Hypovolumic shock
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypovolemic shock" management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer on hypovolemic shock. Let me compile everything.
Hypovolemic Shock
Hypovolemic shock is the most common type of shock encountered in surgical and emergency practice. It occurs when intravascular volume falls to a level at which the heart can no longer maintain adequate cardiac output (CO) to meet the oxygen demands of vital organs.
Definition & Core Pathophysiology
Hypovolemic shock is defined by:
- Reduced CO due to decreased preload (low circulating volume)
- Elevated SVR (sympathetic compensatory vasoconstriction)
- Low CVP and PCWP (low filling pressures)
- Low mixed venous O2 saturation (SvO2)
Harrison's Principles of Internal Medicine 22E summarizes it: "Hypovolemic shock encompasses disease processes that reduce CO (and oxygen delivery) via a reduction in preload... characterized by an elevated SVR and low CVP and PCWP related to decreased intravascular volume."
Causes
Hemorrhagic (most common):
- External trauma
- Internal bleeding (upper/lower GI hemorrhage)
Non-hemorrhagic:
- GI losses: profuse vomiting, diarrhea
- Renal losses: osmotic diuresis (DKA, diabetes insipidus)
- Skin losses: severe burns, Stevens-Johnson syndrome
- Plasma sequestration: soft tissue injury, peritonitis, bowel obstruction
The essential threshold: loss of >20% of circulating volume is required to produce the full shock syndrome. Blood volume is estimated at ~7% of ideal body weight (~4,900 mL in a 70-kg adult).
Compensatory Mechanisms
When blood volume and arterial pressure fall, three major systems are activated:
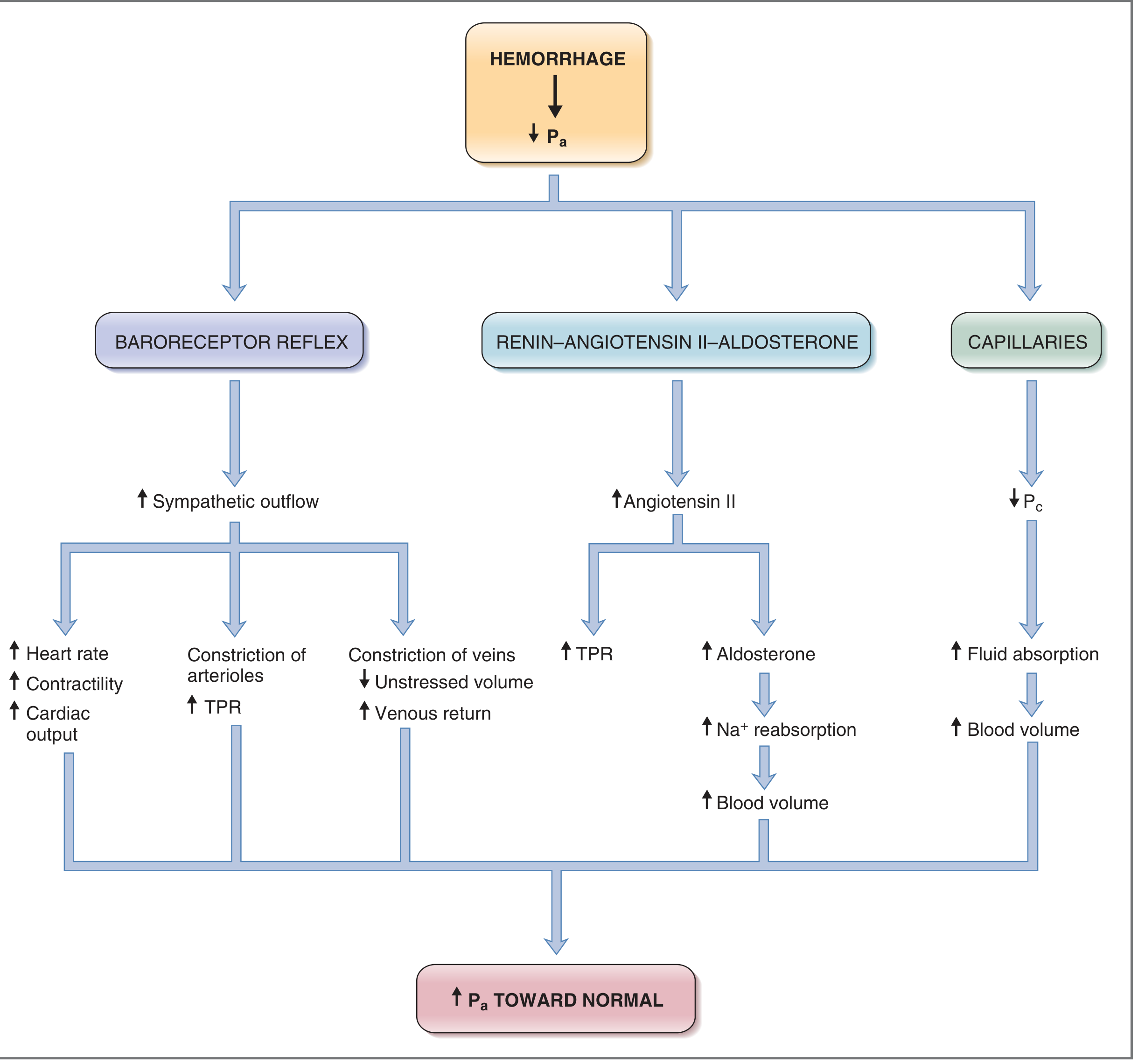
1. Baroreceptor Reflex (immediate):
- Increased sympathetic outflow
- Tachycardia + increased contractility
- Arteriolar constriction → increased TPR
- Venous constriction → increased venous return
2. Renin-Angiotensin-Aldosterone System:
- Angiotensin II raises TPR
- Aldosterone promotes Na+ retention → restores blood volume
3. Capillary Fluid Shift:
- Decreased capillary hydrostatic pressure draws interstitial fluid into vasculature, restoring volume
Key point: Sympathetic reflexes preferentially maintain arterial pressure over cardiac output - CO falls first, BP falls later. Cardiac and cerebral blood flows are protected until MAP falls below ~70 mmHg.
