CSF RHINORRHEA AND ITS TREATMENT
Reading File
Finding Sources
Finding Sources
Searching PubMed
"CSF rhinorrhea" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent - I now have very comprehensive textbook content. I have all the information needed to compose a thorough, well-structured answer. Let me compile it now.
CSF Rhinorrhea
Definition
Cerebrospinal fluid (CSF) rhinorrhea results from a direct communication between the CSF-containing subarachnoid space and the mucosalized space of the paranasal sinuses. This communication creates a pathway for bacterial pathogens to reach the intracranial compartment, making meningitis the most feared complication. The skull base defect can also allow pneumocephalus and secondary brain compression.
- Cummings Otolaryngology, p. 948
Classification
CSF rhinorrhea is broadly divided into Traumatic (>90%) and Nontraumatic (<10%) categories:
I. Traumatic
A. Accidental (most common)
- Immediate (within 48 hours of injury)
- Delayed (weeks to months later)
- Most fistulas due to accidental trauma are at the anterior cranial base, typically the cribriform plate
- Approximately 80% of all traumatic leaks occur after accidental trauma (mostly closed head injuries)
- CSF rhinorrhea is noted in only 2-3% of serious head trauma cases; skull base fractures are associated with a CSF fistula in 12-30% of cases
B. Surgical (Iatrogenic)
- Complication of neurosurgical procedures: transsphenoidal hypophysectomy, frontal craniotomy, other skull base procedures
- Complication of rhinologic procedures: endoscopic sinus surgery (reported rate ~0.5%), septoplasty, combined skull base procedures
- Recent data suggest iatrogenic CSF leaks may now be more common than accidental trauma leaks
II. Nontraumatic (<10%)
A. With Elevated Intracranial Pressure
- Intracranial neoplasm
- Hydrocephalus (communicating or obstructive)
- Benign intracranial hypertension (BIH/idiopathic intracranial hypertension)
B. With Normal Intracranial Pressure
- Congenital anomaly
- Skull base neoplasm (nasopharyngeal carcinoma, sinonasal tumors)
- Skull base erosive process (sinus mucosa, osteomyelitis, granulomatous disease including granulomatosis with polyangiitis)
- Idiopathic (true "spontaneous" - reserved for cases where investigation fails to reveal a cause)
Note: Idiopathic nontraumatic CSF rhinorrhea is strongly linked to elevated ICP, benign intracranial hypertension, and empty sella syndrome. These three entities may be manifestations of the same underlying pathophysiologic derangement.
- Cummings Otolaryngology, p. 949-950
Pathophysiology
CSF is produced by the choroid plexus at 20 mL/hour in adults. Total CSF volume is ~140 mL (20 mL ventricles, 50 mL intracranial subarachnoid space, 70 mL paraspinal subarachnoid space). Normal CSF pressure is 4 cm H₂O in infants and up to 14 cm H₂O in adults.
For rhinorrhea to occur:
- There must be a bony defect in the skull base (cribriform plate, ethmoid roof, sphenoid sinus wall, etc.)
- A dural tear must be present
- CSF pressure must overcome the local tissue resistance
In trauma, CSF leaks usually develop because of shearing forces across the thin cribriform plate. In elevated ICP states, persistent pressure erodes thin areas of bone over time. Meningoencephaloceles may accompany the leak, particularly in the non-traumatic idiopathic group.
- Cummings Otolaryngology, pp. 3150-3170
Clinical Features
- Unilateral, watery, clear nasal discharge - often described as having a characteristic metallic or salty taste
- Discharge typically worsens with head bending forward or Valsalva maneuver (reservoir sign / "Dandy sign")
- May be positional or intermittent
- Headache (sometimes from low ICP if large leak)
- History of head trauma, skull base surgery, or features of raised ICP (papilledema, pulsatile tinnitus, visual obscurations)
Diagnosis
1. Clinical Suspicion
The classic "halo sign" (a ring of clear fluid surrounding a blood stain on filter paper) is unreliable and has been largely abandoned.
2. Biochemical Confirmation
- Beta-2 transferrin: The gold standard biochemical test. A CSF-specific protein (also found in perilymph and aqueous humor but not in serum/nasal secretions) - highly sensitive and specific for CSF.
- Beta-trace protein (prostaglandin D2 synthase): An alternative with high sensitivity/specificity; results available more rapidly than beta-2 transferrin.
