Elderly female with pancerebellar inv - history to ask , examination, investigations and dd
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed to compile a comprehensive, structured answer. Let me synthesize this.
Pancerebellar Syndrome in an Elderly Female — Complete Clinical Approach
"Pancerebellar" involvement means all three functional zones of the cerebellum are affected: midline vermis (truncal/gait ataxia), anterior lobe (limb ataxia, titubation), and flocculonodular lobe (vestibulo-ocular dysfunction), producing the full tetrad of ataxia, dysarthria, nystagmus, and limb incoordination.
1. HISTORY TO ASK
Onset & Time Course (Most Critical for DD)
| Pattern | Suggests |
|---|---|
| Acute (hours–days) | Stroke, Wernicke's, drug toxicity, MS relapse |
| Subacute (weeks–months) | Paraneoplastic, autoimmune (anti-GAD), CJD, abscess |
| Chronic progressive (months–years) | MSA-C, ILOCA, gluten ataxia, hypothyroid |
| Episodic | Episodic ataxia EA-1/EA-2, TIA, MS |
Presenting Complaint
- Gait unsteadiness, falls, veering to one side
- Slurred/scanning speech
- Double vision, oscillopsia
- Clumsiness of hands (writing, utensils, dressing)
- Swallowing difficulty (late feature)
- Dizziness or vertigo
Aetiological History — Key Questions in Elderly Female
Paraneoplastic (high priority in women):
- History of breast or ovarian cancer (anti-Yo antibodies), lung cancer (anti-Hu), gynaecological malignancy
- Weight loss, night sweats, lumps, menstrual changes (if relevant)
- Previous cancer screening results
Autoimmune / metabolic:
- Known hypothyroidism (myxoedema ataxia)
- Coeliac disease or gluten sensitivity — GI symptoms (diarrhoea, bloating), family history
- Type 1 diabetes (anti-GAD ataxia)
Toxic / nutritional:
- Alcohol consumption — daily quantity, duration
- Drug history: phenytoin, carbamazepine, phenobarbital, lithium, metronidazole, amiodarone, chemotherapy agents
- Dietary adequacy — thiamine (B1), B12, vitamin E intake
Vascular:
- Hypertension, diabetes, atrial fibrillation, smoking (cerebellar stroke risk)
- Sudden onset or stepwise progression
Infectious / inflammatory:
- Recent viral illness (post-infectious cerebellitis, though rare in elderly)
- HIV risk factors
- TB exposure
Degenerative:
- Associated parkinsonism features: rigidity, bradykinesia, REM sleep behaviour disorder → MSA-C
- Autonomic dysfunction: orthostatic hypotension, urinary incontinence, constipation, impotence → MSA
- Family history of ataxia (late-onset SCA — SCA-6, SCA-2 possible even in elderly)
Systemic:
- Connective tissue disease history (SLE, Sjögren — autoimmune ataxia)
Functional Impact
