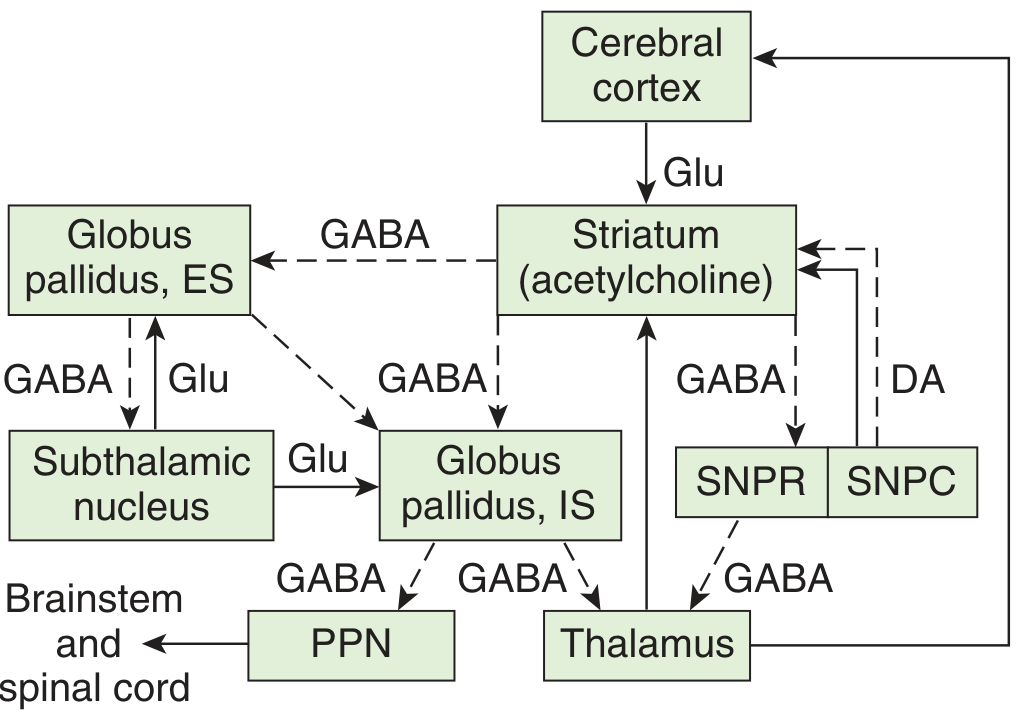
A. Direct Pathway (excitatory net effect on cortex - facilitates movement)
Cortex --[Glu]-→ Striatum --[GABA]-→ GPi/SNpr --[GABA]-→ Thalamus --[Glu]-→ Cortex
- Cortex excites striatum
- Striatum inhibits GPi/SNpr (reduces tonic inhibition - disinhibition)
- Thalamus is now released from inhibition → excites cortex
- Net effect: facilitates and increases motor cortex activity
B. Indirect Pathway (inhibitory net effect on cortex - suppresses movement)
Cortex --[Glu]-→ Striatum --[GABA]-→ GPe --[GABA]-→ STN --[Glu]-→ GPi/SNpr --[GABA]-→ Thalamus --[Glu]-→ Cortex
- Cortex excites striatum
- Striatum inhibits GPe
- GPe normally inhibits STN - so now STN is released (disinhibited)
- STN excites GPi/SNpr → increased tonic inhibition on thalamus
- Thalamus sends less excitatory output to cortex
- Net effect: suppresses motor cortex activity
Key principle: Direct and indirect pathways have opposite effects that are precisely balanced. This allows the basal ganglia to select desired movements and suppress competing movements simultaneously.
6. Role of Dopamine (Nigrostriatal Pathway)
The SNpc sends dopaminergic fibers to the striatum. Dopamine has dual opposing effects depending on which receptor it binds:
| Receptor | Pathway | Effect of Dopamine | Net Effect |
|---|---|---|---|
| D1 receptors | Direct pathway | Excites striatum → inhibits GPi → disinhibits thalamus | Facilitates movement |
| D2 receptors | Indirect pathway | Inhibits striatum → less inhibition of GPe → GPe inhibits STN → less excitation of GPi → less thalamic inhibition | Facilitates movement |
Therefore, dopamine facilitates movement via both pathways - it simultaneously amplifies the direct pathway (D1) and dampens the indirect pathway (D2).