3. Imaging & Localization
| Modality | Details |
|---|---|
| High-resolution CT of skull base | First-line imaging; identifies bony defects; best for cribriform, ethmoid roof, sphenoid; non-invasive |
| CT cisternography | LP + intrathecal iodinated contrast; high spatial resolution; requires active leak to be reliable; good localization |
| MRI cisternography | Non-invasive (no LP needed with specific protocols); good soft tissue detail; identifies meningoencephaloceles; better than CT for soft tissue extent |
| Radionuclide cisternography | LP + intrathecal radiotracer; pledgets placed in nose; low spatial resolution; poor sensitivity; largely replaced by CT/MRI |
| Intrathecal fluorescein | Dilute fluorescein (0.1 mL of 10% solution diluted in 10 mL CSF) given intrathecally; endoscopic visualization identifies the exact leak site intraoperatively; risk of serious neurologic sequelae at higher doses - must use dilute concentration |
Both CT and MRI cisternography offer far superior spatial resolution compared to radionuclide cisternography but still require a relatively large, active leak for reliable detection.
- Cummings Otolaryngology, p. 3011
Treatment
Conservative Management
Indicated primarily for traumatic CSF leaks:
- Bed rest with head of bed elevation (15-30°)
- Avoidance of Valsalva (no nose blowing, straining, coughing)
- Lumbar drainage: Drains at the rate of CSF production (~20 mL/hour); the drainage bag is pinned at shoulder level; tubing is clamped for ambulation. Over-drainage must be avoided (risk of subdural hematoma).
- Prophylactic antibiotics: Historically used, but current evidence does NOT support routine antibiotic prophylaxis for traumatic CSF leaks (may select resistant organisms without preventing meningitis).
The majority of traumatic (post-accidental) leaks resolve spontaneously within 5-7 days. If the leak persists beyond 7 days of conservative management, lumbar drainage is initiated. If it persists after 5-7 days of lumbar drainage, surgical repair is considered.
Nontraumatic (spontaneous) CSF rhinorrhea is unlikely to resolve spontaneously and almost always requires operative repair after excluding etiologic causes (e.g., brain tumor).
- Cummings Otolaryngology, p. 3019-3023; Shambaugh Surgery of the Ear, p. 3495-3503
Surgical Repair
1. Endoscopic Endonasal Repair (Current Gold Standard)
Endoscopic repair has supplanted traditional transcranial approaches and is now the standard of care, with success rates >90%. First popularized by Papay et al. (1989) and Mattox & Kennedy (1990), it is minimally invasive and avoids craniotomy.
Key Steps:
- Identify the leak site (aided by intrathecal fluorescein)
- Remove bony partitions around the defect to create a flat surface
- Strip adjacent sinus mucosa to create denuded bone for graft adherence
- Place graft material:
- Autogenous: Fascia lata, free bone graft, fat, free nasal mucosal graft (middle turbinate mucosa or nasal floor mucosa are reliable donor sites)
- Allograft: Acellular dermal allograft
- Xenogeneic: Collagen dural substitutes
- A free mucosal graft is placed as an overlay
- Secure with surgical sealant (fibrin glue) + resorbable collagen-based packing ± nonresorbable sponge packing
- For high-flow leaks or large dural defects: vascularized mucosal flaps (e.g., nasoseptal flap) are preferred over free grafts
Intraoperative CSF leaks (during endoscopic sinus surgery): Should be repaired immediately at the time of recognition.
Postoperative care:
- Head CT and MRI post-repair to exclude intracranial bleeding/injury
- Neurosurgical and infectious disease consultation
- Lumbar drains are NOT routinely recommended post-repair (studies have not confirmed benefit). They may be used selectively in patients with confirmed or suspected raised ICP.
- Cummings Otolaryngology, pp. 3017-3025; K.J. Lee's Essential Otolaryngology, pp. 10190-10202
2. Historical/Alternative Approaches
| Approach | Details |
|---|---|
| Bicoronal craniotomy (Dandy, 1926) | First successful repair; fascia lata graft; high morbidity; reserved for complex/failed cases or defects not accessible endoscopically |
| Extracranial (Lynch) approach | Mid-20th century; external naso-orbital incision; avoids brain retraction |
| Transsphenoidal approach | For sphenoid sinus leaks |
| Middle fossa craniotomy | For tegmen defects, especially those anterior to the epitympanum or >1.5 cm in diameter; also used for spontaneous leaks from tegmen dehiscence |
| Transmastoid approach | For tegmen defects posterior to the epitympanum |
3. Management of Specific Situations
Postsurgical CSF rhinorrhea (e.g., after acoustic neuroma surgery):
- CSF percolates through mastoid air cells to nasopharynx via the Eustachian tube
- Try lumbar drain for 5 days if presenting in the first few days post-op
- If it persists: reoperation for internal sealing
- If hearing has been sacrificed: Eustachian tube obliteration via transcanal procedure (Friedman technique) - circumferential ear canal incision, resection of TM/skin, Eustachian tube packed with fascia/muscle, ear canal everted and closed
Spontaneous CSF leaks from tegmen dehiscence:
- Usually from congenitally thin tegmen or arachnoid granulations
- Intermittent course until surgically repaired
- Repair via middle fossa (large defects >1.5 cm, or anterior to epitympanum) or transmastoid approach (posterior defects)
- Repair uses combination of fascia/perichondrium + cartilage or bone
Complications of Untreated CSF Rhinorrhea
- Bacterial meningitis - most feared; risk increases with duration of leak
- Pneumocephalus - air entry through the defect
- Brain abscess
- Recurrent meningitis - should raise suspicion for an occult CSF fistula
Recent Evidence (2024-2026)
Three recent high-quality publications update the evidence base:
-
Mughal Z et al. (2026) - Meta-analysis of endoscopic management of spontaneous CSF rhinorrhea (Laryngoscope, PMID: 40650638): Provides pooled outcome data confirming high success rates with endoscopic repair.
