Ear anatomy for exam point of view
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive material. Let me compile a thorough, exam-focused answer.
Ear Anatomy - Exam Guide
Here is a structured, high-yield breakdown of ear anatomy from authoritative sources (Cummings Otolaryngology, KJ Lee's Essential Otolaryngology, Costanzo Physiology, Gray's Anatomy).
Overview: Three Divisions
The ear divides into external ear, middle ear, and inner ear. All three housed within the temporal bone, which has four parts: squamous, mastoid, petrous, and tympanic.
1. Temporal Bone - High Yield Facts
| Part | Key Features |
|---|---|
| Squamous | Forms lateral middle fossa floor; temporal line ~5 mm inferior to middle fossa floor |
| Mastoid | Contains mastoid antrum; MacEwen triangle (cribriform area) marks it; SCM pulls mastoid tip inferiorly |
| Petrous | Contains inner ear structures; arcuate eminence = prominence of superior SCC on middle fossa floor |
| Tympanic | Forms floor and anterior wall of external auditory canal |
- Temporal bone articulates with sphenoid, parietal, occipital, and zygomatic bones
- Stylomastoid foramen = anterior limit of digastric groove (where facial nerve exits)
- Mastoid antrum = largest mastoid air cell; located deep to MacEwen triangle
2. External Ear
Auricle
- Composed of elastic fibrocartilage (except lobule = fat only)
- Sensory supply: Great auricular nerve (C2/C3), Auriculotemporal nerve (V3), Arnold's nerve (CN X branch - important in ear-cough reflex)
External Auditory Canal (EAC)
- Outer 1/3 - cartilaginous (skin has hair follicles + ceruminous glands; fissures of Santorini allow infection spread)
- Inner 2/3 - bony (skin is thin, no adnexa; directly on bone)
- Total length ~24 mm
- Foramen of Huschke - potential defect in bony EAC (tumor spread pathway)
- Bony-cartilaginous junction - narrowest point; pathway for tumor spread
Blood Supply of EAC
- Posterior auricular artery, deep auricular artery (from maxillary artery), superficial temporal artery
3. Tympanic Membrane (TM)
Layers (4 layers - classic exam question)
- Lateral - squamous epithelium (continuous with EAC skin)
- Radiate fibrous layer (outer fibrous)
- Circular fibrous layer (inner fibrous)
- Medial - mucosal layer (middle ear mucosa)
The annular ligament anchors TM peripherally to the tympanic sulcus (bony ring).
Two Parts
| Region | Features |
|---|---|
| Pars tensa | Lower 4/5; 4-layer; attached to annulus; site of most perforations |
| Pars flaccida (Shrapnell membrane) | Upper 1/5; 2-layer (no fibrous); superior to anterior/posterior mallear folds; site of cholesteatoma origin |
Surface Landmarks (otoscopy)
- Umbo = tip of malleus handle (most depressed central point)
- Mallear stria = handle visible through TM
- Lateral process = most prominent point at upper end of handle
- Cone of light = seen anteroinferiorly (5 o'clock right ear, 7 o'clock left ear)
- Anterior and posterior mallear folds = define upper limit of pars tensa
Dimensions
- Total area: 70-80 mm²
- Effective vibrating area: ~55 mm²
Prussak Space (important for cholesteatoma)
- Anterior: lateral malleal fold
- Posterior: lateral malleal fold
- Superior: lateral malleal fold
- Inferior: lateral process of malleus
- Medial: neck of malleus
- Lateral: Shrapnell membrane
4. Middle Ear
Divisions (relative to tympanic annulus)
| Division | Location |
|---|---|
| Hypotympanum | Below level of TM |
| Mesotympanum | Level of TM; contains most ossicles |
| Epitympanum (attic) | Above TM; contains head of malleus + body of incus |
| Mastoid antrum | Posterior extension |
Ossicles - Embryology (Very High Yield)
| Ossicle | Branchial Arch Origin |
|---|---|
| Head of malleus, body + short process of incus | 1st arch (Meckel's cartilage) |
| Manubrium of malleus, long process of incus, stapes superstructure | 2nd arch (Reichert's cartilage) |
| Stapes footplate | Otic capsule (not branchial arch) |
Ossicles are adult size at birth - formed by 8 weeks gestation.