- Falls and injuries
- Ability to walk, use stairs, self-care
2. EXAMINATION
General
- Nutritional status, BMI, signs of chronic alcoholism (spider naevi, parotid enlargement)
- Lymphadenopathy, breast masses → paraneoplastic screen
- Skin: telangiectasia (ataxia-telangiectasia — rare in elderly), rash, jaundice
Neurological Examination — Five Domains (SARA Scale)
1. Eyes
| Finding | Significance |
|---|---|
| Gaze-evoked nystagmus | Non-specific cerebellar |
| Downbeat nystagmus | Midline/floccular lesion, MSA, drugs |
| Upbeat nystagmus | Anterior vermis lesion |
| Square-wave jerks | Friedreich's, PSP |
| Ocular dysmetria / hypometric saccades | SCA-2 (slow), various SCAs |
| Smooth pursuit breakdown | SCA-3, many types |
| Skew deviation | Posterior fossa structural lesion |
2. Speech
- Scanning (cerebellar) dysarthria: slow, with irregular rhythm and undue separation of syllables
- Explosive or slurred speech
3. Hands / Upper Limbs
- Finger-nose test: intention tremor, dysmetria, past-pointing
- Finger-chase test: overshoot/undershoot
- Dysdiadochokinesis (rapid alternating pronation/supination)
- Rebound phenomenon (Holmes rebound)
- Titubation (rhythmic head/trunk tremor)
4. Lower Limbs / Coordination
- Heel-shin test: heel falls off the shin
- Lower limb intention tremor
5. Gait and Stance
- Wide-based, lurching, staggering gait — worsened on narrow base or tandem walking
- Romberg test: positive suggests sensory ataxia (consider combined disease)
- Truncal sway on sitting without back support
- Titubation at 3 Hz = anterior lobe atrophy
Associated Signs (Crucial for Aetiological Clues)
- Pyramidal signs (extensor plantars, brisk reflexes) → MSA-C, MS, spinocerebellar degeneration
- Extrapyramidal features (rigidity, bradykinesia) → MSA
- Autonomic: postural BP drop, anhidrosis
- Peripheral neuropathy (absent ankle jerks, reduced vibration/proprioception) → Friedreich's, paraneoplastic sensory neuropathy, B12/B1 deficiency
- Optic atrophy → Friedreich's, mitochondrial
- Pes cavus, scoliosis → Friedreich's (rare new presentation in elderly, but recessive forms)
- Cognitive impairment → MSA (minimal), CJD (rapid), posterior cerebellar atrophy
3. INVESTIGATIONS
Tier 1 — All Patients
| Investigation | Looking For |
|---|---|
| MRI Brain (with gadolinium) | Cerebellar atrophy pattern, structural lesions, vascular disease, hot-cross-bun sign (MSA), T2 peduncle changes |
| Blood glucose + HbA1c | Diabetic neuropathy, anti-GAD ataxia context |
| Thyroid function tests | Hypothyroid cerebellar ataxia (myxoedema) |
| Serum B12, folate | Deficiency |
| Serum thiamine (B1) | Wernicke's, especially if alcohol history |
