Teach me about acute dacryocystitis
Reading File
Finding Sources
Searching PubMed
acute dacryocystitis
Searching Images
acute dacryocystitis lacrimal sac infection
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have all the information needed for a comprehensive teaching response. Let me compose it.
Acute Dacryocystitis
Anatomy & Pathophysiology
The lacrimal drainage system runs from the puncta → canaliculi → lacrimal sac → nasolacrimal duct → inferior meatus of the nose. Acute dacryocystitis is infection of the lacrimal sac, almost always secondary to nasolacrimal duct obstruction (NLDO). When outflow is blocked, stagnant tears create a reservoir for bacterial proliferation.
Less common causes of obstruction include:
- Lacrimal sac diverticula or dacryoliths
- Nasal/sinus surgery or trauma
- Rarely, lacrimal sac tumors
Epidemiology
- Bimodal distribution: neonates/infants (congenital NLDO, often from an imperforate valve of Hasner) and middle-aged to older adults (acquired NLDO, more common in women)
- In children, dacryocystitis frequently follows a viral upper respiratory infection
Microbiology
| Organism | Notes |
|---|---|
| Staphylococcus aureus | Most common overall |
| Streptococcus pneumoniae | Common in adults and children |
| Haemophilus influenzae | More common in children (chocolate agar for culture) |
| Gram-negative / atypical organisms | More common in diabetics, immunocompromised, and nursing home patients |
| MRSA | Consider in healthcare exposure, prior MRSA history |
Clinical Presentation
Symptoms:
- Subacute onset of pain and tenderness at the medial canthus
- Epiphora (tearing)
- Discharge (mucopurulent)
- Fever or chills in more severe cases
Signs:
- Erythematous, tender, tense swelling below the medial canthal tendon (critical anatomical landmark)
- Mucoid or purulent discharge expressible from the punctum on pressure over the lacrimal sac
- May progress to frank abscess formation
- Associated preseptal cellulitis may develop
- Rare: orbital cellulitis, skin fistula
Key pearl: Swelling is below the medial canthal tendon. If above — suspect lacrimal sac tumor or frontal sinus mucocele.
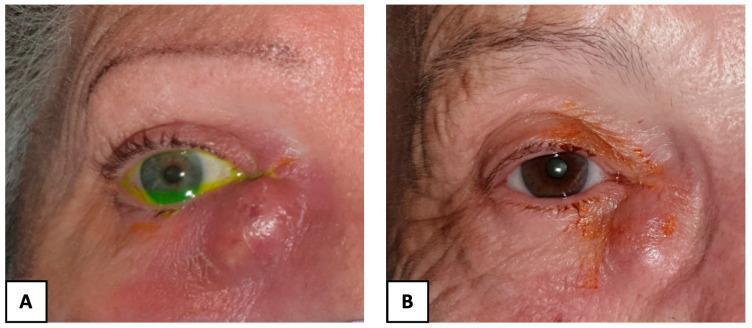
Clinical photos (A) acute dacryocystitis with abscess and purulent discharge; (B) chronic dacryocystitis with localized swelling and crusting
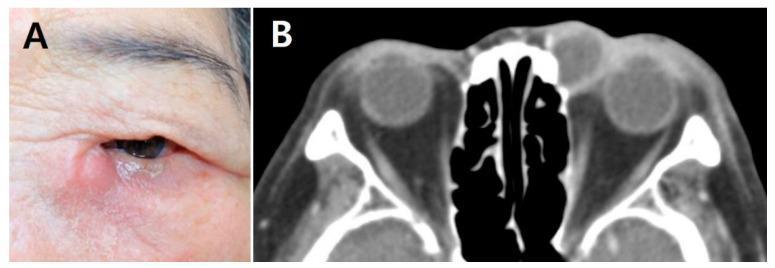
Clinical appearance (A) and contrast-enhanced axial CT (B) showing rim-enhancing lacrimal sac abscess with periorbital inflammation
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Facial/preseptal cellulitis | No discharge from punctum on pressure; patent lacrimal irrigation |
| Acute ethmoid sinusitis | Pain/erythema over nasal bone just medial to inner canthus; imaging diagnostic |
| Frontal sinus mucocele | Swelling above medial canthal tendon; proptosis and globe displacement |
| Lacrimal sac tumor | Mass above medial canthal tendon; no acute inflammatory signs |
| Dacryocystocele (infants) | Bluish, non-inflamed swelling; present from birth |
Workup
- History — prior episodes, sinus disease, trauma, surgery, immune status
- Physical exam — apply gentle pressure with a cotton-tipped swab over the lacrimal sac to express discharge from the punctum; examine contralateral eye too
- Gram stain and culture of expressed discharge — blood agar ± chocolate agar (children)
- Evaluate for orbital signs — pupils, extraocular motility, proptosis, vision
- CT orbits and paranasal sinuses — for severe/atypical cases, no response to antibiotics, or suspected orbital extension
Do NOT probe or irrigate the lacrimal system during the acute phase — this risks spreading the infection.
