Jaundice short note
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the short note.
Jaundice - Short Note
Definition
Jaundice (icterus) is the yellow discoloration of the skin, sclerae, nail beds, and mucous membranes caused by bilirubin deposition secondary to hyperbilirubinemia. Normal serum bilirubin is ≤1 mg/dL; jaundice becomes clinically visible at 2-3 mg/dL.
- Biochemistry, Lippincott Illustrated Reviews, 8th ed., p. 799
- Schwartz's Principles of Surgery, 11th ed., p. 1381
Bilirubin Metabolism (Background)
- Heme from senescent RBCs is catabolized by macrophages → free bilirubin (unconjugated, lipophilic)
- Unconjugated bilirubin (UCB) binds albumin in plasma → transported to the liver
- Hepatocytes conjugate UCB with glucuronic acid via UGT1A1 → water-soluble conjugated bilirubin (CB, "direct bilirubin")
- CB is secreted into bile canaliculi (rate-limiting, energy-dependent step)
- In intestine, gut bacteria reduce CB → urobilinogen → stercobilin (brown stool color). Some urobilinogen is reabsorbed → excreted in urine as urobilin (yellow urine color)
Classification
Jaundice is divided into three types based on the site of defect:
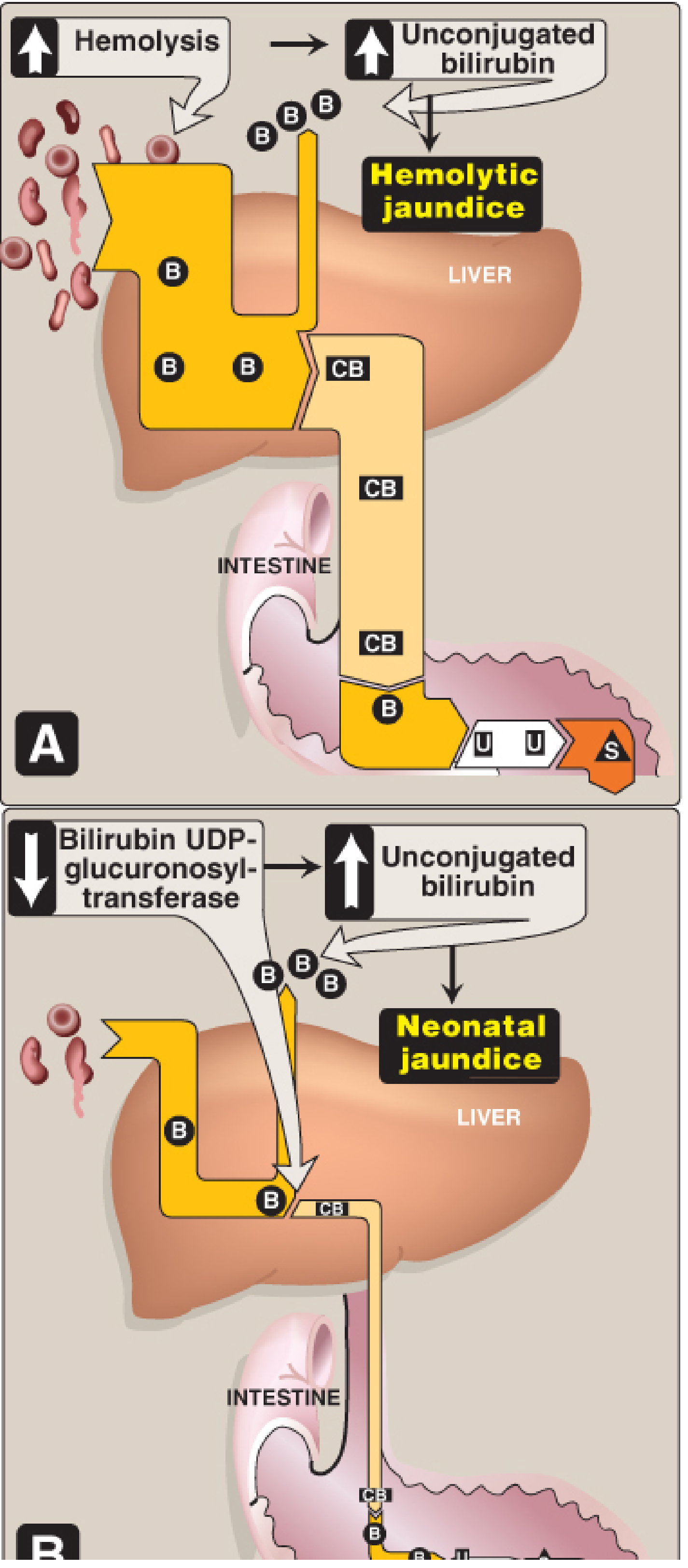
1. Prehepatic (Hemolytic) Jaundice
- Cause: Excessive hemolysis overwhelms the liver's conjugating capacity
- Examples: Sickle cell anemia, G6PD deficiency, pyruvate kinase deficiency, immune hemolytic anemias, malaria
- Biochemistry: Elevated UCB only; CB normal or high-normal; urobilinogen increased in urine; no bilirubin in urine; stools normally colored
- Also includes protein-loss states (burns, malnutrition) - decreased albumin fails to carry UCB to liver
2. Hepatocellular (Intrahepatic) Jaundice
- Cause: Liver cell damage impairs conjugation and/or excretion
- Examples: Viral hepatitis, cirrhosis, alcoholic liver disease, sepsis, drug toxicity (acetaminophen, oral contraceptives, anabolic steroids), autoimmune hepatitis
- Inherited disorders:
- Gilbert's syndrome - mild UGT1A1 deficiency (~4-7% of population); benign, mild UCB rises with fasting/stress
- Crigler-Najjar syndrome - near-complete/complete UGT1A1 deficiency; rare, severe; can cause kernicterus in neonates
- Dubin-Johnson syndrome / Rotor's syndrome - defects in secretion of CB from hepatocyte into bile → conjugated hyperbilirubinemia
- Biochemistry: Both UCB and CB elevated; ALT/AST elevated; urinary urobilinogen increased; dark urine; pale stools
3. Posthepatic (Obstructive/Extrahepatic Cholestatic) Jaundice
- Cause: Obstruction of the biliary ductal system preventing CB flow into duodenum
- Intrinsic: Cholelithiasis, choledocholithiasis, cholangiocarcinoma, biliary strictures, cholangitis, papilla of Vater disorders, primary sclerosing cholangitis
- Extrinsic: Carcinoma head of pancreas (commonest malignant cause), pancreatitis, pseudocyst
- Iatrogenic: Surgical clips, retained stones, bile duct ischemia
- Biochemistry: Elevated CB (conjugated hyperbilirubinemia); CB appears in urine (dark urine - "cola-colored"); urinary urobilinogen absent; stools pale/clay-colored; GI pain, nausea