-
O'Leary S et al. (2024) - Systematic review of evidence-based approaches to cranial CSF leaks in low- and middle-income countries (Neurosurg Rev, PMID: 39738756): Addresses resource-limited settings and conservative vs. surgical options.
-
Samargandy SA et al. (2025) - Case series + systematic review of traumatic CSF rhinorrhea associated with COVID-19 nasal testing (Eur Arch Otorhinolaryngol, PMID: 39277828): Highlights iatrogenic CSF rhinorrhea from nasopharyngeal swabs as an emerging entity.
Summary Algorithm
CSF Rhinorrhea
│
├── Confirm Diagnosis
│ ├── Beta-2 transferrin / Beta-trace protein
│ └── CT skull base ± CT/MRI cisternography
│
├── TRAUMATIC
│ ├── Conservative: Bed rest, head elevation, avoid Valsalva (5-7 days)
│ ├── If persistent >7 days → Lumbar drain (5-7 days)
│ └── If persistent → Endoscopic surgical repair
│
└── NONTRAUMATIC / SPONTANEOUS
├── Exclude underlying cause (tumor, BIH, hydrocephalus)
├── Treat raised ICP if present (acetazolamide, weight loss, VP shunt)
└── Surgical repair (almost always required)
├── Endoscopic endonasal repair (first choice, >90% success)
└── Craniotomy/middle fossa (large defects, failed endoscopic)
Sources: Cummings Otolaryngology Head and Neck Surgery (Chapter 48, pp. 948-975) | K.J. Lee's Essential Otolaryngology (pp. 615-616) | Shambaugh Surgery of the Ear (pp. 3478-3514)
Generate a comparison poster: traumatic vs. nontraumatic CSF rhinorrhea management
Generating Image
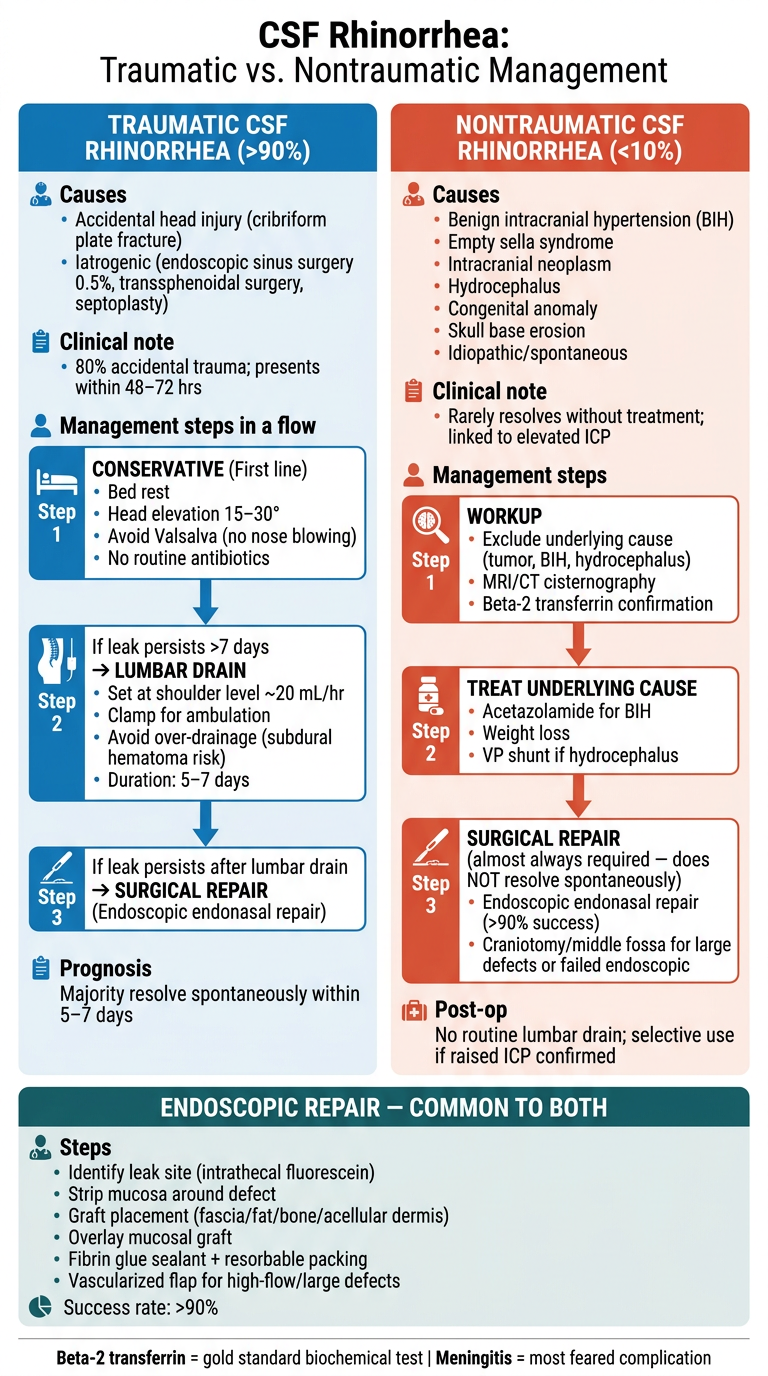
Here is the comparison poster. It covers:
-
Left (Blue) - Traumatic: Step-by-step management from conservative measures through lumbar drain to surgical repair, with the key point that most resolve spontaneously within 5-7 days.
