Gross anatomy of breast and axillary lymph nodes
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of the gross anatomy of the breast and axillary lymph nodes, drawn from Sabiston's Textbook of Surgery, Fischer's Mastery of Surgery, Gray's Anatomy for Students, and the THIEME Atlas.
Gross Anatomy of the Breast and Axillary Lymph Nodes
1. Position and Surface Anatomy
The female breast sits on the anterior thoracic wall, between ribs II and VI in the midclavicular line. It overlies three muscles: pectoralis major (central and medial), serratus anterior (lateral), and external oblique (inferolateral). A superolateral tongue of glandular tissue, the axillary tail (axillary process), extends around the lower margin of the pectoralis major to enter the axilla - this is clinically relevant because it may be palpated in the axilla and may harbor tumors.
- Gray's Anatomy for Students
2. Structural Layers (Deep to Superficial)
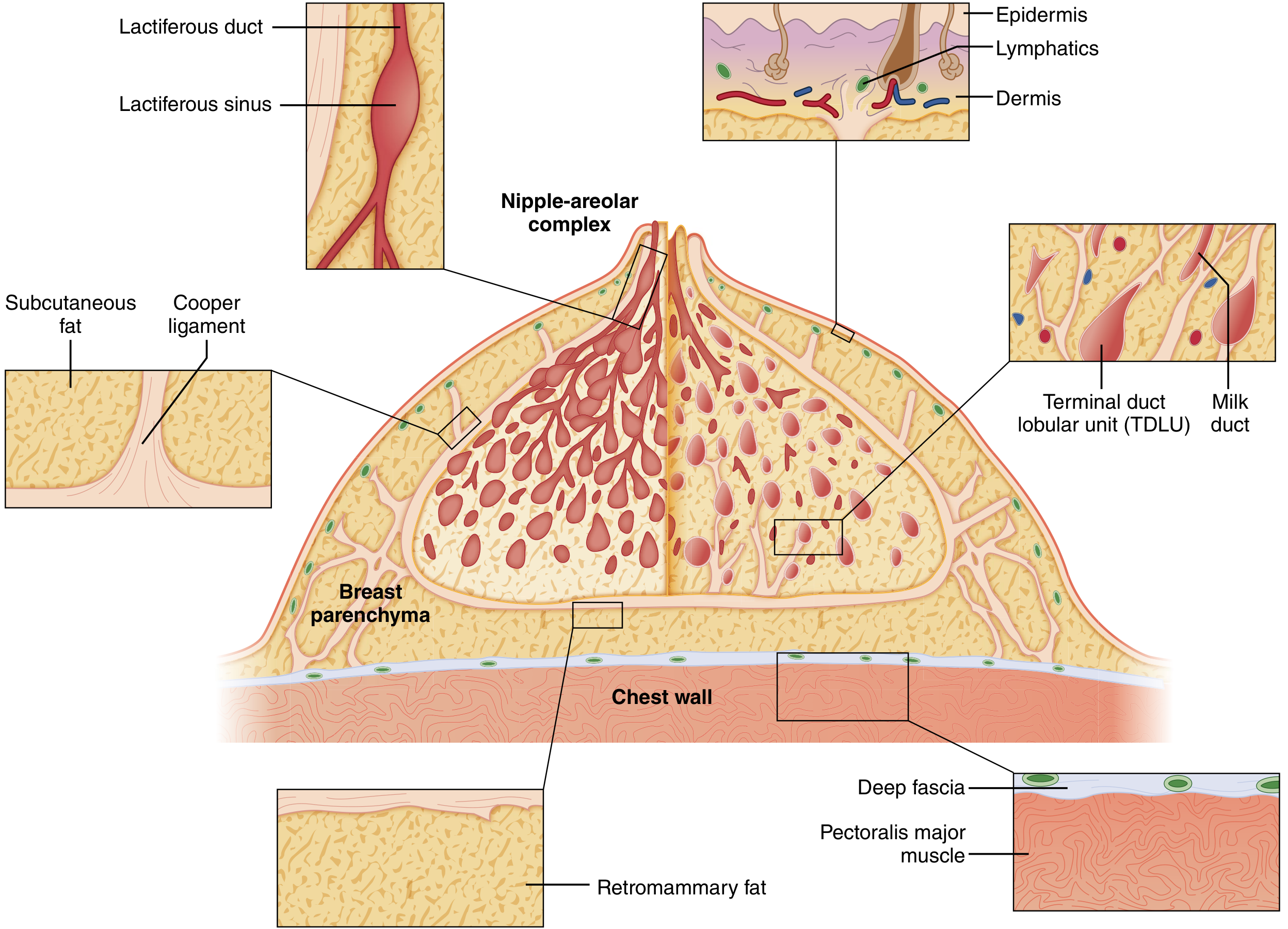
The breast is composed of three principal tissue types:
- Glandular epithelium - the functional secretory tissue
- Fibrous stroma - provides structural support
- Adipose tissue - surrounds and cushions the gland
It lies between:
-
Anteriorly: skin and subcutaneous fat
-
Posteriorly: superficial pectoral fascia and pectoralis major; a potential retromammary space lies between the deep breast surface and the pectoral fascia, allowing the breast to move
-
Sabiston Textbook of Surgery
3. Suspensory Ligaments of Cooper
Multiple fibrous bands - Cooper's ligaments - run between the deep fascia of the chest wall and the dermis, anchoring the breast and giving it shape. When tumors infiltrate these ligaments or cause edema:
-
Traction produces skin dimpling
-
Dermal lymphatic blockage produces peau d'orange (orange-peel skin appearance)
-
Sabiston Textbook of Surgery
4. Ductal System and Lobular Unit
The glandular apparatus is arranged in a radial, tree-like pattern spreading from the nipple-areolar complex (NAC):
- 15-20 lobes per breast, each draining via a lactiferous duct opening at the nipple
- Each duct has a dilated segment beneath the NAC: the lactiferous sinus
- Ducts progressively branch, ending in terminal ductules (acini)
- The terminal duct lobular unit (TDLU) = one lobule + its terminal duct - the basic secretory unit and the site where most malignant breast tumors originate
The ductal epithelium is surrounded by contractile myoepithelial cells, outside which lies a continuous basement membrane (laminin, type IV collagen). Invasion through this membrane defines the transition from DCIS to invasive carcinoma.