Ossicle Parts
Malleus: Head → Neck → Manubrium (handle) → Anterior process + Lateral process
Incus: Body → Short process → Long process → Lenticular process (articulates with stapes)
Stapes: Head → Neck → Anterior crus + Posterior crus → Footplate (1.41 × 2.99 mm)
Incus: Body → Short process → Long process → Lenticular process (articulates with stapes)
Stapes: Head → Neck → Anterior crus + Posterior crus → Footplate (1.41 × 2.99 mm)
Ossicular Joints
- Malleoincudal joint = diarthrodial
- Incudostapedial joint = diarthrodial
- Stapediovestibular (labyrinthine) joint = syndesmotic (annular ligament)
Most Vulnerable Part of Ossicular Chain
Long process of the incus - single nutrient vessel, no collateral circulation; most commonly eroded in chronic otitis media.
Middle Ear Muscles
| Muscle | Nerve Supply | Action |
|---|---|---|
| Tensor tympani | CN V3 (medial pterygoid nerve) | Pulls malleus medially, tenses TM |
| Stapedius | CN VII (facial nerve) | Pulls stapes posteriorly, dampens loud sounds (acoustic reflex) |
Stapedius = smallest muscle in the body. Paralysis in Bell's palsy causes hyperacusis.
Eustachian Tube (ET)
- Connects middle ear to nasopharynx
- Angle: ~45° from horizontal in adults (more horizontal in children - explains frequent OM in children)
- Proximal 1/3: bony; distal 2/3: fibrocartilaginous (collapsed at rest)
- Opens during swallowing/yawning via tensor veli palatini (CN V3)
- Bony-cartilaginous junction = narrowest point
Important Middle Ear Relations
- Roof (tegmen tympani) - separates middle ear from middle fossa
- Floor - jugular bulb below
- Anterior wall - internal carotid artery (may be dehiscent)
- Posterior wall - facial nerve, aditus ad antrum
- Medial wall - promontory (cochlear basal turn), oval window, round window, facial nerve canal
Windows
- Oval window - accepts stapes footplate; lies in sagittal plane; transmits vibrations to scala vestibuli
- Round window - covered by secondary tympanic membrane; allows pressure relief
5. Facial Nerve in the Temporal Bone
The facial nerve traverses the fallopian canal with three segments:
| Segment | Details | Clinical Relevance |
|---|---|---|
| Labyrinthine | Shortest, narrowest; from fundus IAC to geniculate ganglion | Most vulnerable to swelling (herpes zoster/Ramsay Hunt) |
| Tympanic (horizontal) | Above oval window; most often dehiscent | Injured in cholesteatoma surgery |