Effect of Blood Loss on Hemodynamics
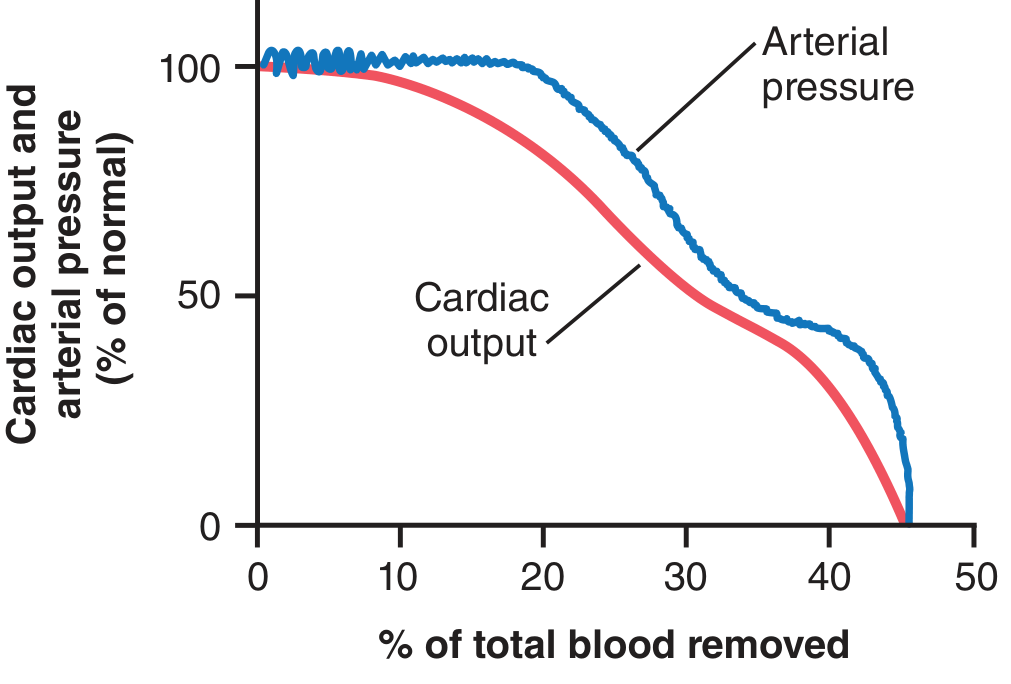
- Up to ~10% blood loss: minimal change in BP or CO
- 20-30%: CO begins to fall significantly; BP partially maintained by reflexes
- 40-45%: Both CO and BP fall to zero - lethal without intervention
ATLS Classification (Hemorrhagic Shock)
| Class | Blood Loss | Volume (70-kg adult) | HR | BP | Pulse Pressure | Urine Output | Mental Status |
|---|---|---|---|---|---|---|---|
| I | <15% | <750 mL | Normal | Normal | Normal | >30 mL/hr | Normal |
| II | 15-30% | 750-1,500 mL | >100 | Slightly ↓ | Narrowed | 20-30 mL/hr | Anxious |
| III | 30-40% | 1,500-2,000 mL | >120 | Hypotensive | Narrowed | 5-15 mL/hr | Confused |
| IV | >40% | >2,000 mL | >140 | Severely ↓ | Unobtainable | Negligible | Lethargic/Comatose |
From Mulholland and Greenfield's Surgery / ATLS classification
- Class I-II: crystalloid resuscitation usually sufficient
- Class III: blood transfusion + crystalloid
- Class IV: immediate blood transfusion + surgical/angiographic intervention
Progressive vs. Nonprogressive Shock
Nonprogressive (Compensated) Shock:
- Blood loss within tolerable limits
- Compensatory mechanisms (baroreceptors, RAAS, stress-relaxation) maintain circulation
- Patient can recover with adequate resuscitation
Progressive Shock:
- Blood loss exceeds a critical threshold (~45% in experimental models)
- "Shock causes more shock" - a vicious cycle of deterioration
- Mechanisms include: cardiac ischemia → decreased contractility, gut ischemia → toxin release, microvascular failure, coagulopathy
- Without intervention, leads to irreversible shock and death
Irreversible Shock:
- So much cellular and tissue damage that survival is impossible even with aggressive treatment
- Characterized by refractory hypotension, multiorgan failure
Hemodynamic Profile (Comparison Table)
| Shock Type | CO | SVR | PAOP | CVP | SvO2 |
|---|---|---|---|---|---|
| Hypovolemic | ↓ | ↑ | ↓ | ↓ | ↓ |
| Cardiogenic (LV MI) | ↓ | ↑ | ↑ | N/↑ | ↓ |
| Cardiogenic (RV MI) | ↓ | ↑ | N/↓ | ↑ | ↓ |
| Tamponade | ↓ | ↑ | ↑ | ↑ | ↓ |
| Distributive (early) | ↑/N | ↓ | N | N | ↑ |
Source: Mulholland and Greenfield's Surgery
The unique signature of hypovolemic shock: low CO + high SVR + low filling pressures (CVP, PCWP).
Clinical Features