- Sabiston Textbook of Surgery; THIEME Atlas
5. Blood Supply
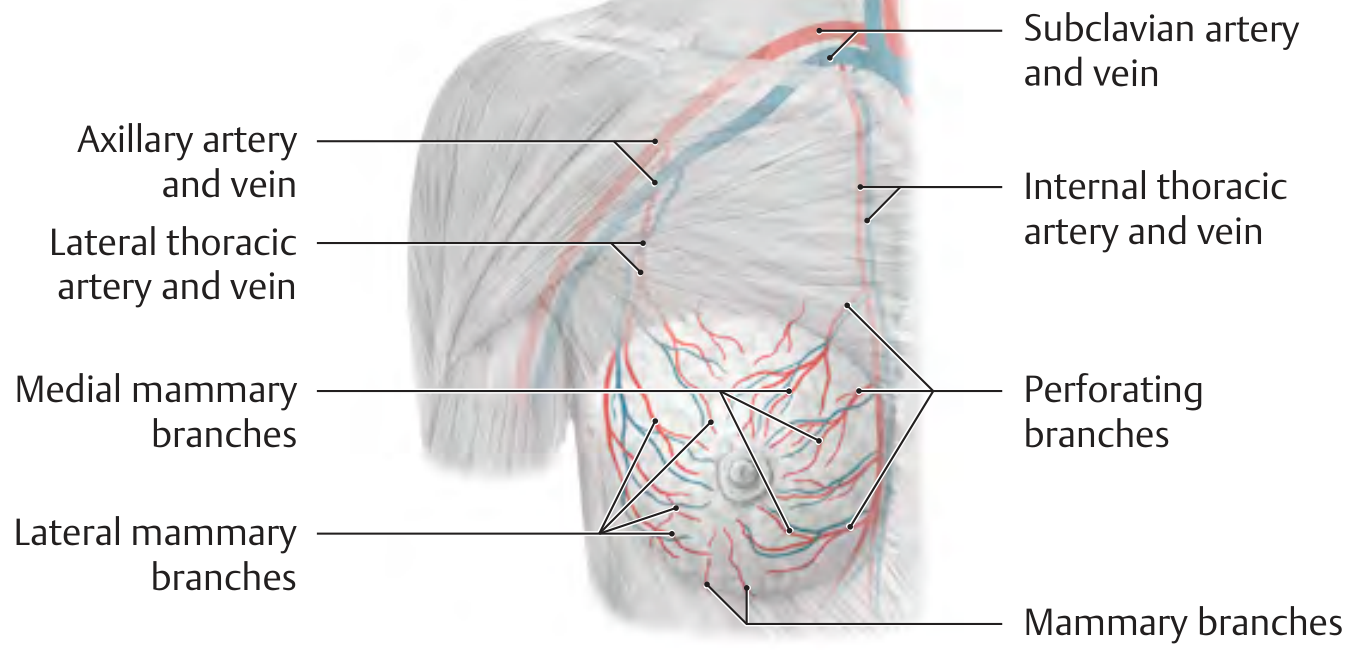
The breast receives blood from three sources:
| Source | Branches | Region supplied |
|---|---|---|
| Internal thoracic (mammary) artery | Perforating branches (2nd-4th intercostal spaces) - medial mammary branches | Medial breast (major contributor, ~60%) |
| Lateral thoracic artery | Lateral mammary branches | Lateral and superior breast |
| Intercostal arteries (2nd-5th) | Mammary branches | Direct branches to parenchyma |
Venous drainage mirrors the arterial supply via internal thoracic veins and lateral thoracic veins, ultimately draining to the axillary and subclavian veins.
- THIEME Atlas of Anatomy; Fischer's Mastery of Surgery
6. Nerve Supply
The breast has segmental sensory innervation from branches of the 2nd-6th intercostal nerves (medial and lateral mammary branches). The supraclavicular nerves (cervical plexus, C3-C4) supply the upper and anterior breast. The nipple is primarily supplied by the lateral cutaneous branch of T4.
- THIEME Atlas of Anatomy
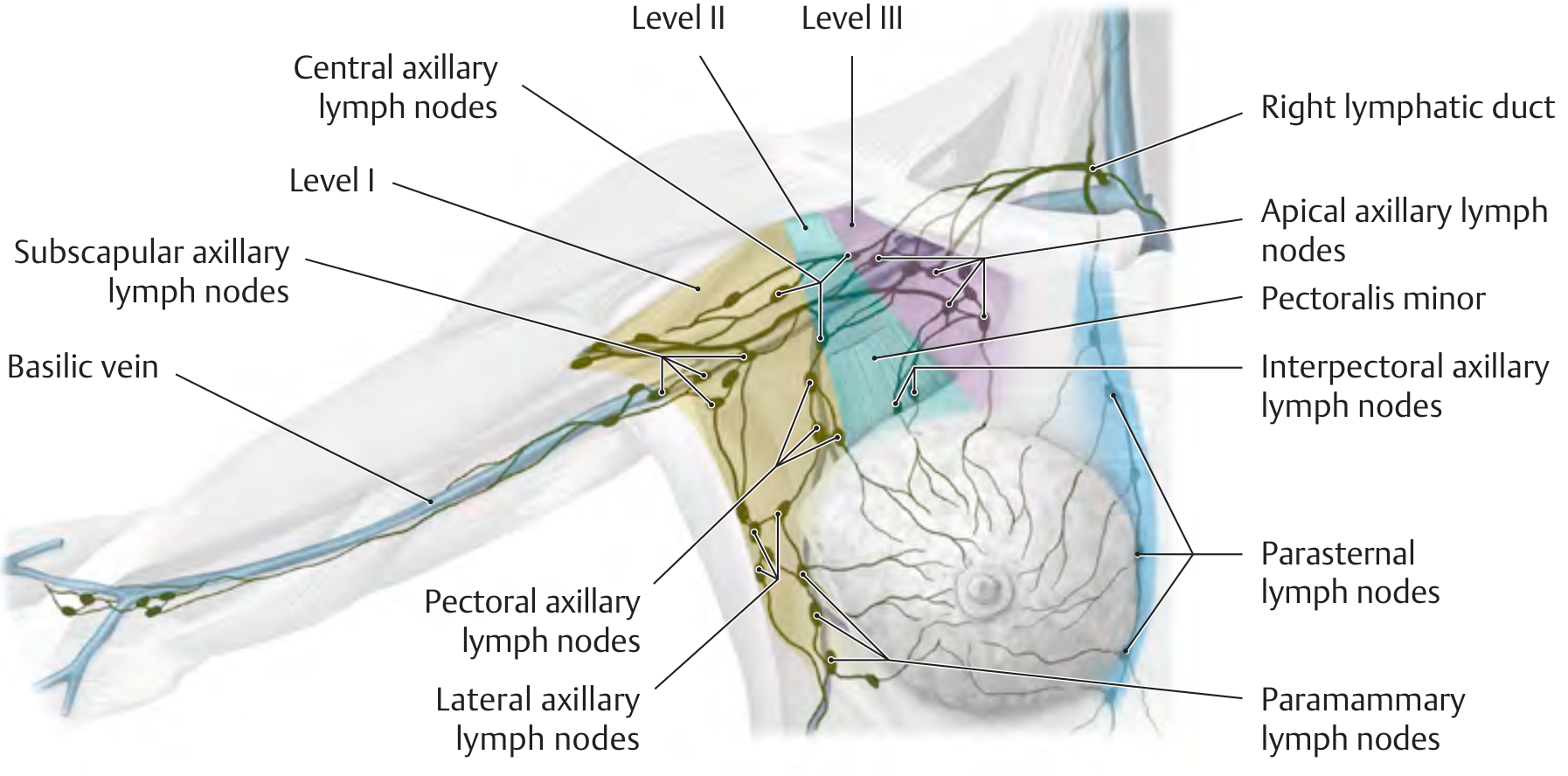
7. Lymphatic Drainage
The lymphatic system is a primary route of breast cancer metastasis. Lymphatic channels are abundant in both the breast parenchyma and the dermis.