| Serum vitamin E | Deficiency ataxia |
| LFTs, GGT | Alcoholic cerebellar degeneration |
| FBC, ESR, CRP | Inflammatory, neoplastic |
| U&E, calcium | Metabolic causes |
Tier 2 — Based on Clinical Suspicion
Paraneoplastic workup (subacute onset, elderly female):
- Paraneoplastic antibody panel: anti-Yo (PCA-1), anti-Hu (ANNA-1), anti-Ri, anti-Tr (DNER), anti-CASPR2, anti-NMDAR
- CT chest/abdomen/pelvis or PET-CT — occult malignancy (breast, ovary, lung)
- Mammography, CA-125, CA 19-9 as directed
Autoimmune:
- Anti-GAD antibodies (high titre > 2000 IU/mL → autoimmune ataxia)
- Anti-gliadin + anti-tissue transglutaminase antibodies (gluten/coeliac ataxia)
- Anti-TPO antibodies (Hashimoto encephalopathy / SREAT)
- ANA, ANCA, anti-dsDNA if systemic autoimmune suspected
Metabolic:
- Serum alpha-fetoprotein (elevated in ataxia-telangiectasia)
- Serum cholesterol (cerebrotendinous xanthomatosis)
- Lactate, pyruvate (mitochondrial disease)
CSF analysis (especially if immune-mediated or CJD suspected):
- Cell count, protein, glucose
- Oligoclonal bands (MS)
- 14-3-3 protein → CJD
- CSF paraneoplastic antibodies (when serum negative but suspicion high)
- CSF anti-GAD, anti-gliadin (when serum equivocal)
Genetic (late-onset sporadic):
- CANVAS screen (RFC1 repeat expansion) — onset >45 years without family history
- FXTAS (fragile X tremor-ataxia syndrome — females can be affected; FMR1 CGG repeat)
- Spinocerebellar ataxia panel (SCA-1, 2, 3, 6, 7) if family history
- Whole-exome/genome sequencing if no diagnosis reached
Neurophysiology:
- Nerve conduction studies + EMG — peripheral neuropathy (Friedreich's, paraneoplastic sensory neuronopathy, B12)
- VEPs, SSEPs — MS, mitochondrial
4. DIFFERENTIAL DIAGNOSIS
Ranked by priority in an elderly female with pancerebellar involvement:
Most Important / Common
| Diagnosis | Key Clues |
|---|---|
| Paraneoplastic cerebellar degeneration | Subacute onset, elderly female, breast/ovarian Ca, anti-Yo+, rapid progression |
| Multiple System Atrophy – Cerebellar (MSA-C) | Autonomic dysfunction, parkinsonism, hot-cross-bun MRI sign |
| Idiopathic Late-Onset Cerebellar Ataxia (ILOCA) | Slow progression, no cause found, diagnosis of exclusion |
| Alcoholic/nutritional cerebellar degeneration | Alcohol history, anterior vermis atrophy, B1 deficiency |
| Cerebellar stroke | Acute/stepwise onset, vascular risk factors, DWI on MRI |
Autoimmune / Metabolic
| Diagnosis | Key Clues |
|---|---|
| Gluten ataxia | GI symptoms or silent coeliac, anti-gliadin/anti-TG antibodies, responds to gluten-free diet |
| Anti-GAD ataxia | T1DM, stiff-person features, high anti-GAD titres |
