Approach to hyperkalemia
Reading File
Finding Sources
Searching PubMed
"hyperkalemia" AND "management"
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have all the key information needed for a comprehensive answer. Let me compile the full response.
Approach to Hyperkalemia
Definition and Severity
Hyperkalemia is defined as serum K⁺ ≥5.5 mmol/L, with significant (severe) hyperkalemia at ≥6.0-6.5 mmol/L. It is found in 1.1-10% of hospitalized patients and carries a mortality of 14-41% in severe cases - Brenner and Rector's The Kidney.
Severity classification:
- Mild: 5.5-6.0 mEq/L
- Moderate: 6.0-6.5 mEq/L
- Severe: >6.5 mEq/L (or any level with ECG changes)
Step 1 - Rule Out Pseudohyperkalemia
Before any workup, confirm the result is real. Pseudohyperkalemia occurs with:
- Prolonged tourniquet time or fist clenching during venipuncture
- Thrombocytosis, leukocytosis, or erythrocytosis (in vitro K⁺ release)
- Cooling of blood sample post-venipuncture
- Hereditary pseudohyperkalemia (SLC4A1 mutations causing red cell K⁺ leak)
- Acute anxiety causing respiratory alkalosis with redistribution
If suspected, repeat the sample as a plasma (heparinized) specimen rather than serum. - Harrison's Principles of Internal Medicine 22E
Step 2 - Identify the Cause
Mechanism-Based Classification
A. Increased K⁺ intake (rarely the sole cause unless excretion is impaired)
- Dietary excess, IV potassium supplementation, blood transfusions
B. Transcellular shift (K⁺ out of cells)
| Cause | Mechanism |
|---|---|
| Acidemia (non-anion gap metabolic, respiratory) | H⁺ enters cells, K⁺ exits |
| Insulin deficiency / DKA | Reduced Na⁺/K⁺-ATPase activity |
| Beta-blocker toxicity | Impaired Na⁺/K⁺-ATPase stimulation |
| Succinylcholine | Depolarizes muscle, K⁺ exits via ACh receptors |
| Digoxin overdose | Inhibits Na⁺/K⁺-ATPase in skeletal muscle |
| Hypertonic states (mannitol, hypertonic saline, hypertonic glucose) | Solvent drag effect |
| Fluoride poisoning | Inhibits Na⁺/K⁺-ATPase |
| Cationic amino acids (lysine, arginine, epsilon-aminocaproic acid) | Cation-K⁺ exchange |
| Tissue destruction (rhabdomyolysis, tumor lysis, hemolysis, burns) | Cell lysis releases K⁺ |
Note: Anion-gap acidoses (lactic acidosis, ketoacidosis) do NOT cause hyperkalemia via this mechanism - Harrison's 22E
C. Decreased renal excretion (most common mechanism)