Subareolar (Sappey's) Plexus
Specialized lymphatics collect under the nipple-areola to form Sappey's plexus (described 1885). Lymph flows from the skin into this plexus and then into the interlobular lymphatics of the parenchyma. This plexus is the basis for successful sentinel lymph node mapping.
Routes of Drainage
-
70-80% drains to the axillary lymph nodes (primary route)
-
~20% drains to internal mammary lymph nodes as a secondary route
-
Internal mammary nodes are the predominant drainage in 2-3% of patients
-
Minor drainage through the pectoralis muscle to medial lymph node groups
-
The lower inner quadrant drains via a plexus over the rectus sheath that can communicate with the subperitoneal plexus (explaining rare Krukenberg's tumor metastasis to the ovary)
-
Sabiston Textbook of Surgery; S. Das Manual on Clinical Surgery
8. Axillary Lymph Nodes - Levels and Groups
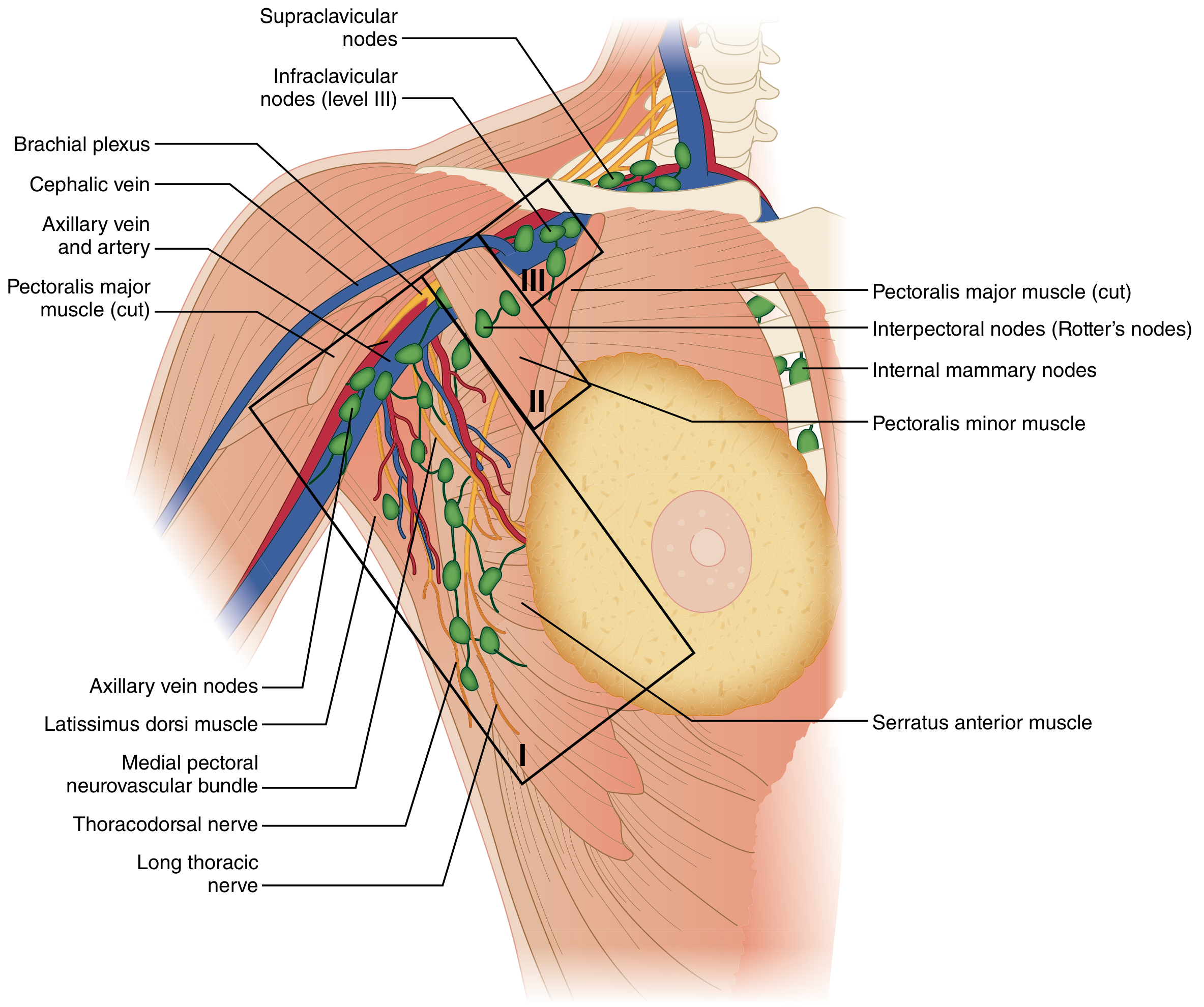
The axillary nodes are classified into three surgical levels based on their relationship to the pectoralis minor muscle:
Level I - Lower Axillary Group (lateral to pectoralis minor)
| Node Group | Location | Notes |
|---|---|---|
| Pectoral (anterior/external mammary) | Deep to lateral edge of pectoralis major; along lateral thoracic artery | First nodes to receive breast lymphatics; functionally the sentinel node is usually here |
| Subscapular (posterior) | Along subscapular vessels and thoracodorsal branches | Intercostobrachial and thoracodorsal nerves pass through |
| Lateral (humeral/axillary vein) | Along axillary vein, from tendon of latissimus dorsi to thoracoacromial vein | Receive most lymphatics from upper extremity |
| Paramammary | Along the lateral breast border |
Level II - Middle Axillary Group (along/posterior to pectoralis minor)
| Node Group | Location | Notes |
|---|---|---|
| Central | Fat in central axilla, ~midway between anterior and posterior folds | May lie subcutaneously; drain to apical nodes |
| Interpectoral (Rotter's nodes) | Areolar tissue between pectoralis major and clavipectoral fascia | Associated with pectoral branches of thoracoacromial artery |
Level III - Upper Infraclavicular Group (medial to pectoralis minor)
| Node Group | Location | Notes |
|---|---|---|
| Apical (infraclavicular) | Along axillary vein proximal to thoracoacromial vein; posterior to subclavius | Receive all other axillary node drainage; efferent drains to inferior deep cervical nodes or venous angle (junction of internal jugular and subclavian veins) |
After level III, drainage continues to supraclavicular nodes (considered outside the anatomic boundaries of the axilla).