-
Right (Red/Orange) - Nontraumatic: Emphasizes the need to rule out underlying causes first, treat elevated ICP medically, and that surgical repair is almost always required since these leaks rarely resolve on their own.
-
Bottom (Teal) - Shared Section: The endoscopic endonasal repair technique that applies to both types, including graft materials and >90% success rate.
Key facts are highlighted throughout - the 90/10 split, the 0.5% iatrogenic ESS rate, beta-2 transferrin as the gold standard test, and meningitis as the most feared complication.
COPD DIAGNOSIS AND ITS TREATMENT
Reading File
Finding Sources
Finding Sources
Searching PubMed
"COPD" AND "diagnosis" AND "management"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content across all major sections. Let me compile the full, detailed answer.
COPD: Diagnosis and Treatment
Definition
Chronic obstructive pulmonary disease (COPD) is an umbrella term for conditions that result in fixed airway obstruction and dyspnea on exertion. It is characterized by persistent respiratory symptoms and airflow limitation due to airway or alveolar abnormalities, usually caused by significant exposure to noxious particles or gases. Nearly all patients have elements of both:
- Emphysema: air space destruction with loss of alveolar walls and capillary beds
- Chronic bronchitis: daily cough and sputum production for ≥3 months in ≥2 consecutive years
Airflow limitation is formally defined as post-bronchodilator FEV1/FVC < 0.70.
- Goldman-Cecil Medicine, p. 892
Epidemiology
- Global prevalence: ~175 million people
- Third leading cause of death worldwide - 3.2 million deaths annually
- Presents typically in the sixth decade or later
- US costs: ~$50 billion/year ($30B direct, $20B indirect)
- Cigarette smoking is the major risk factor; pack-years inversely correlate with FEV1
Other risk factors:
- Biomass fuel combustion (cooking/heating in poorly ventilated spaces)
- Occupational dust exposure (mining, grain handling, cotton mills)
- Childhood respiratory infections (impair lung growth, lower peak FEV1)
- Alpha-1 antitrypsin (α1-AT) deficiency (genetic predisposition)
- Air pollution (associated with increased mortality in established COPD)
Pathobiology
Pathogenesis
1. Protease-Antiprotease Imbalance (primary mechanism for emphysema)
- Cigarette smoking triggers influx of neutrophils and macrophages into the lung
- Excess elastolytic protease activity (neutrophil elastase, macrophage elastases) overwhelms antiprotease defenses (α1-antitrypsin)
- Leads to degradation of alveolar elastin → permanent air space enlargement
- α1-Antitrypsin deficiency is the genetic prototype of this mechanism
2. Airway Inflammation
- CD8+ lymphocytes, neutrophils, and macrophages dominate (unlike asthma which is eosinophilic)
- A subset of COPD patients do show peripheral/sputum eosinophilia (clinically important - these respond to inhaled corticosteroids)
- Small airway inflammation, wall thickening, and fibrosis → fixed obstruction in airways <2 mm
3. Vascular and Apoptotic Mechanisms
- Reduced VEGF expression → apoptosis of septal endothelial cells
- Chronic hypoxemia → pulmonary vasoconstriction → pulmonary hypertension
Key point: The inflammatory response in the lung persists after smoking cessation, explaining continued disease progression even after quitting.