Schwartz's Principles of Surgery, 11th ed., pp. 1381-1382
Neonatal Jaundice
- Occurs in ~60% of full-term and ~80% of preterm neonates
- Due to: high RBC turnover + immature UGT1A1 (reaches adult levels at ~4 weeks)
- Physiological neonatal jaundice: transient UCB rise in first postnatal week, self-limiting
- Pathological causes: isoimmunization (Rh/ABO), heritable hemolytic disorders, extravasated blood (cephalhematoma), Crigler-Najjar syndrome
- Kernicterus: UCB >20-25 mg/dL (exceeds albumin binding capacity) crosses the blood-brain barrier → deposits in basal ganglia → toxic encephalopathy, hearing loss, choreoathetosis
- Treatment: Blue fluorescent light (phototherapy) converts UCB to water-soluble photoisomers excreted in bile without conjugation; exchange transfusion in severe cases
Lippincott Biochemistry, 8th ed., p. 800; Medical Physiology (Boron & Boulpaep), p. 46-6
Lab Findings Summary Table
| Parameter | Prehepatic | Hepatocellular | Posthepatic |
|---|---|---|---|
| Serum UCB | ↑↑ | ↑ | Normal |
| Serum CB | Normal/slight ↑ | ↑ | ↑↑ |
| Urine bilirubin | Absent | Present | Present |
| Urine urobilinogen | ↑↑ | ↑ | Absent |
| Stool color | Normal/dark | Pale | Pale/clay |
| ALT/AST | Normal | ↑↑ | Normal/mild ↑ |
| ALP/GGT | Normal | Normal/mild ↑ | ↑↑ |
Bilirubin Measurement
Bilirubin is measured by the van den Bergh reaction using diazotized sulfanilic acid:
- Direct bilirubin = CB (reacts rapidly in aqueous solution within 1 minute)
- Total bilirubin = reaction in methanol (both CB + UCB)
- Indirect bilirubin = Total minus Direct = UCB
Key Clinical Approach (Workup)
- History: Drug history, alcohol use, viral exposure, family history, pain (obstructive causes often painful), weight loss
- Examination: Scleral icterus (first sign), hepatomegaly, splenomegaly, stigmata of chronic liver disease, Courvoisier's sign (palpable non-tender gallbladder in malignant obstruction)
- Labs: LFTs (bilirubin, ALT, AST, ALP, GGT), albumin, PT/INR, CBC, peripheral smear, viral hepatitis markers, urine bilirubin & urobilinogen
- Imaging: Ultrasound (first-line to detect ductal dilatation), CT/MRCP (for extent and cause), ERCP (therapeutic)
Sources
- Biochemistry, Lippincott Illustrated Reviews, 8th ed., pp. 798-805
- Schwartz's Principles of Surgery, 11th ed., pp. 1381-1382
- Medical Physiology (Boron & Boulpaep), Chapter 46
- Goldman-Cecil Medicine, International Edition
Classification cause
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have rich data from multiple authoritative sources. Here is the detailed classification and causes of jaundice:
Classification and Causes of Jaundice
I. Classification Based on Bilirubin Type
| Type | Bilirubin Elevated | Also Called |
|---|---|---|
| Unconjugated hyperbilirubinemia | Indirect (UCB) | Acholuric jaundice (no bile in urine) |
| Conjugated hyperbilirubinemia | Direct (CB) | Choluric jaundice (bile pigments in urine) |
| Mixed | Both UCB + CB | Hepatocellular jaundice |
- Harper's Illustrated Biochemistry, 32nd ed.