- Sabiston Textbook of Surgery; Fischer's Mastery of Surgery; THIEME Atlas
9. Surgical Boundaries and Key Nerves of the Axilla
The surgical axilla is bounded by:
- Medially: serratus anterior muscle and chest wall
- Posteriorly: latissimus dorsi, teres major, subscapularis
- Anteriorly: pectoralis major and minor
- Superiorly: axillary vein (which becomes the subclavian vein at the costoclavicular/Halsted's ligament - the apex of the axilla)
Three Nerves Critical to Preserve During Axillary Dissection
| Nerve | Origin | Innervation | Injury consequence |
|---|---|---|---|
| Long thoracic nerve (nerve of Bell) | C5-C7 roots | Serratus anterior | Winged scapula |
| Thoracodorsal nerve | Posterior cord, brachial plexus | Latissimus dorsi | Weak shoulder extension/adduction |
| Medial pectoral nerve | Medial cord, brachial plexus | Pectoralis major (and minor) | Atrophy of pectoralis major; also a landmark for the axillary vein (just cephalad and deep to the medial pectoral neurovascular bundle) |
Additionally, 3-5 intercostobrachial nerves cross the axilla horizontally, supplying sensation to the upper inner arm and posterior axillary skin. Division causes numbness and occasionally chronic pain in that distribution.
- Sabiston Textbook of Surgery; Fischer's Mastery of Surgery
10. Clinical Correlates
| Finding | Anatomical Basis |
|---|---|
| Peau d'orange | Tumor emboli blocking dermal lymphatics |
| Skin dimpling | Cooper's ligament traction by scirrhous tumor |
| Winged scapula post-mastectomy | Long thoracic nerve injury |
| Lymphedema post-ALND | Disruption of upper limb lymphatics draining via axillary vein region |
| Axillary tail mistaken for lymph node | Extension of breast parenchyma into axilla |
| Sentinel lymph node usually in Level I | External mammary/pectoral group receives first breast lymphatics |
Sources: Sabiston Textbook of Surgery (Fig. 68.1, 68.4, 68.5); Fischer's Mastery of Surgery (Ch. 57); THIEME Atlas of General Anatomy & Musculoskeletal System; Gray's Anatomy for Students; S. Das Manual on Clinical Surgery
Formation and relations of the brachial plexus, cutaneal supplies/dermatome of upper limb w.r.t. MS1 level. Netter's atlas diagram and suitable textbooks
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Searching the Web
Netter's Atlas brachial plexus formation diagram plate number