Pathophysiology
- Obstruction in small airways (<2 mm) is the anatomic site
- Mechanisms: smooth muscle constriction, wall thickening, loss of airways, dynamic airway collapse
- Dynamic hyperinflation: During exertion, expiratory flow limitation forces air trapping, increasing end-expiratory lung volume, flattening the diaphragm, increasing respiratory muscle fatigue, and causing intolerable dyspnea
- Ventilation-perfusion (V/Q) mismatch → hypoxemia
- DLCO reduction on PFTs reflects parenchymal destruction (emphysema component)
Clinical Features
| Feature | Details |
|---|---|
| Dyspnea | Exertional initially, progressing to rest; the dominant symptom |
| Chronic cough | Often productive; may precede dyspnea by years |
| Sputum production | Typically mucoid; purulent during exacerbations |
| Wheeze | Especially on exertion |
| Barrel chest | Increased AP diameter due to hyperinflation |
| Pursed-lip breathing | Increases end-expiratory pressure, reduces dynamic collapse |
| Accessory muscle use | Sternocleidomastoid, scalenes recruited |
| Weight loss/cachexia | In advanced disease |
| Cor pulmonale | Elevated JVP, peripheral edema, right heart failure from chronic hypoxemia |
Classic Phenotypes
- "Pink Puffer" (emphysema predominant): Thin, breathless, non-cyanotic, uses accessory muscles, pursed-lip breathing, minimal sputum, preserved gas exchange until late
- "Blue Bloater" (chronic bronchitis predominant): Obese, cyanotic, productive cough, cor pulmonale, early hypoxemia, more frequent exacerbations
Diagnosis
1. Spirometry (mandatory - gold standard)
| Criterion | Finding |
|---|---|
| Post-bronchodilator FEV1/FVC | < 0.70 (confirms airflow obstruction) |
| Bronchodilator reversibility | <12% or <200 mL improvement (distinguishes from asthma) |
| FEV1 % predicted | Determines GOLD severity grade |
2. GOLD Spirometric Grading (based on FEV1 % predicted, post-bronchodilator)
| GOLD Grade | FEV1 % Predicted | Severity |
|---|---|---|
| GOLD 1 | ≥80% | Mild |
| GOLD 2 | 50-79% | Moderate |
| GOLD 3 | 30-49% | Severe |
| GOLD 4 | <30% | Very severe |
3. GOLD ABE Assessment Groups (symptom + exacerbation risk)
The GOLD 2023 report shifted from ABCD groups to ABE groups:
- Group A: 0-1 exacerbations (not leading to hospitalization), low symptoms (mMRC 0-1 / CAT <10)
- Group B: 0-1 exacerbations (not leading to hospitalization), high symptoms (mMRC ≥2 / CAT ≥10)
- Group E: ≥2 exacerbations or ≥1 hospitalization (high exacerbation risk)
4. Symptom Assessment Tools
- Modified Medical Research Council (mMRC) dyspnea scale: 0-4; ≥2 = significant symptoms
- COPD Assessment Test (CAT): 0-40 score; ≥10 = high symptom burden
5. Additional Investigations
| Test | Purpose |
|---|---|
| Chest X-ray | Hyperinflation, flattened diaphragms, increased retrosternal air space, bullae; excludes other causes |
| High-resolution CT chest | Characterizes emphysema distribution, detects bronchiectasis, airway wall thickening; not routine but valuable |
| DLCO (diffusing capacity) | Reduced in emphysema; normal/elevated in chronic bronchitis; helps distinguish subtypes |
| Arterial blood gas (ABG) | Hypoxemia (PaO₂ <60 mmHg), hypercapnia (PaCO₂ >45 mmHg) in advanced disease; guides O₂ therapy |
| Alpha-1 antitrypsin level | Screen all COPD patients once; deficiency (<20% of normal) warrants augmentation therapy |
| 6-Minute Walk Test / CPET | Functional assessment; 6MWT distance is a strong predictor of mortality |
| Echocardiogram | Assess for pulmonary hypertension and cor pulmonale |
| Full blood count | Polycythemia (from chronic hypoxemia); eosinophil count guides ICS use |
6. Differential Diagnosis
- Asthma: Younger onset, atopy, variable/reversible obstruction, eosinophilic inflammation
- Bronchiectasis: Purulent sputum, dilated/thickened airways on HRCT
- Bronchiolitis obliterans: Post-transplant or industrial inhalant exposure
- Congestive heart failure: Bibasal crackles, elevated BNP, normal spirometry with restrictive pattern
Treatment
No intervention other than lung transplantation can reverse or cure COPD. Treatment focuses on modifying natural history, improving symptoms, minimizing complications, and reducing mortality.