| Mastoid (vertical) | From 2nd genu to stylomastoid foramen | Exits at stylomastoid foramen |
- Geniculate ganglion: gives off Greater Superficial Petrosal Nerve (GSPN) → lacrimal gland
- Chorda tympani: branches from mastoid segment → taste ant. 2/3 tongue, submandibular/sublingual glands
6. Inner Ear
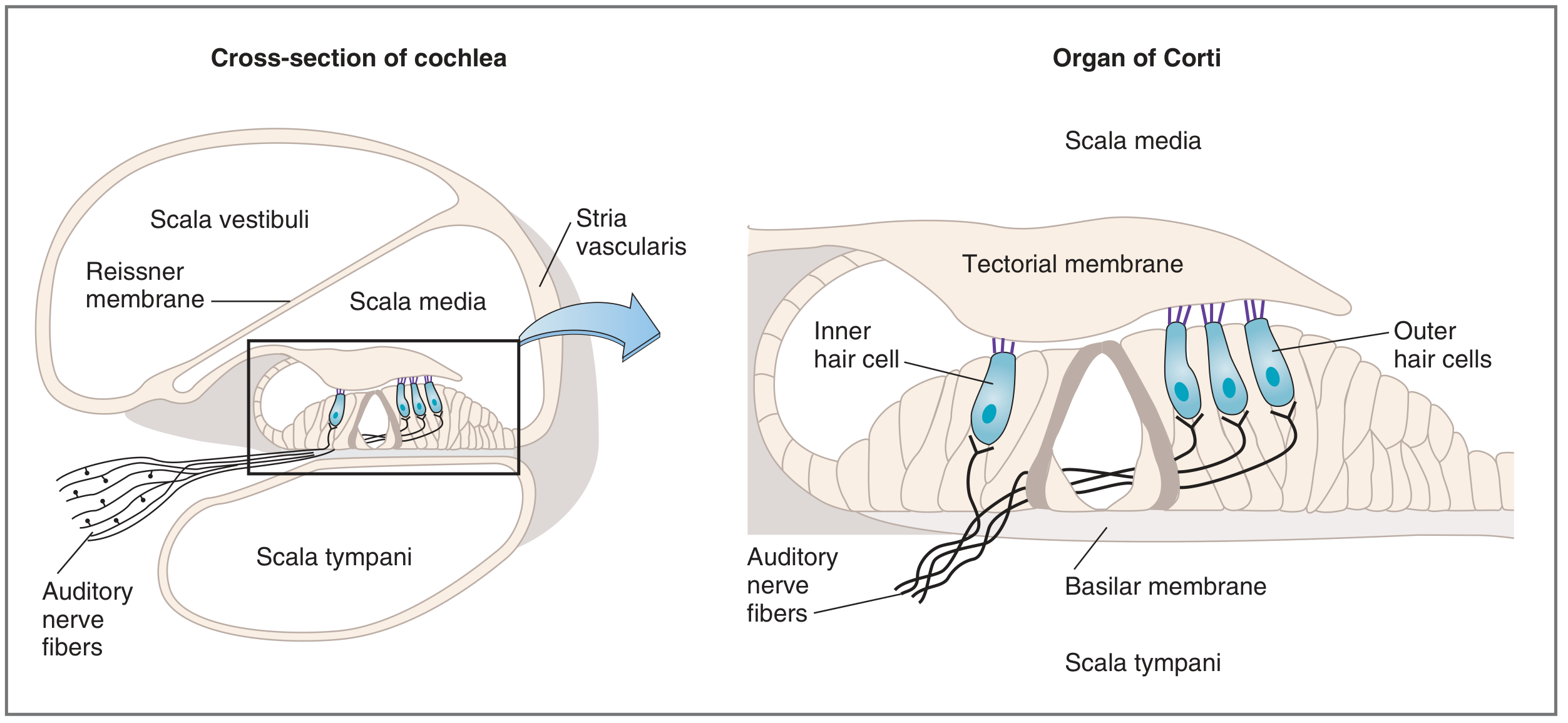
Cochlea - Three Scalae
| Chamber | Fluid | Boundaries |
|---|---|---|
| Scala vestibuli | Perilymph | Communicates with oval window |
| Scala media (cochlear duct) | Endolymph | Between Reissner's and basilar membranes |
| Scala tympani | Perilymph | Communicates with round window |
- Scala vestibuli and tympani communicate at the apex via helicotrema
- Reissner's membrane separates scala vestibuli from scala media
- Basilar membrane separates scala media from scala tympani
- Stria vascularis produces endolymph (high K+, low Na+)
Organ of Corti (on basilar membrane)
- Contains inner hair cells (1 row, ~3500) and outer hair cells (3 rows, ~12,000)
- Hair cells (cilia) embedded in tectorial membrane
- Inner hair cells = primary auditory transducers (90% of afferent fibers)
- Outer hair cells = amplifiers (active motility, otoacoustic emissions)
- Cell bodies in spiral ganglion → cochlear nerve → CN VIII
Tonotopy (Exam Favorite)
- Base of cochlea = high frequency (20,000 Hz)
- Apex of cochlea = low frequency (20 Hz)
Vestibular Apparatus
- 3 semicircular canals (superior/anterior, posterior, horizontal/lateral) - detect angular acceleration
- Utricle - macula oriented horizontally; detects linear acceleration and head tilt
- Saccule - macula oriented vertically; detects vertical linear acceleration
Fluids
- Perilymph - similar to CSF (high Na+, low K+); in scala vestibuli and tympani
- Endolymph - similar to intracellular fluid (high K+ ~150 mM, low Na+); in scala media; produced by stria vascularis
- Endolymphatic hydrops = excessive endolymph → Meniere's disease
7. Embryology Summary
| Structure | Origin |
|---|---|
| Auricle | 1st and 2nd branchial arch hillocks (6 hillocks of His) |
| EAC | 1st branchial groove |
| Middle ear cavity, ET | 1st pharyngeal pouch (tubotympanic recess) |
| Malleus head, incus body/short process | 1st arch (Meckel's) |
| Malleus handle, incus long process, stapes superstructure | 2nd arch (Reichert's) |
| Stapes footplate | Otic capsule |
| Inner ear (cochlea, vestibule, SCCs) | Otic vesicle (otocyst) from ectoderm |