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the material needed for a thorough MS1-level response. Here is the complete, well-structured answer:
Brachial Plexus: Formation, Relations, Branches, and Cutaneous Supply of the Upper Limb
Sources: Gray's Anatomy for Students (Moore & Dalley), THIEME Atlas of General Anatomy & Musculoskeletal System, Fischer's Mastery of Surgery
1. Formation - The Basics
The brachial plexus is a somatic nerve plexus formed by the anterior rami (ventral rami) of C5, C6, C7, C8, and T1. It is organized into five sequential parts from proximal to distal:
Mnemonic: "Real Teenagers Drink Cold Beer" - Roots → Trunks → Divisions → Cords → Branches

(Gray's Anatomy for Students, Fig. 7.52A - Major components in the neck and axilla)
2. Parts of the Brachial Plexus
Roots (C5-T1)
- The roots pass between the anterior scalene and middle scalene muscles in the posterior triangle of the neck.
- They lie superior and posterior to the subclavian artery.
- Each root receives gray rami communicantes from the sympathetic trunk, carrying postganglionic sympathetic fibers to the periphery.
Trunks (3)
The roots unite to form three trunks that cross over rib I to enter the axilla:
| Trunk | Formed by | Position |
|---|---|---|
| Superior (upper) | C5 + C6 | Most superior |
| Middle | C7 alone | Intermediate |
| Inferior (lower) | C8 + T1 | Lies on rib I, posterior to subclavian artery |
Divisions (6)
Each trunk divides into an anterior and a posterior division (6 total). No peripheral nerves arise directly from the divisions.
- Anterior divisions → supply flexor (anterior) compartments
- Posterior divisions → supply extensor (posterior) compartments
Cords (3) - Named by their position relative to the 2nd part of the axillary artery
| Cord | Formed from | Roots | Position |
|---|---|---|---|
| Lateral | Anterior divisions of superior + middle trunks | C5-C7 | Lateral to axillary artery |
| Medial | Anterior division of inferior trunk | C8-T1 | Medial to axillary artery |
| Posterior | All three posterior divisions | C5-T1 | Posterior to axillary artery |
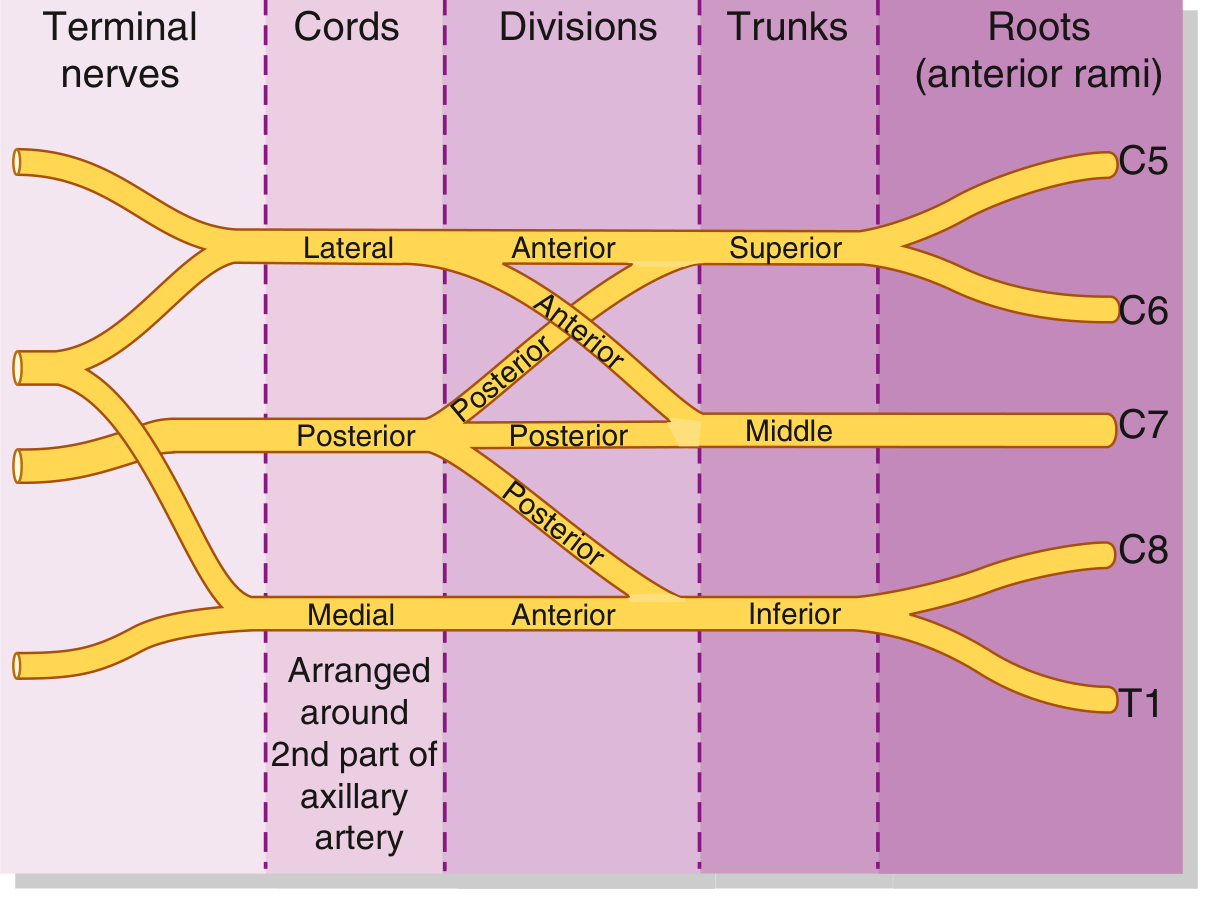
(Gray's Anatomy for Students, Fig. 7.52B - Schematic)
3. Relations
In the Neck (posterior triangle)
- Roots/trunks pass between anterior and middle scalene muscles
- The plexus lies posterior and superior to the subclavian artery