- Goldman-Cecil Medicine, p. 897
A. Non-Pharmacological (Foundation of Management)
1. Smoking Cessation - single most effective intervention
- Reduces the rate of FEV1 decline and overall long-term mortality
- Also reduces lung cancer and cardiovascular mortality
- Methods: behavioral counseling + pharmacotherapy
- Varenicline (most effective): partial nicotinic receptor agonist
- Bupropion: atypical antidepressant; doubles quit rates
- Nicotine replacement therapy (NRT): patches, gum, inhaler
2. Pulmonary Rehabilitation
- Multidisciplinary program including exercise training, education, nutritional counseling
- Reduces dyspnea and fatigue, improves exercise capacity and quality of life
- Recommended for all patients with mMRC ≥2 or CAT ≥10
- Does not improve FEV1 but improves functional outcomes
3. Vaccinations
- Annual influenza vaccine (reduces COPD exacerbations and mortality)
- Pneumococcal vaccine (PPSV23 + PCV13/PCV15/PCV20)
- COVID-19 vaccine
- Pertussis (Tdap) booster
4. Nutritional Support
- Malnutrition and muscle wasting are independent predictors of mortality
- BMI <21 is associated with increased mortality
B. Pharmacological Treatment - Stable COPD
Bronchodilators (cornerstone of treatment)
1. Short-Acting Beta-2 Agonists (SABA)
- Salbutamol (albuterol), terbutaline
- For rescue/as-needed use; rapid onset (5-15 min)
- Mechanism: relaxes airway smooth muscle via β2 receptor activation → bronchodilation
2. Short-Acting Muscarinic Antagonists (SAMA)
- Ipratropium bromide
- Can provide a small increase in FEV1; useful as add-on or SABA alternative
- Does not impact the rate of FEV1 decline
3. Long-Acting Beta-2 Agonists (LABA)
- Salmeterol, formoterol, indacaterol, olodaterol
- Twice or once daily; reduces dyspnea and exacerbations
- Improves FEV1, exercise tolerance, quality of life
4. Long-Acting Muscarinic Antagonists (LAMA)
- Tiotropium, umeclidinium, glycopyrronium, aclidinium
- Once daily; considered the preferred first-line bronchodilator in COPD
- Tiotropium modestly reduces FEV1 decline in early-stage COPD (UPLIFT trial)
- Reduces exacerbations more effectively than LABA alone
- Preferred over LABA for exacerbation prevention
5. LABA + LAMA (dual bronchodilation)
- Umeclidinium/vilanterol, tiotropium/olodaterol, glycopyrronium/indacaterol
- Superior to monotherapy for symptoms, exacerbations, and FEV1
- Preferred for symptomatic patients (GOLD Group B/E)
Inhaled Corticosteroids (ICS)
- Fluticasone, budesonide, beclomethasone
- NOT recommended as monotherapy in COPD
- Used as ICS + LABA combination (e.g., salmeterol/fluticasone, formoterol/budesonide)
- Benefits: reduces exacerbation frequency in patients with blood eosinophils ≥300 cells/μL
- Side effects: pneumonia risk (significant), oral candidiasis, osteoporosis
- Consider ICS addition when: ≥2 exacerbations/year + blood eosinophils ≥100 cells/μL (especially ≥300 cells/μL)
- Avoid/withdraw ICS when: blood eosinophils <100 cells/μL, recurrent pneumonia
Triple Therapy (ICS + LABA + LAMA)
- e.g., fluticasone/umeclidinium/vilanterol (Trelegy), budesonide/glycopyrronium/formoterol
- Recommended for Group E patients (high exacerbation risk) with blood eosinophils ≥100 cells/μL
- Reduces exacerbations more than dual therapy (IMPACT, ETHOS trials)
GOLD Initial Pharmacotherapy Algorithm
| GOLD Group | Initial Pharmacotherapy |
|---|---|
| Group A | Bronchodilator (SABA or LAMA or LABA) |
| Group B | LAMA + LABA (dual bronchodilation) |
| Group E | LAMA + LABA; consider ICS if eosinophils ≥300 cells/μL (triple therapy) |
Other Pharmacological Agents
| Drug | Class | Indication | Notes |
|---|---|---|---|
| Roflumilast | PDE4 inhibitor | Severe COPD (FEV1 <50%) + chronic bronchitis + frequent exacerbations | Oral; reduces exacerbations; side effects: nausea, weight loss, depression |
| Azithromycin | Macrolide antibiotic | Prophylaxis in frequent exacerbators (≥3/year) | Once-daily or 3x/week; risk of hearing loss, QTc prolongation, macrolide resistance |
| Theophylline | Methylxanthine | Add-on in resource-limited settings | Narrow therapeutic window; interactions; not a preferred agent |
| N-acetylcysteine (NAC) | Mucolytic/antioxidant | May reduce exacerbations in selected patients | Limited evidence |
| Alpha-1 antitrypsin augmentation | IV protein replacement | Proven α1-AT deficiency with emphysema | Weekly IV infusions; slows emphysema progression |
C. Oxygen Therapy
Long-Term Oxygen Therapy (LTOT) - the only pharmacological intervention proven to reduce mortality (along with smoking cessation) in severe COPD:
| Indication | Criteria |
|---|---|
| Absolute | PaO₂ ≤55 mmHg (SaO₂ ≤88%) at rest on room air |
| Conditional | PaO₂ 56-60 mmHg with cor pulmonale, erythrocytosis (Hct >55%), or pulmonary hypertension |
- Target SaO₂: 88-92% (avoid over-oxygenation - may worsen hypercapnia via Haldane effect and loss of hypoxic drive)
- Minimum 15 hours/day to achieve survival benefit
- Ambulatory oxygen for exercise-induced desaturation improves exercise capacity
D. Management of COPD Exacerbations
Definition: An acute worsening of respiratory symptoms (dyspnea, cough, sputum) beyond normal day-to-day variation, requiring a change in medication.