- Mastoid antrum appears at 21 weeks gestation
- Mastoid tip poorly developed at birth → facial nerve more superficial and prone to surgical injury in neonates
- Eustachian tube doubles in length from birth to adulthood
8. Blood Supply
- EAC: Posterior auricular + superficial temporal arteries (external ear); deep auricular artery (bony EAC)
- Middle ear: Anterior tympanic (from maxillary), inferior tympanic (from ascending pharyngeal), superior tympanic (from middle meningeal), stylomastoid (from posterior auricular)
- Inner ear: Labyrinthine artery (from AICA or basilar artery) - end artery, no collaterals → labyrinthine infarction is devastating
9. Nerve Supply Summary (Exam High Yield)
| Region | Nerves |
|---|---|
| Auricle outer surface | Auriculotemporal (V3), greater auricular (C2/C3), lesser occipital (C2), Arnold's nerve (CN X) |
| EAC skin | Arnold's nerve (CN X) - stimulation causes ear-cough reflex + vagal syncope |
| Middle ear mucosa | Jacobson's nerve (CN IX, tympanic branch) → tympanic plexus |
| Stapedius | CN VII |
| Tensor tympani | CN V3 |
| Cochlea (afferent) | CN VIII (cochlear division), spiral ganglion |
| Vestibule (afferent) | CN VIII (vestibular division), Scarpa's ganglion |
10. High-Yield Exam Quick-Recall
| Fact | Answer |
|---|---|
| Smallest bone in body | Stapes |
| Smallest muscle in body | Stapedius |
| Most vulnerable ossicle to erosion | Long process of incus |
| Pars flaccida is also called | Shrapnell membrane |
| Cholesteatoma originates from | Pars flaccida |
| Scala with endolymph | Scala media |
| Endolymph produced by | Stria vascularis |
| High K+ fluid in ear | Endolymph |
| Prussak space - lateral wall | Shrapnell membrane |
| ET opened by | Tensor veli palatini (CN V3) |
| Hyperacusis in Bell's palsy - due to | Stapedius paralysis |
| Arnold's nerve stimulation causes | Ear-cough reflex, vagal syncope |
| Facial nerve most dehiscent in | Tympanic (horizontal) segment above oval window |
| Arcuate eminence = prominence of | Superior semicircular canal |
| Helicotrema connects | Scala vestibuli and scala tympani at cochlear apex |
| Base vs apex of cochlea - frequency | Base = high freq; Apex = low freq |
Sources: Cummings Otolaryngology Head and Neck Surgery, Ch. 126 | KJ Lee's Essential Otolaryngology | Costanzo Physiology 7th Ed, Ch. 3 | Langman's Medical Embryology
This is a shared conversation. Sign in to Orris to start your own chat.