- The inferior trunk lies directly on rib I, behind the subclavian artery (clinically: a cervical rib or Pancoast tumor at the lung apex may compress the inferior trunk → Klumpke's palsy pattern)
In the Axilla
- Cords surround the axillary artery (named for their positions relative to its 2nd part)
- The pectoralis minor muscle is the key landmark:
- Level I nodes (and lateral cord) = lateral to pectoralis minor
- Level II (posterior cord) = at the level of pectoralis minor
- Level III (medial cord/apical nodes) = medial to pectoralis minor
- The musculocutaneous nerve, lateral root of median, median nerve, medial root of median, and ulnar nerve form an "M" shape over the 3rd part of the axillary artery - a useful intraoperative landmark
4. Branches - Complete Table
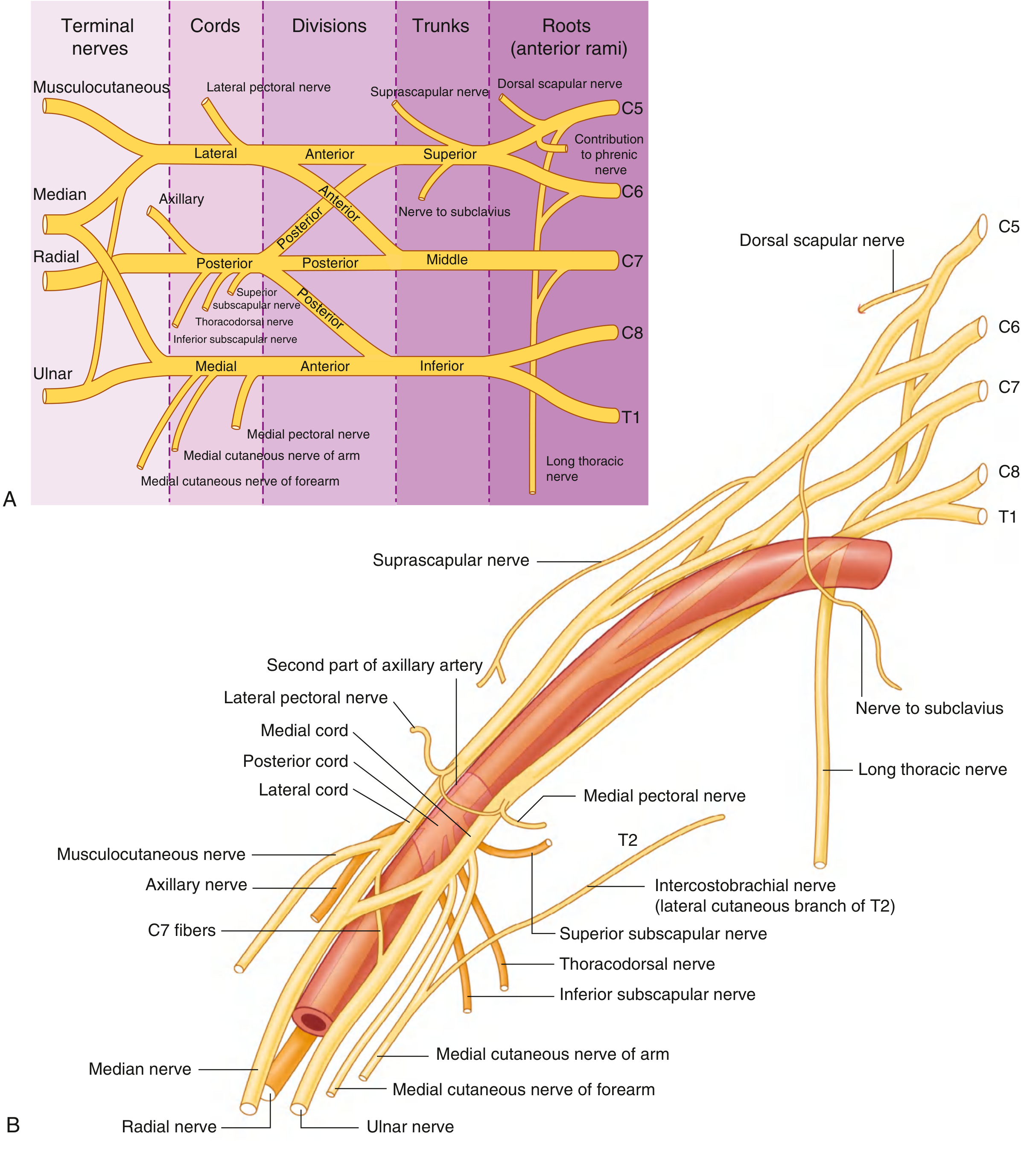
(Gray's Anatomy for Students, Fig. 7.53 - Brachial plexus branches and relationship to axillary artery)
From the Roots
| Nerve | Root | Target |
|---|---|---|
| Dorsal scapular | C5 | Rhomboid major, rhomboid minor |
| Long thoracic | C5, C6, C7 | Serratus anterior (injury = winged scapula) |
| C5 contribution | C5 | Phrenic nerve |
From the Trunks (both from superior trunk only)
| Nerve | Root | Target |
|---|---|---|
| Suprascapular | C5, C6 | Supraspinatus, infraspinatus |
| Nerve to subclavius | C5, C6 | Subclavius muscle |
From the Lateral Cord (C5-C7)
| Nerve | Target/Function |
|---|---|
| Lateral pectoral nerve | Pectoralis major (clavicular head) |
| Musculocutaneous nerve | Coracobrachialis, biceps, brachialis; terminates as lateral cutaneous nerve of forearm (sensory to lateral forearm) |
| Lateral root of median nerve | Joins medial root to form median nerve |
From the Medial Cord (C8-T1)
| Nerve | Target/Function |
|---|---|
| Medial pectoral nerve | Pectoralis minor + sternocostal head of pectoralis major |
| Medial cutaneous nerve of the arm | Skin - medial distal 1/3 of arm |
| Medial cutaneous nerve of the forearm | Skin - medial (ulnar) side of forearm to wrist |
| Medial root of median nerve | Joins lateral root to form median nerve |
| Ulnar nerve | FCU, medial half FDP; all intrinsic hand muscles except 3 thenar + 2 lateral lumbricals; skin - medial 1.5 digits (palmar + dorsal), medial palm |
From the Posterior Cord (C5-T1)
| Nerve | Target/Function |
|---|---|
| Superior subscapular | Subscapularis |
| Thoracodorsal | Latissimus dorsi |