Triggers: Respiratory infections (Haemophilus influenzae, Streptococcus pneumoniae, Moraxella catarrhalis, rhinovirus), air pollution, pulmonary embolism.
Treatment:
- Short-acting bronchodilators (SABA ± SAMA) - first-line; frequent nebulization
- Systemic corticosteroids: Prednisone 40 mg/day for 5 days (reduces recovery time, treatment failure, and length of stay; longer courses add no benefit)
- Antibiotics: Indicated when sputum is purulent (or 2 of 3 Anthonisen criteria: increased dyspnea, sputum volume, sputum purulence). Amoxicillin-clavulanate, azithromycin, or doxycycline for mild-moderate; fluoroquinolone for severe/hospitalized
- Controlled oxygen: Target SaO₂ 88-92%
- Non-invasive ventilation (NIV/BiPAP): For acute hypercapnic respiratory failure (pH <7.35, PaCO₂ >45 mmHg); reduces intubation, mortality, and length of ICU stay
- Mechanical ventilation: For severe respiratory failure failing NIV; carries high weaning difficulty
E. Surgical and Interventional Options
| Procedure | Indication | Mechanism/Notes |
|---|---|---|
| Lung Volume Reduction Surgery (LVRS) | Upper-lobe predominant emphysema + low exercise capacity | Resects most diseased lung tissue, improves diaphragm mechanics, reduces dynamic hyperinflation; NETT trial: mortality benefit in selected patients |
| Bronchoscopic Lung Volume Reduction (BLVR) | Severe emphysema with hyperinflation, intact interlobar fissures | Endobronchial valves (Zephyr) block target lobe → atelectasis; reduces hyperinflation; improves FEV1 and 6MWD |
| Bullectomy | Giant bulla (>1/3 of hemithorax) compressing adjacent lung | Resection of bulla; improves mechanics |
| Lung Transplantation | End-stage COPD (GOLD 4), BODE index ≥7, severe exacerbations | Only cure; COPD is the most common indication for lung transplant; improves quality of life and exercise capacity; modest survival benefit |
F. Palliative Care
- For end-stage or treatment-refractory COPD
- Low-dose oral morphine: Reduces refractory dyspnea; not associated with respiratory depression at low doses
- Anxiolytics (low-dose benzodiazepines) for dyspnea-related anxiety
- Advance care planning and hospice referral when appropriate
COPD Monitoring and Follow-Up
| Parameter | Target/Goal |
|---|---|