| Hashimoto encephalopathy (SREAT) | Hypothyroid or euthyroid, anti-TPO+, responds to steroids |
| Hypothyroid cerebellar ataxia | Overt hypothyroidism, improves with thyroxine |
| Wernicke encephalopathy | Alcohol/malnutrition, confusion + ophthalmoplegia + ataxia triad, mamillary body T2 changes |
Structural / Infectious / Other
| Diagnosis | Key Clues |
|---|---|
| Posterior fossa tumour (primary or metastatic) | MRI mass lesion with mass effect |
| Multiple sclerosis | Age less typical but possible; relapsing course, CSF OCBs, white matter lesions |
| Creutzfeldt-Jakob disease (CJD) | Rapidly progressive dementia + ataxia, 14-3-3 in CSF, DWI cortical ribboning |
| CANVAS (RFC1) | Sensory neuropathy + vestibular areflexia + ataxia, cough, >45 yr onset |
| FXTAS | Tremor + ataxia + MCP T2 signal; FMR1 premutation (female carriers can be affected) |
| Drug-induced | Phenytoin, carbamazepine, lithium — medication review essential |
| Superficial siderosis | Haemosiderin on MRI susceptibility sequences, hearing loss |
| Mitochondrial ataxia (POLG) | Multisystem, elevated lactate, T2 inferior olive changes |
Diagnostic Workflow
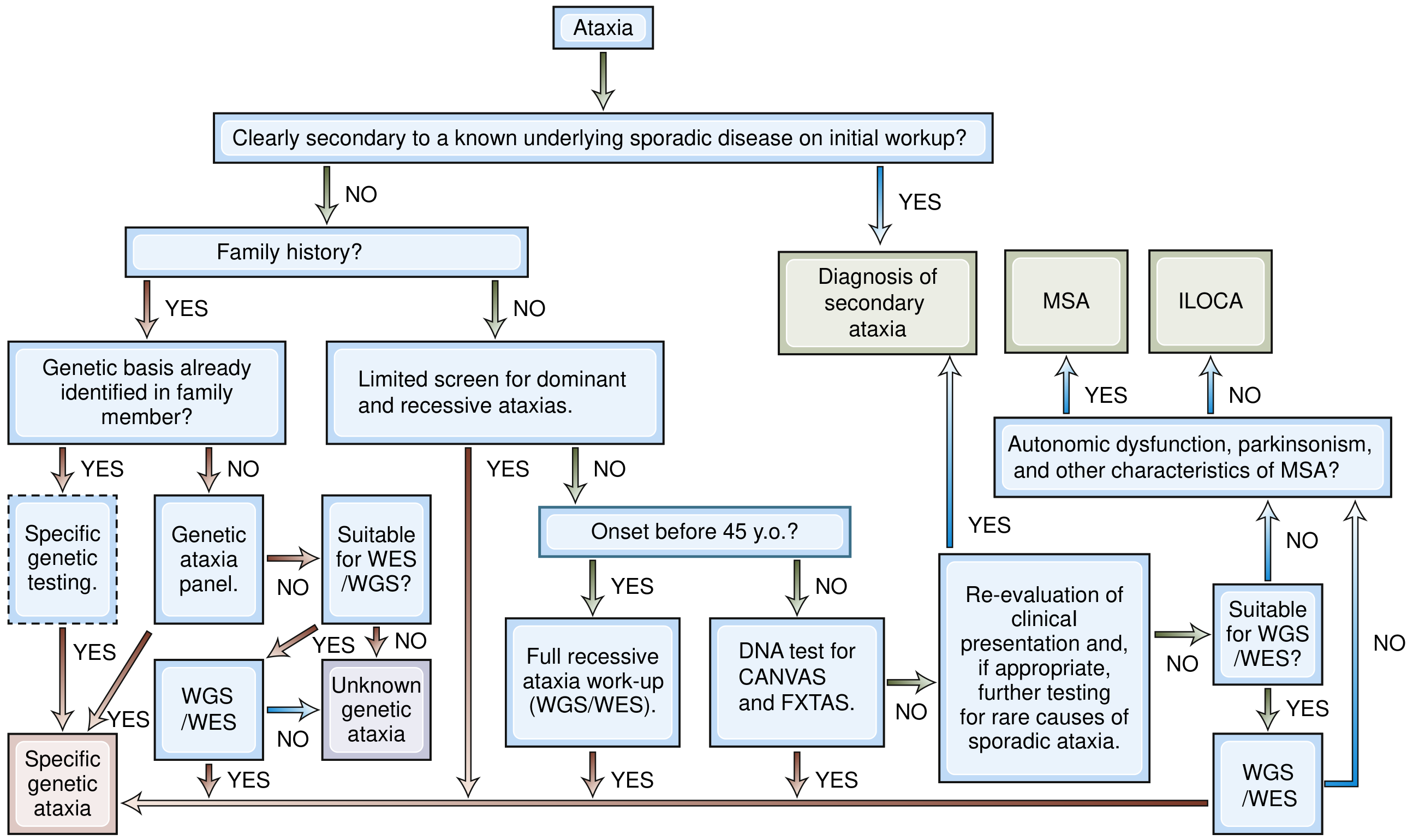
Fig: Step-by-step diagnostic algorithm for cerebellar ataxia. For elderly females with sporadic onset >45 years, if no family history: screen for secondary causes, test for CANVAS/FXTAS, then consider MSA-C vs ILOCA. — Bradley and Daroff's Neurology in Clinical Practice
Key Clinical Pearl for Elderly Females
Paraneoplastic cerebellar degeneration must be actively excluded — it affects predominantly women with breast or ovarian cancers, evolves rapidly (weeks to months), and can precede cancer detection by years. Anti-Yo antibodies are the signature; PET-CT is essential even when structural imaging is negative. — Adams and Victor's Principles of Neurology, 12th Ed.; Bradley and Daroff's Neurology in Clinical Practice
Young pt with dementia approach
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I've exhausted my DB queries but have the core textbook content. Let me now compile the comprehensive answer from what was retrieved, supplemented with authoritative knowledge.
Young-Onset Dementia (YOD) — Complete Clinical Approach
Definition: Dementia with onset before age 65 (some use <45 for "true" young-onset). This is critical because the differential is dramatically different from late-onset dementia — treatable causes are far more common and must be actively excluded.
Epidemiologically (Mayo Clinic data, Kelley et al. 2008): neurodegenerative (31%), autoimmune/inflammatory (21%), metabolic (11%), unknown (19%).