II. Physiological (Anatomical) Classification
A. PREHEPATIC JAUNDICE (Unconjugated Hyperbilirubinemia)
Excess bilirubin production overwhelms hepatic conjugating capacity, or delivery to the liver is impaired.
1. Increased Production of UCB from Heme
Hemolysis - Hereditary:
- Hereditary spherocytosis
- G6PD deficiency
- Pyruvate kinase deficiency
- Sickle cell anemia
- Thalassemia
Hemolysis - Acquired:
- Immune-mediated: autoimmune hemolytic anemia, transfusion reactions, drugs (methyldopa, penicillin) - Coombs positive
- Non-immune: microangiopathic hemolytic anemia (TTP, HUS, DIC), prosthetic heart valves, infections (malaria, Clostridium), drugs/toxins directly damaging RBCs - Coombs negative
Ineffective erythropoiesis:
- Megaloblastic anemia (B12/folate deficiency)
- Sideroblastic anemia
- Thalassemia (intramedullary destruction)
Rapid RBC turnover: Physiological neonatal jaundice (high RBC mass at birth)
Other heme sources: Myoglobin (rhabdomyolysis), cytochrome turnover
2. Decreased Delivery of UCB to Hepatocyte
- Right-sided congestive heart failure
- Portocaval shunt
3. Decreased Uptake of UCB by Hepatocytes
- Competitive inhibition by drugs (rifampicin, flavaspidic acid)
- Gilbert's syndrome (mildly impaired uptake + conjugation)
- Sepsis, fasting
4. Decreased Storage in Cytosol (Reduced Ligandin/Y and Z proteins)
- Competitive inhibition
- Fever
B. HEPATIC (INTRAHEPATIC) JAUNDICE
Can be unconjugated (defective conjugation) or conjugated (defective secretion into bile) - often mixed.
1. Decreased Conjugation (Unconjugated Hyperbilirubinemia)
| Disorder | Mechanism |
|---|---|
| Gilbert's syndrome | Mildly reduced UGT1A1 activity; ~4-7% of population; benign; precipitated by fasting, illness, stress |
| Crigler-Najjar Type I | Complete UGT1A1 deficiency; severe unconjugated hyperbilirubinemia; kernicterus; often fatal without liver transplant |
| Crigler-Najjar Type II (Arias) | Partial UGT1A1 deficiency; less severe; responds to phenobarbital |
| Neonatal physiological jaundice | Immature UGT1A1 (reaches adult levels ~4 weeks); transient |
| Drugs | Inhibitors of UGT1A1 |
| Hepatocellular dysfunction | Cirrhosis, hepatitis |
2. Defective Secretion of CB into Bile Canaliculi (Conjugated Hyperbilirubinemia)
| Disorder | Mechanism |
|---|---|
| Dubin-Johnson syndrome | Deficiency of MRP2 (canalicular transport protein); conjugated hyperbilirubinemia; black pigment in liver; benign |
| Rotor syndrome | Similar to Dubin-Johnson but no liver pigment; gallbladder visible on cholecystography; benign |
| Drugs | Estradiol, oral contraceptives, anabolic steroids, cyclosporin |
3. Hepatocellular Disease (Mixed - Cholestatic + Conjugation Defect)
Viral hepatitis:
- Hepatitis A, B, C, D, E
- Epstein-Barr virus (EBV/infectious mononucleosis)
- Cytomegalovirus (CMV)
- Herpes simplex virus (HSV)
Toxic/Drug-induced:
- Dose-dependent (predictable): acetaminophen, alcohol
- Idiosyncratic (unpredictable): isoniazid, halothane, chlorpromazine
- Environmental toxins: vinyl chloride, pyrrolizidine alkaloids (Jamaica bush tea), wild mushrooms
Metabolic/Genetic liver diseases:
- Wilson's disease (copper accumulation - young adults)
- Hemochromatosis (iron overload)