- Acute kidney injury (AKI) or chronic kidney disease (CKD)
- Hypoaldosteronism:
- Primary: Addison disease, bilateral adrenalectomy, adrenal hemorrhage, heparin/LMWH-induced
- Hyporeninemic hypoaldosteronism (Type 4 RTA): diabetic nephropathy, NSAIDs, calcineurin inhibitors
- Drug-induced RAAS blockade: ACEi, ARBs, direct renin inhibitors, aliskiren
- Potassium-sparing diuretics: spironolactone, amiloride, triamterene
- Voltage-dependent defects in K⁺ secretion: obstructive uropathy, sickle cell disease
- Gordon syndrome (pseudohypoaldosteronism type II)
Step 3 - Clinical Features
Symptoms are often absent until hyperkalemia is severe. When present:
- Neuromuscular: weakness, fatigue, ascending paralysis, paresthesias
- Cardiac: palpitations, syncope, cardiac arrest (most dangerous manifestation)
- GI: nausea, vomiting (less specific)
Step 4 - ECG Changes (Sequential with Rising K⁺)
ECG changes may be absent even in severe hyperkalemia - a normal ECG does not exclude dangerous hyperkalemia. However, when present, they follow a rough sequence:
| Serum K⁺ | ECG Change |
|---|---|
| 5.5-6.5 mEq/L | Peaked (tall, narrow, symmetric) T waves - earliest sign |
| 6.5-7.5 mEq/L | PR prolongation, P wave flattening/disappearance |
| 7.0-8.0 mEq/L | QRS widening |
| >8.0 mEq/L | Sine wave pattern, VF, asystole |
- Rosen's Emergency Medicine
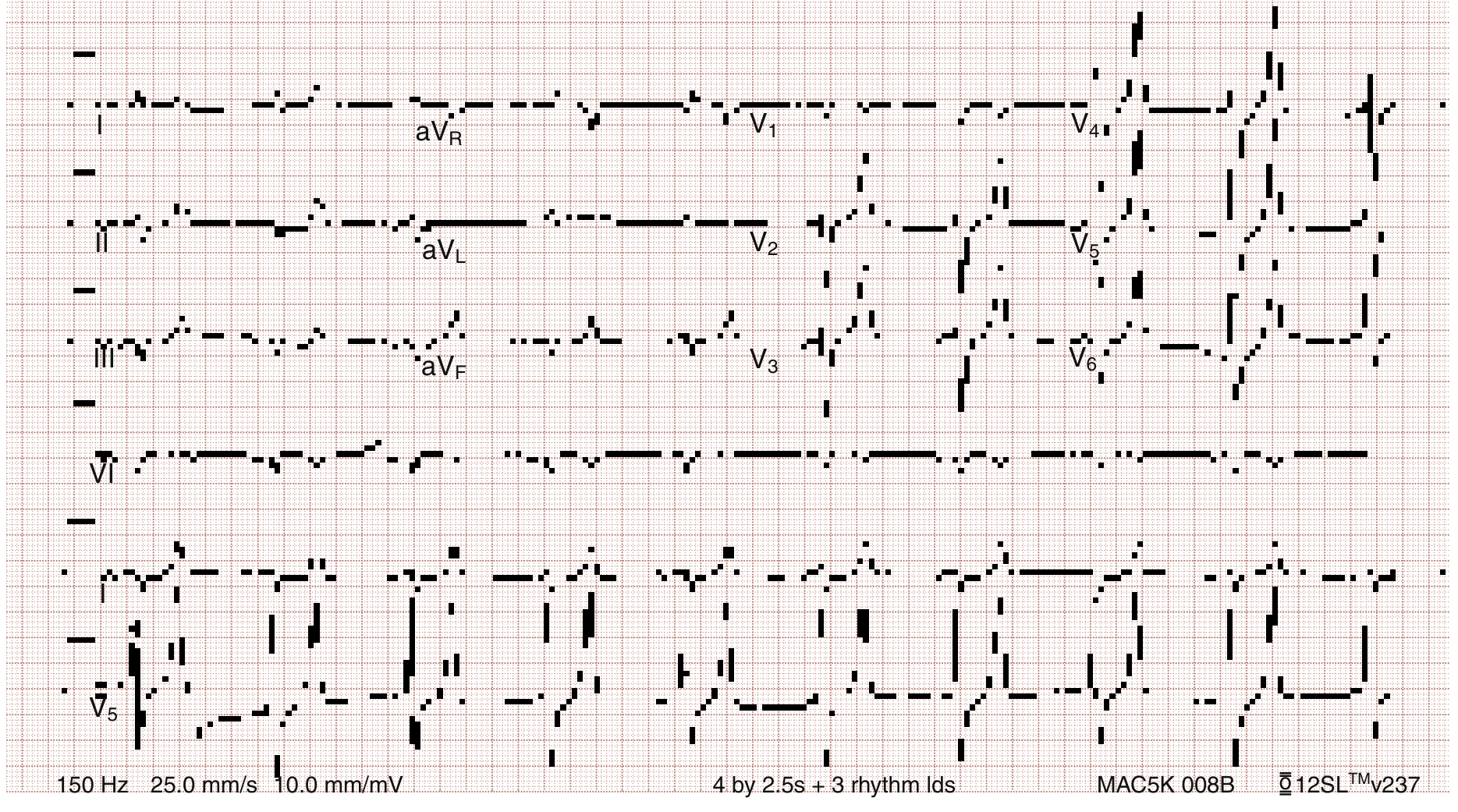
ECG: Severe hyperkalemia - QRS widening merging into T wave, absent P waves (pre-treatment):
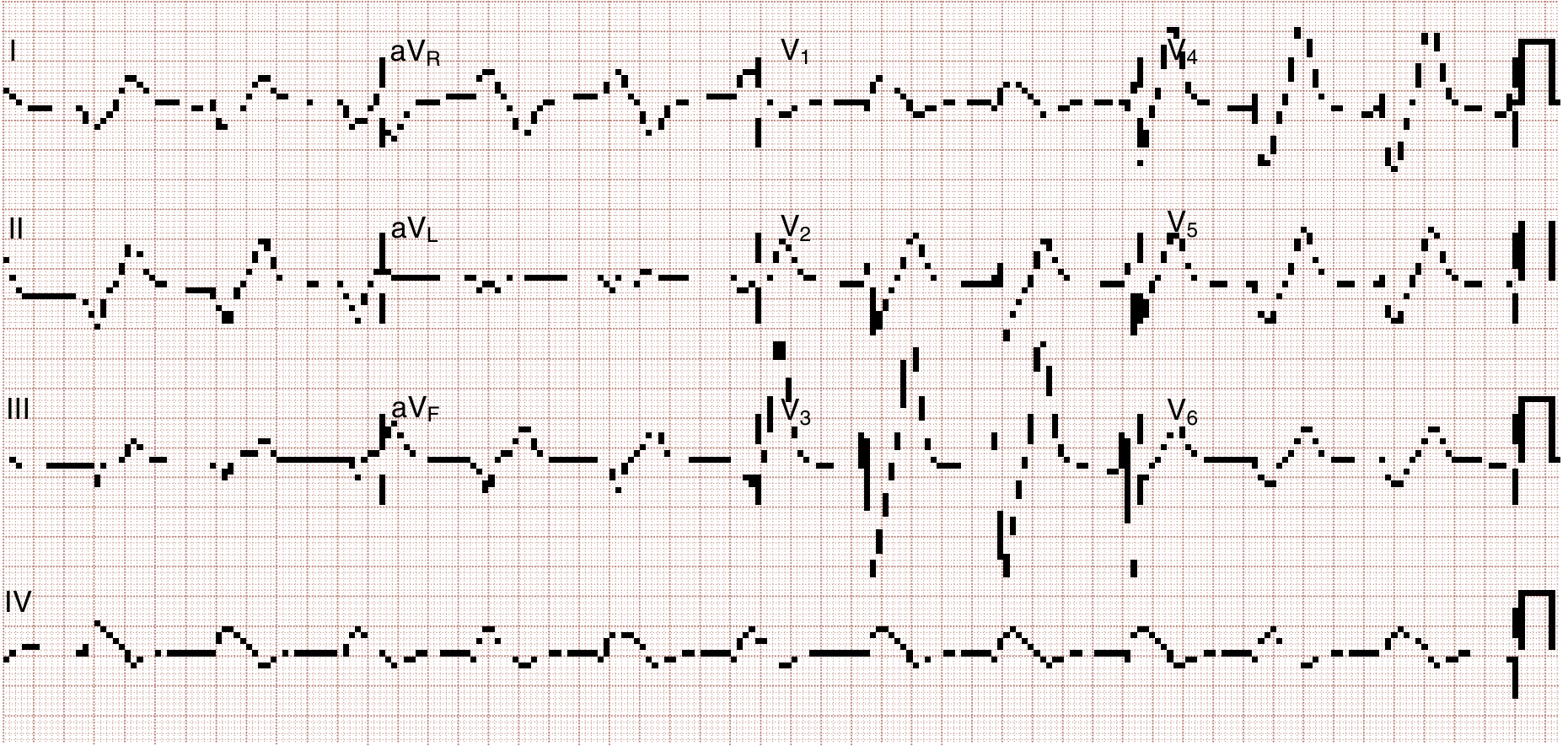
ECG: Same patient after initial treatment - tall peaked T waves, decreased P wave amplitude:
Hyperkalemia can also present as atropine-resistant bradycardia with or without apparent heart block - Rosen's Emergency Medicine
Step 5 - Diagnostic Workup
- Serum electrolytes, BUN/creatinine - assess renal function
- Glucose, insulin levels - diabetic causes
- Arterial/venous blood gas - acidemia
- Urine K⁺, urine creatinine, urine/serum osmolality
- Transtubular K⁺ gradient (TTKG):
TTKG = (U_K × Serum Osm) / (Serum K⁺ × Urine Osm)
- Normal response to hyperkalemia: TTKG >7-8 (appropriate renal excretion)
- TTKG <3-5 in hyperkalemia = impaired K⁺ secretion (aldosterone deficiency or resistance)
- Plasma aldosterone and renin - to distinguish primary from secondary hypoaldosteronism
- ECG - obtain immediately in any suspected hyperkalemia
Step 6 - Treatment