- Tachycardia (earliest and most sensitive sign)
- Tachypnea
- Hypotension (late sign - appears after Class III)
- Narrowed pulse pressure
- Cool, pale, clammy skin (cutaneous vasoconstriction)
- Delayed capillary refill
- Oliguria/anuria (reduced renal perfusion)
- Altered mental status (anxiety → confusion → coma)
For non-hemorrhagic hypovolemia (plasma/fluid losses), additional features include:
- Hemoconcentration
- Elevated BUN and creatinine
- Hypernatremia (in free water losses)
Treatment
General Principles:
- Stop the source of loss (hemorrhage control, treat underlying cause)
- Restore intravascular volume (fluid resuscitation)
- Restore oxygen-carrying capacity (blood transfusion when indicated)
Specific Management:
| Class | Intervention |
|---|---|
| I | Observation; fluid replacement usually not needed |
| II | Crystalloid (isotonic saline or lactated Ringer's) |
| III | Crystalloid + packed red blood cells (pRBCs) |
| IV | Immediate blood products + emergent surgical/interventional radiology |
Hemorrhagic shock additional considerations:
- Damage control resuscitation: balanced ratio of pRBCs:FFP:platelets (1:1:1)
- Permissive hypotension: tolerate MAP 50-65 mmHg until hemorrhage controlled (avoid fluid overload and clot disruption before surgical control)
- Tranexamic acid (TXA): given within 3 hours of injury to reduce hemorrhage-related mortality
- Vasopressors: generally NOT first-line; used only if volume replacement is insufficient and patient remains unstable
For non-hemorrhagic losses: crystalloid replacement tailored to the specific electrolyte abnormality (e.g., hypotonic fluids for hypernatremia, repleting specific electrolytes for GI losses).
Monitoring Endpoints
- Urine output (target >0.5 mL/kg/hr in adults)
- Lactate clearance (target normalization within 6 hours)
- Heart rate normalization
- Mean arterial pressure (target >65 mmHg)
- CVP/PCWP if central monitoring available
- Point-of-care ultrasound (POCUS): a recent 2025 systematic review (PMID: 40603759) confirms POCUS has high diagnostic accuracy in differentiating shock types
Key Sources:
- Guyton and Hall Textbook of Medical Physiology, Ch. 24
- Mulholland and Greenfield's Surgery, Ch. 9
- Harrison's Principles of Internal Medicine 22E
- Costanzo Physiology, 7th Ed., Box 4.3
- Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.