- Alpha-1 antitrypsin deficiency
- Non-alcoholic fatty liver disease (NAFLD/NASH)
Autoimmune: Autoimmune hepatitis, primary biliary cirrhosis (PBC), primary sclerosing cholangitis (PSC)
Cirrhosis (end-stage from any cause)
Ischemic hepatitis: "Shock liver" from hypoperfusion, right heart failure, Budd-Chiari syndrome
Infiltrative disorders: Amyloidosis, sarcoidosis, lymphoma, metastatic carcinoma
Pregnancy-related:
- Acute fatty liver of pregnancy
- Intrahepatic cholestasis of pregnancy
- HELLP syndrome (hemolysis, elevated liver enzymes, low platelets)
Others: Sepsis, TPN-related jaundice, post-bone marrow transplant (veno-occlusive disease / sinusoidal obstruction syndrome, graft-versus-host disease)
C. POSTHEPATIC (EXTRAHEPATIC OBSTRUCTIVE) JAUNDICE (Conjugated Hyperbilirubinemia)
Obstruction of bile flow from liver to duodenum at any point in the biliary tree.
1. Intraluminal (within the duct)
- Choledocholithiasis (common bile duct stones) - most common benign cause
- Parasites (Ascaris, liver flukes - Clonorchis, Fasciola)
- Blood clots (hemobilia)
2. Mural (wall of the duct)
- Malignant:
- Cholangiocarcinoma (Klatskin tumor at hilum)
- Carcinoma of ampulla of Vater
- Carcinoma of gallbladder
- Benign:
- Primary sclerosing cholangitis (PSC)
- Benign biliary strictures (post-surgical, post-traumatic)
- Biliary atresia (neonates)
- Cholangitis (bacterial infection of bile duct)
- Disorders of the papilla of Vater
3. Extrinsic Compression
- Pancreatic carcinoma (head of pancreas) - most common malignant cause of obstructive jaundice
- Chronic pancreatitis / pancreatitis / pseudocysts
- Lymph node enlargement in porta hepatis (lymphoma, metastatic nodes)
- Mirizzi syndrome (gallstone in cystic duct compressing common hepatic duct)
4. Iatrogenic / Post-Surgical
- Accidental bile duct ligation or clipping
- Bile duct ischemia
- Retained stones post-cholecystectomy
- Post-anastomotic strictures
III. Classification Based on Age Group
Neonatal Causes
| Unconjugated | Conjugated |
|---|---|
| Physiological (most common) | Biliary atresia |
| Breast milk jaundice | Neonatal hepatitis |
| Hemolytic disease of newborn (Rh/ABO incompatibility) | Choledochal cyst |
| G6PD deficiency | Total parenteral nutrition (TPN) |
| Crigler-Najjar syndrome | Alagille syndrome (bile duct paucity) |
| Congenital hypothyroidism | Galactosaemia, tyrosinemia |
| Cephalhematoma (extravasated blood) | Sepsis |
Tietz Textbook of Laboratory Medicine, 7th ed.; Harrison's Principles of Internal Medicine, 22nd ed.
IV. Quick Causes Summary by Bilirubin Type
Unconjugated (Indirect) Hyperbilirubinemia - causes:
- Hemolytic anemias (hereditary + acquired)
- Ineffective erythropoiesis
- Neonatal jaundice
- Gilbert's syndrome
- Crigler-Najjar Types I and II
- Toxic hyperbilirubinemia
Conjugated (Direct) Hyperbilirubinemia - causes:
- Obstruction of biliary tree (stones, carcinoma, strictures)
- Dubin-Johnson syndrome
- Rotor syndrome
- Liver diseases (hepatitis, cirrhosis, cholestasis)
Harper's Illustrated Biochemistry, 32nd ed., Table 31-3; Tietz Textbook of Laboratory Medicine, 7th ed., Box 51.2; Harrison's Principles of Internal Medicine, 22nd ed.
This is a shared conversation. Sign in to Orris to start your own chat.