7. Functions of Basal Ganglia
- Planning and programming of voluntary movements - discharge before movements begin
- Conversion of abstract thought to voluntary action - cognitive-to-motor transformation
- Selection of appropriate movements and suppression of competing/unwanted movements
- Procedural/habit learning - learning motor sequences (basal ganglia-dependent memory)
- Cognitive functions - caudate nucleus is involved in object reversal, delayed alternation; left caudate lesions cause dysarthric aphasia
- Affective and emotional modulation - via limbic loop connections
- Regulation of muscle tone - via output to brainstem and spinal cord (GPi → PPN → brainstem)
8. Diseases of the Basal Ganglia
Three biochemical systems normally operate in balance:
- Nigrostriatal dopaminergic system
- Intrastriatal cholinergic system
- GABAergic system (striatum → GP/SN)
Dysfunction of one or more systems leads to hyperkinetic or hypokinetic disorders.
Types of Movement Disorders:
| Type | Disorder | Characteristics |
|---|---|---|
| Hypokinetic | Akinesia | Difficulty initiating movement |
| Hypokinetic | Bradykinesia | Slowness of movement |
| Hyperkinetic | Chorea | Rapid, involuntary "dancing" movements |
| Hyperkinetic | Athetosis | Continuous, slow writhing movements |
| Hyperkinetic | Ballism | Involuntary flailing, violent limb movements |
A. Parkinson's Disease
Pathology: Degeneration of dopaminergic neurons in SNpc (pars compacta) - fibers to putamen most severely affected.
Mechanism:
- Loss of dopamine → D1 stimulation lost (direct pathway weakened) + D2 inhibition lost (indirect pathway over-active)
- GPi/SNpr become over-inhibited → excessive inhibition of thalamus → reduced cortical activation
- Result: hypokinesia (reduced movement initiation)
Features:
- Resting tremor (disappears with activity) - 4-6 Hz, "pill-rolling" tremor
- Bradykinesia - slowness, reduced spontaneous movements
- Rigidity - lead pipe rigidity; cogwheel rigidity (series of catches)
- Postural instability - shuffling gait, festination
Treatment:
- L-DOPA (dopamine precursor) - restores dopamine levels
- Dopamine agonists (bromocriptine, pramipexole)
- Anticholinergics (to restore dopamine-ACh balance)
B. Huntington's Disease
Pathology: Autosomal dominant; CAG trinucleotide repeat expansion in huntingtin gene (chromosome 4). Destroys medium spiny GABAergic neurons in the striatum (especially caudate first), and cholinergic neurons.
Mechanism:
- Loss of GABAergic neurons in striatum → GPe loses inhibition → GPe over-active → STN inhibited → GPi under-active → thalamus disinhibited → cortex over-activated
- Result: hyperkinesia (excessive movements)
Features:
- Early: jerky hand trajectory during reaching
- Later: choreiform movements (involuntary, rapid, dance-like)
- Progressive dementia
- Slurred speech, then incomprehensible speech
- Death in 10-15 years after onset
C. Hemiballismus
Pathology: Lesion (usually infarct or hemorrhage) of subthalamic nucleus (STN) - most often on one side.
Mechanism:
- STN lesion → STN cannot excite GPi
- GPi becomes under-active → thalamus disinhibited → cortex over-stimulated on opposite side
- Result: contralateral ballismus (violent flinging movements of the limbs)
9. Summary Comparison Table
| Feature | Parkinson's Disease | Huntington's Disease | Hemiballismus |
|---|---|---|---|
| Lesion | SNpc | Striatum (caudate > putamen) | Subthalamic nucleus |
| Lost neurotransmitter | Dopamine | GABA, ACh | Glutamate (STN output) |
| Movement type | Hypokinetic + some hyperkinetic | Hyperkinetic (chorea) | Hyperkinetic (ballism) |
| GPi activity | Increased (over-inhibits thalamus) | Decreased (thalamus disinhibited) | Decreased (thalamus disinhibited) |
| Genetics | Mostly sporadic (SNCA, LRRK2 in familial) | Autosomal dominant, CAG repeat | Usually vascular |
| Treatment | L-DOPA, dopamine agonists | Symptomatic (tetrabenazine) | Haloperidol; often resolves |
10. Key Points for Exam
- The striatum is the input nucleus; GPi and SNpr are the output nuclei
- Direct pathway = excitatory net effect on cortex (facilitates movement)
- Indirect pathway = inhibitory net effect on cortex (suppresses movement)
- Dopamine facilitates movement via D1 (direct) and D2 (indirect)
- Parkinson = too much GPi inhibition on thalamus (hypokinetic)
- Huntington = too little GPi inhibition on thalamus (hyperkinetic)
- Hemiballismus = STN lesion → contralateral violent movements
- Basal ganglia also mediate cognitive, limbic, and procedural learning functions (not just motor)
- Ganong's Review of Medical Physiology, 26th Ed., Ch. 12 | Costanzo Physiology, 7th Ed., Ch. 3 | Kandel's Principles of Neural Science, 6th Ed., Ch. 43
This is a shared conversation. Sign in to Orris to start your own chat.