| Spirometry | Annual monitoring of FEV1 decline |
| Symptom scores | CAT <10, mMRC <2 |
| Exacerbation frequency | <2 per year; ≥2 = "frequent exacerbator" phenotype |
| Blood eosinophil count | Guides ICS use decisions |
| SaO₂ and ABG | If FEV1 <50%, screen for hypoxemia to qualify for LTOT |
| BMI | Nutritional support if <21 |
Summary Treatment Algorithm
STABLE COPD - Initial Pharmacotherapy
│
├── ALL PATIENTS:
│ Smoking cessation + Pulmonary rehabilitation + Vaccinations
│
├── GROUP A (Low risk, low symptoms)
│ → Single bronchodilator (SABA or LAMA or LABA, as needed or regular)
│
├── GROUP B (Low risk, high symptoms)
│ → LAMA + LABA (dual bronchodilation)
│
└── GROUP E (High exacerbation risk)
├── Eosinophils ≥300 cells/μL → ICS + LABA + LAMA (Triple therapy)
├── Eosinophils 100-299 cells/μL → LAMA + LABA; consider adding ICS
└── Eosinophils <100 cells/μL → LAMA + LABA (no ICS)
└── Add roflumilast if FEV1 <50% + chronic bronchitis
└── Add azithromycin if ex-smoker + frequent exacerbations
Sources: Goldman-Cecil Medicine (Chapter 76, pp. 890-900) | Murray & Nadel's Textbook of Respiratory Medicine | Fishman's Pulmonary Diseases | Robbins & Kumar Basic Pathology | GOLD 2023 Global Strategy Report (cited in Goldman-Cecil, p. 3301)
Generate a poster: COPD FOR CONTENT MENTIONED ABOVE
Generating Image
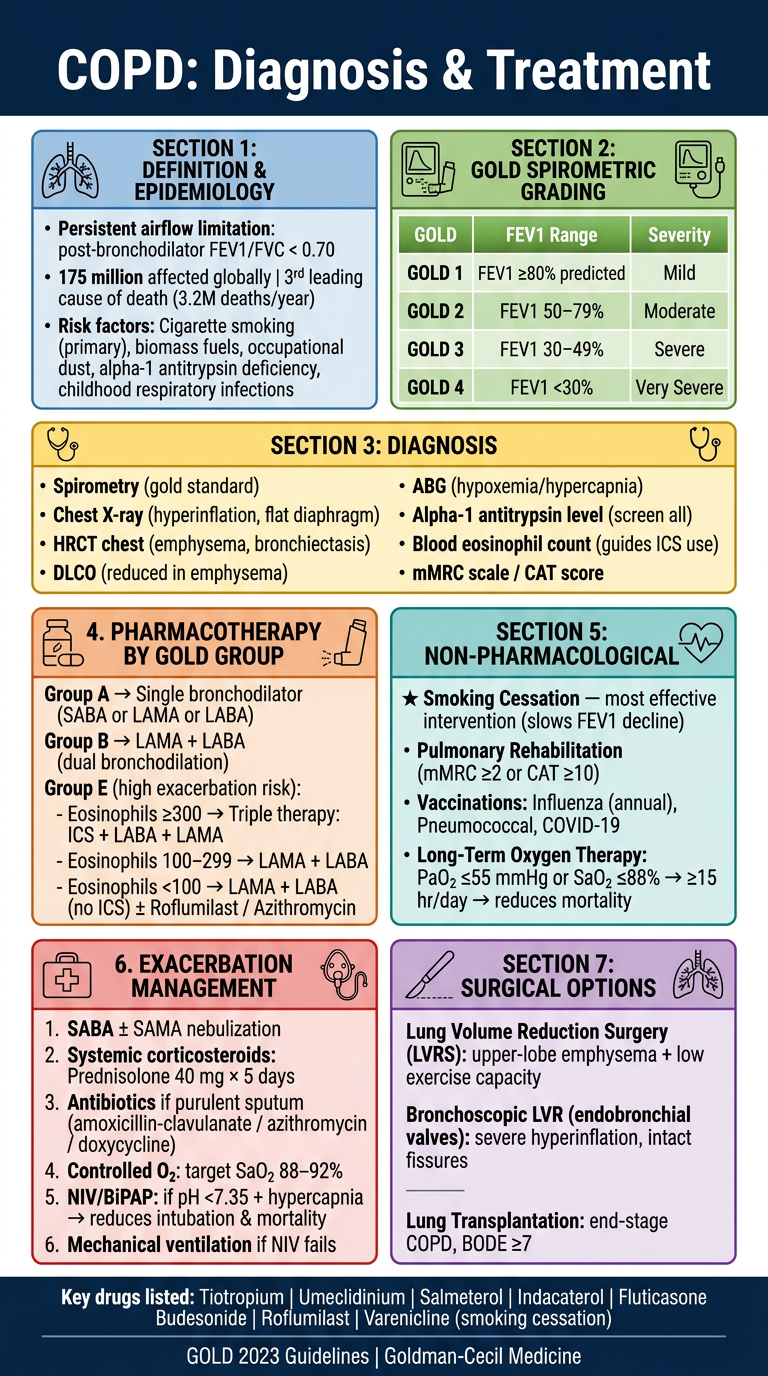
Here is the comprehensive COPD poster covering all content from the discussion above, organized into 7 color-coded sections:
| Section | Color | Content |
|---|---|---|
| Definition & Epidemiology | Blue | FEV1/FVC <0.70, global burden, risk factors |
| GOLD Grading | Green | GOLD 1-4 severity grades by FEV1% |
| Diagnosis | Yellow | Spirometry, HRCT, DLCO, ABG, alpha-1 AT, eosinophils |
| Pharmacotherapy | Orange | Group A/B/E treatment ladder with eosinophil-guided ICS use |
| Non-Pharmacological | Teal | Smoking cessation, pulmonary rehab, vaccinations, LTOT |
| Exacerbation Management | Red | SABA/SAMA, steroids, antibiotics, O₂, NIV, intubation |
| Surgical Options | Purple | LVRS, bronchoscopic LVR, lung transplantation |
The poster serves as a quick clinical reference aligned with GOLD 2023 Guidelines.
This is a shared conversation. Sign in to Orris to start your own chat.