Treatment is organized into 3 simultaneous stages: - Harrison's 22E, Rosen's Emergency Medicine
Stage 1 - Stabilize the Cardiac Membrane (Immediate)
Indication: ECG changes (especially wide QRS), or K⁺ ≥6.5 mEq/L even without ECG changes
| Agent | Dose | Onset | Duration | Notes |
|---|---|---|---|---|
| Calcium gluconate 10% | 10 mL IV over 2-3 min | 1-3 min | 30-60 min | Preferred for peripheral IV access |
| Calcium chloride 10% | 3-4 mL (or 1g) IV | 1-3 min | 30-60 min | Preferred via central line (tissue necrosis if extravasates); 3x more calcium than gluconate |
- Calcium raises the action potential threshold, restoring the difference between resting and threshold potentials - does NOT lower K⁺
- Repeat dose if no ECG improvement or if improvement recurs
- Caution in digoxin toxicity: hypercalcemia potentiates digoxin cardiotoxicity; if necessary, dilute in 100 mL D5W and infuse over 20-30 min
Stage 2 - Shift K⁺ Into Cells (Rapid, Bridges to Removal)
| Agent | Dose | Onset | Effect | Notes |
|---|---|---|---|---|
| Regular insulin + glucose | 10 units IV + 50 mL D50W (25g glucose) | 10-20 min | Peak 30-60 min, lasts 4-6h; ↓K⁺ ~0.6 mEq/L | Follow with D10W infusion at 50-75 mL/h; monitor glucose closely. Reduce to 5 units if renal dysfunction. Omit glucose if blood glucose ≥200-250 mg/dL |
| Nebulized albuterol | 10-20 mg in 4 mL NS over 10 min (4x bronchodilator dose) | ~30 min | Peak ~90 min; ↓K⁺ 0.5-1 mEq/L | ~20% of ESRD patients are resistant; do NOT use alone without insulin |
| Insulin + albuterol combined | As above | -- | ↓K⁺ ~1.2 mEq/L (additive) | Preferred combination for maximum shift |
| Sodium bicarbonate | 150 mEq in 1L D5W IV infusion | 4-6 h | Modest, delayed | Only useful in metabolic acidosis; do NOT give as undiluted IV bolus (risk of hypernatremia/hypertonicity). No role in acute treatment |
| Normal saline | 100-250 mL IV | -- | Minor | Stimulates Na⁺/K⁺-ATPase; useful in hypovolemic patients; use cautiously in anuric patients |
Stage 3 - Remove K⁺ From the Body (Definitive)
| Method | Agent/Dose | Onset | Notes |
|---|---|---|---|
| Hemodialysis | -- | Rapid | Most effective and reliable; mandatory in cardiac arrest or refractory hyperkalemia; peritoneal dialysis considerably less effective |
| Loop diuretics | Furosemide IV | 30-60 min | Only with intact renal function; combine with saline or isotonic bicarbonate to maintain euvolemia |