Treatment
Outpatient (Afebrile, systemically well, mild–moderate)
| Patient | First-line | MRSA-suspected |
|---|---|---|
| Adults | Cephalexin 500 mg PO q6h or amoxicillin/clavulanate 875/125 mg PO BID | TMP-SMX 160/800 mg PO q12h or clindamycin 300 mg PO TID |
| Children | Amoxicillin/clavulanate 25–45 mg/kg/d PO in 2 divided doses (max 90 mg/kg/d) | — |
- Warm compresses and gentle massage to the inner canthal region 5–10 min QID
- Topical antibiotics (e.g., trimethoprim/polymyxin B QID) as adjunct — topical alone is inadequate
- Analgesia (acetaminophen ± codeine) PRN
- Follow up daily until improvement confirmed
Inpatient (Febrile, acutely ill, or unreliable follow-up)
- Adults: Cefazolin 1 g IV q8h
- Children: Cefuroxime 50–100 mg/kg/d IV in 3 divided doses (ID consult)
- Alternative (penicillin allergy): Clindamycin 10 mg/kg IV q6h
- Vancomycin if MRSA suspected
- Adjust based on culture/sensitivity; step down to oral after clinical improvement
- Total course: 10–14 days
Abscess Management
- Incision and drainage if pus is pointing / about to drain spontaneously
- Risk: persistent sac-skin fistula (Fig. 3.20C in Kanski)
Definitive Surgical Treatment
Dacryocystorhinostomy (DCR) is commonly required after the acute infection has resolved to:
- Prevent recurrence
- Address the underlying NLDO
- Facilitate closure of a fistula if present
A 2024 systematic review and meta-analysis (Li et al., PMID 38444220) examined early endonasal DCR during the acute phase, suggesting it may be safe and effective in selected patients — challenging the traditional approach of waiting for infection to fully resolve before surgery.
Complications
| Complication | Comment |
|---|---|
| Lacrimal sac abscess | Common progression if untreated |
| Preseptal cellulitis | Spread of infection anterior to orbital septum |
| Orbital cellulitis | Rare but serious; requires IV antibiotics and urgent imaging |
| Skin fistula | Especially after spontaneous or surgical drainage |
| Recurrence | High without correction of underlying NLDO |
Follow-Up
- Daily visits until improvement confirmed
- If outpatient condition worsens → hospitalize for IV antibiotics
- Once infection resolves: probing and irrigation to assess nasolacrimal patency, then plan for DCR if obstructed
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 124–125
- The Wills Eye Manual, pp. 399–402
- Tintinalli's Emergency Medicine, Chapter 122
- Li J et al. "Early Endonasal Dacryocystorhinostomy for Acute Dacryocystitis." Am J Rhinol Allergy 2024 — PMID 38444220
This is a shared conversation. Sign in to Orris to start your own chat.