| Inferior subscapular | Subscapularis + teres major |
| Axillary nerve | Deltoid + teres minor; superior lateral cutaneous nerve of arm (sensory to deltoid patch, "regimental badge area") |
| Radial nerve | All posterior compartment muscles of arm and forearm; sensory to posterior arm, posterior forearm, and dorsal lateral hand + dorsal aspect of lateral 3.5 digits |
5. Terminal Nerves - Summary (Netter's Atlas Plate reference: Plate 401-410, 7th edition)
Note: Netter's Atlas of Human Anatomy covers the brachial plexus schema at Plates 401-402 (Brachial Plexus Schema), with cutaneous nerves of the upper limb at Plates 462-465 in the 7th edition. The key Netter plates for MS1 study are:
- Plate 401: Brachial plexus schema (roots → terminal nerves)
- Plate 462-463: Cutaneous innervation of upper limb (anterior/posterior)
- Plate 464-465: Dermatomes of upper limb
6. Cutaneous (Peripheral) Nerve Supply of the Upper Limb
Anterior View
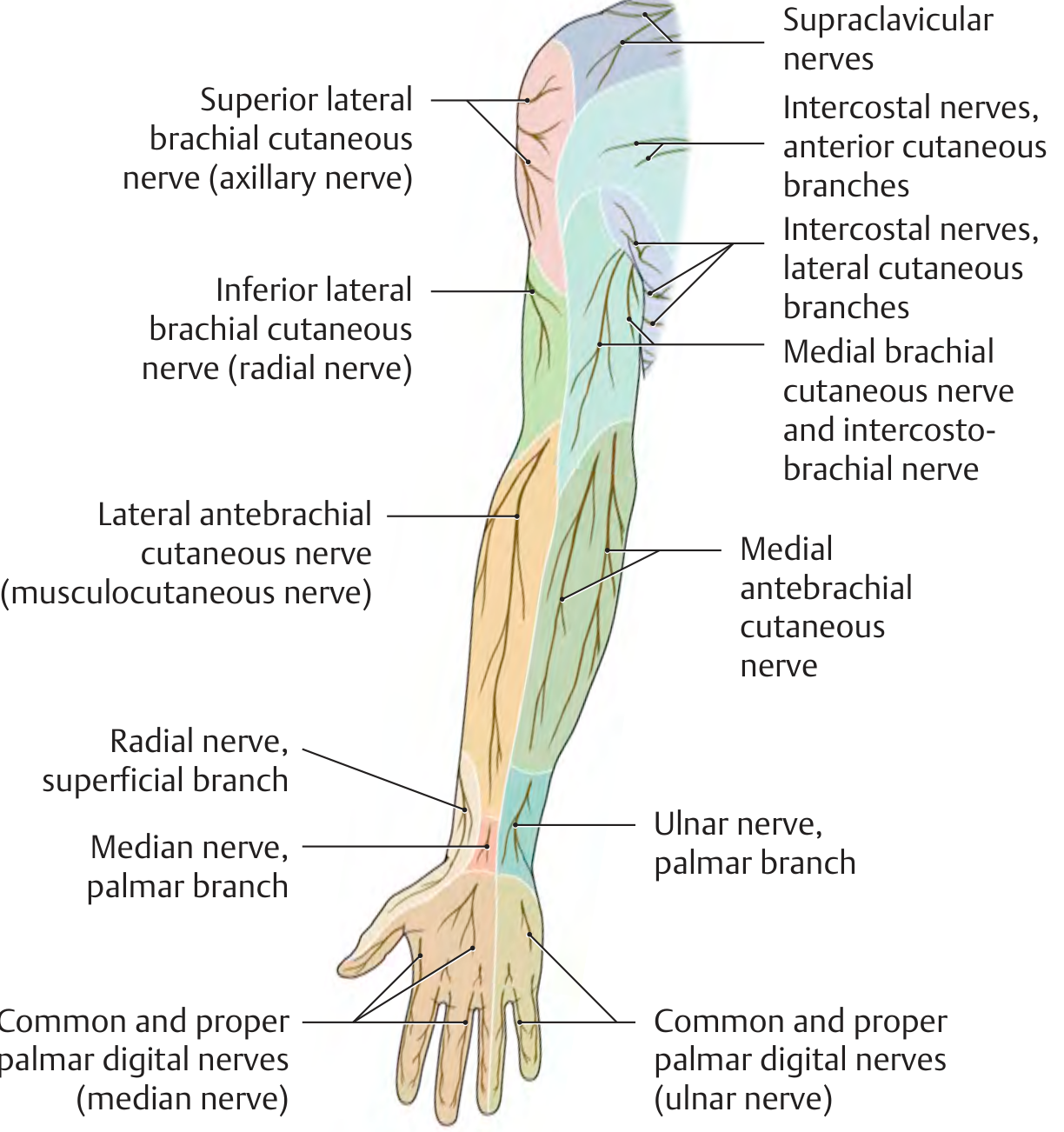
(THIEME Atlas, Fig. 5.1D - Anterior view peripheral cutaneous innervation)
Posterior View
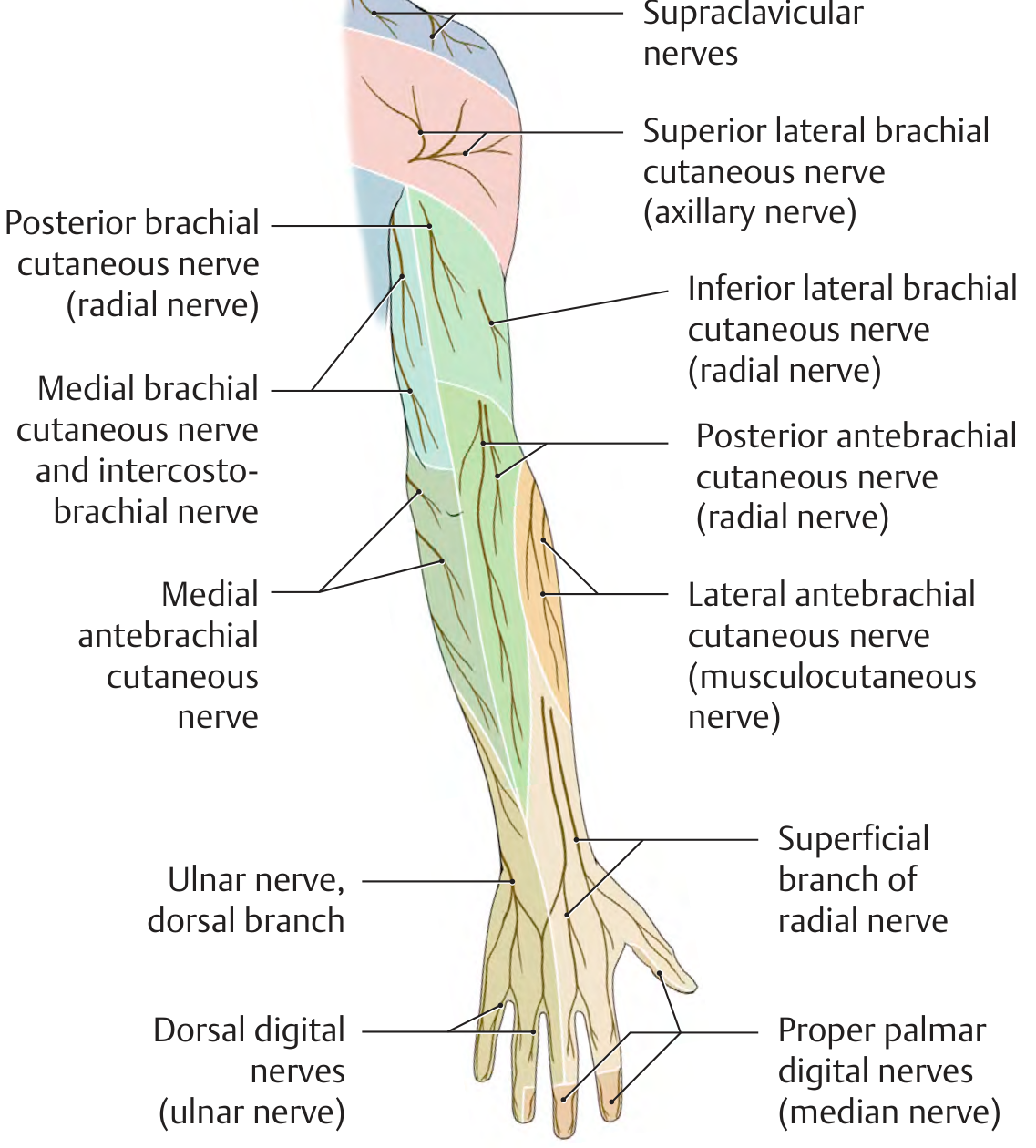
(THIEME Atlas, Fig. 5.2F - Posterior view peripheral cutaneous innervation)
7. Dermatomes of the Upper Limb (Radicular/Segmental Innervation)
Key dermatome map (from THIEME Atlas):
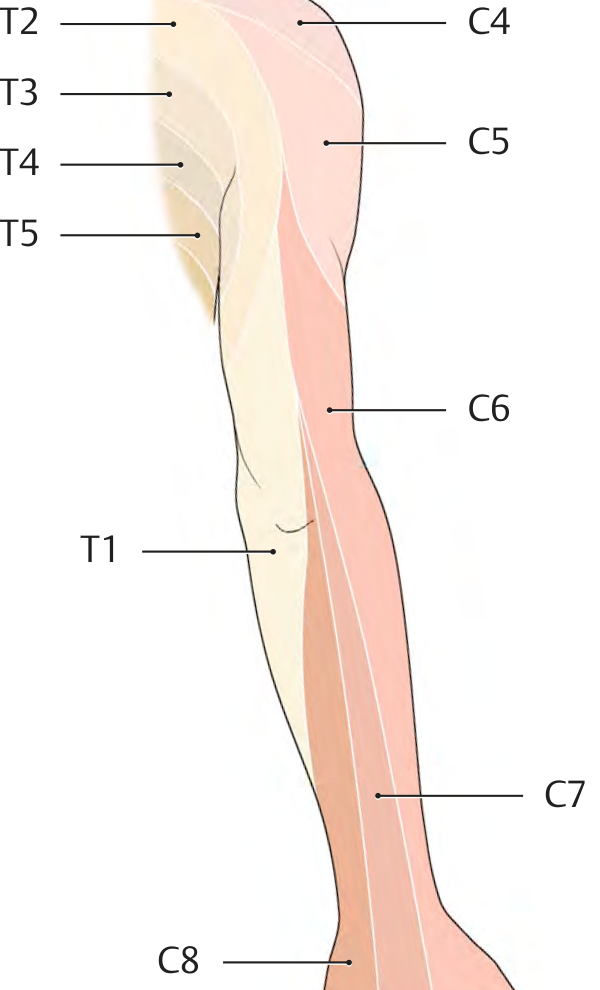
(THIEME Atlas - Posterior dermatomes C4-T5; note how C5-C7 become separated from the thoracic body wall)
With limb outgrowth during development, the sensory segments become elongated into narrow longitudinal bands. Segments C5-C7 become separated from the body wall as the limb buds out:
| Spinal Level | Dermatome Area |
|---|---|
| C4 | Shoulder cap (over deltoid/trapezius) |
| C5 | Lateral arm (deltoid patch, lateral upper arm) |
| C6 | Lateral forearm, thumb, index finger |
| C7 | Middle finger (autonomous zone); posterior forearm |
| C8 | Ring and little fingers, medial forearm |
| T1 | Medial arm (proximal part, near axilla) |
| T2 | Axilla, upper medial arm (intercostobrachial nerve) |
Important Distinctions for MS1:
-
Dermatome (radicular) vs. peripheral cutaneous territory - these are NOT the same. A single peripheral nerve may carry fibers from multiple roots. Injury to a nerve root (e.g., disc herniation at C6) produces a dermatome-shaped sensory loss. Injury to a peripheral nerve (e.g., median nerve at wrist) produces a peripheral territory loss.