| Sodium polystyrene sulfonate (SPS/Kayexalate) | 15-30 g in 33% sorbitol suspension PO/PR | Hours (full effect up to 24h) | Risk of intestinal necrosis (especially post-op, opioid use, reduced motility); avoid when possible |
| Patiromer | 8.4 g PO daily | Hours | Nonabsorbed polymer; exchanges K⁺ for Ca²⁺; side effect: hypomagnesemia; preferred over SPS |
| Sodium zirconium cyclosilicate (SZC) | 10 g PO TID x 48h (acute) | 1-2 h (faster onset than patiromer) | Exchanges Na⁺/H⁺ for K⁺ and NH₄⁺; preferred over SPS |
Patiromer and SZC have replaced SPS as preferred binders in most settings due to their lack of intestinal toxicity - Harrison's 22E. A 2025 systematic review (PMID 40542996) confirms novel potassium binders also allow optimization of RAAS inhibitor therapy in CKD and heart failure.
Summary Algorithm
Suspected Hyperkalemia
↓
1. Obtain ECG + serum K⁺ immediately
↓
ECG changes or K⁺ ≥6.5?
YES → IV Calcium IMMEDIATELY (membrane stabilization)
NO → Proceed to workup + shifts
↓
2. Shift K⁺ into cells:
Insulin 10U IV + D50W 50mL
+ Nebulized albuterol 10-20mg
↓
3. Remove K⁺ from body:
- Adequate urine output? → Furosemide ± saline
- Oral/enteral route available? → Patiromer or SZC
- AKI/ESRD or refractory? → Hemodialysis
↓
4. Find and treat the underlying cause
- Review medications (ACEi/ARB, NSAIDs, K-sparing diuretics)
- Check renal function, aldosterone/renin
- Dietary counseling
Special Considerations
- Succinylcholine is relatively contraindicated in pre-existing hyperkalemia, and absolutely contraindicated in patients with burns, neuromuscular disease, prolonged immobilization, or spinal cord injury (marked upregulation of ACh receptors causes massive K⁺ efflux)
- Digoxin toxicity co-existing with hyperkalemia: use calcium with extreme caution; diluted slow infusion preferred
- ACEi/ARBs causing hyperkalemia: with the availability of patiromer/SZC, these drugs can often be continued at reduced dose rather than discontinued - this is a shift in modern management
- ESRD patients: even modest potassium loads or common medications (beta-blockers, ACEi) can precipitate severe hyperkalemia; maintain low threshold for monitoring and treatment - Rosen's Emergency Medicine
Sources: Harrison's Principles of Internal Medicine 22E (2025); Rosen's Emergency Medicine; Brenner and Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.