-
Autonomous zones (minimal overlap, reliable for testing):
- C6 = tip of index finger
- C7 = tip of middle finger
- C8 = tip of little finger
- Axillary nerve = regimental badge area (lateral deltoid)
- Radial nerve = dorsal first web space
- Median nerve = tip of index finger (palmar)
- Ulnar nerve = tip of little finger
8. Full Body Peripheral Cutaneous Innervation (Including Upper Limb)
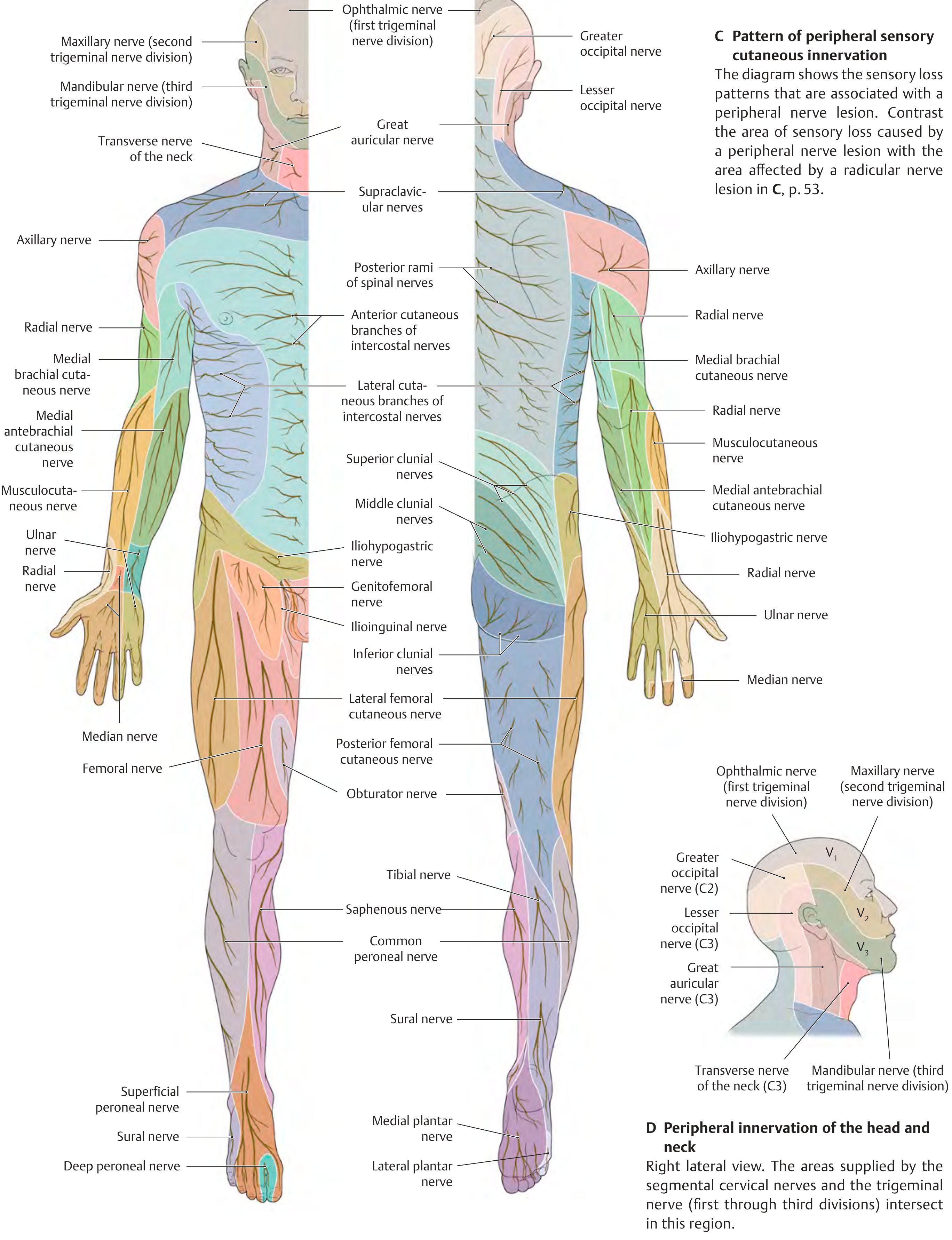
(THIEME Atlas - Whole body peripheral cutaneous innervation, anterior and posterior)
9. Clinical Correlates (MS1 High-Yield)
| Injury | Mechanism | Deficit |
|---|---|---|
| Erb's palsy (C5-C6) | Upper plexus - shoulder dystocia, lateral neck stretching | "Waiter's tip" - arm adducted, internally rotated, forearm pronated; loss of shoulder abduction/flexion, elbow flexion |
| Klumpke's palsy (C8-T1) | Lower plexus - arm pulled superiorly, Pancoast tumor | Claw hand (intrinsics lost), Horner's syndrome if T1 sympathetics involved |
| Long thoracic nerve (C5-7) | Axillary dissection, carrying heavy loads on shoulder | Winged scapula |
| Axillary nerve | Surgical neck humerus fracture, shoulder dislocation | Deltoid paralysis (shoulder abduction lost after 15°), sensory loss over regimental badge area |
| Radial nerve | Midshaft humerus fracture in spiral groove | Wrist drop (posterior interosseous), sensory loss dorsal lateral hand |
| Median nerve at wrist | Carpal tunnel syndrome | Thenar wasting, sensory loss lateral 3.5 digits (palmar) |
| Ulnar nerve at elbow | Cubital tunnel | Claw hand (ring + little), sensory medial 1.5 digits |
Sources used:
- Gray's Anatomy for Students (Moore, Dalley, Agur) - Figs. 7.52-7.56, Table 7.7
- THIEME Atlas of General Anatomy and Musculoskeletal System - pp. 106-108, 229, 396-398
- Netter's Atlas of Human Anatomy (7th ed): Plates 401-402 (brachial plexus schema), 462-465 (cutaneous/dermatomes upper limb) - the standard MS1 reference for visual plate study
This is a shared conversation. Sign in to Orris to start your own chat.