1. HISTORY
Presenting Cognitive Complaint
Characterise the domains involved — this determines the syndrome type:
| Domain | Examples | Points toward |
|---|---|---|
| Memory (episodic) | Forgetting recent events, repetitive questioning | Alzheimer's |
| Behaviour / personality | Disinhibition, apathy, loss of empathy, socially inappropriate | FTD (bvFTD) |
| Language | Word-finding difficulty, non-fluent speech, comprehension loss | PPA / FTD |
| Executive function | Poor planning, impulsivity, can't multitask | FTD, vascular, HD |
| Visuospatial | Getting lost, difficulty driving, dressing | Posterior cortical atrophy, DLB |
| Psychiatric | Hallucinations (visual), delusions | DLB, autoimmune |
| Psychomotor | Slowness, clumsiness, falls | DLB, HD, CBD, PSP |
Onset & Progression
- Acute / subacute (days–weeks): autoimmune encephalitis, prion disease (CJD), CNS vasculitis, toxic/metabolic, NCSE
- Subacute (weeks–months): paraneoplastic, autoimmune, CJD, lymphoma, Wernicke's
- Gradual progressive (months–years): neurodegenerative (FTD, AD, HD, DLB), storage diseases, MS, mitochondrial
- Stepwise: vascular dementia
- Fluctuating: DLB (core feature), autoimmune, vascular
Aetiological Focused Questions
Family history (critical in young patients):
- Dementia in relatives — age of onset, type
- Huntington's disease — known family diagnosis? Chorea in relatives?
- Early-onset Alzheimer's (familial AD — PSEN1, PSEN2, APP mutations)
- FTD/ALS overlap — motor neuron disease in family (MAPT, PGRN, C9orf72)
Drug & substance history:
- Alcohol — quantity, duration (alcohol-related brain damage, Wernicke-Korsakoff)
- Recreational drugs — chronic cannabis, stimulants
- Medications — lithium, methotrexate, anticholinergics, immunosuppressants
Psychiatric history:
- Depression can mimic dementia ("pseudodementia") — previous depressive episodes, onset of mood change before or after cognitive decline
- Schizophrenia — long-standing psychosis with cognitive decline
Medical history:
- HIV status / risk factors
- Autoimmune disease: SLE (neuropsychiatric lupus), Sjögren's, antiphospholipid syndrome
- Thyroid disease, liver disease, renal failure, diabetes
- Epilepsy (NCSE, post-ictal state)
- Cardiac disease / stroke risk (vascular dementia)
- Down syndrome (early Alzheimer's)
- Head injury
Systemic symptoms (paraneoplastic / inflammatory):
- Weight loss, night sweats, fever, lymphadenopathy
- Rash (lupus, vasculitis)
- Joint pains, sicca symptoms (Sjögren's)
- Seizures (autoimmune encephalitis, CJD)
Movement symptoms (crucial clues):
- Involuntary movements / chorea → Huntington's disease
- Rigidity, slowness → DLB, HD, CBD, Wilson's
- Tremor, Kayser-Fleischer rings → Wilson's disease (<45 yr, copper)
- Dystonia, dysarthria → Wilson's, neurodegeneration with brain iron accumulation (NBIA)
- Gait difficulty, falls → vascular, NPH, DLB, PSP
Sleep history:
- REM sleep behaviour disorder → DLB (precedes dementia)
- Excessive daytime sleepiness → DLB, NPH
Occupational / social history:
- Occupation (toxic exposures — heavy metals, solvents)
- Driving ability, job performance
- Social function, relationships
2. EXAMINATION
Cognitive Assessment
- Bedside cognitive tests: MoCA (Montreal Cognitive Assessment — preferred), MMSE, ACE-III
- Delineate which cognitive domains are affected (memory, executive, visuospatial, language, attention)
- Compare informant history with patient's own account (anosognosia → FTD, Alzheimer's)
General Examination — Aetiological Clues
| Finding | Suggests |
|---|---|
| Kayser-Fleischer rings (slit-lamp) | Wilson's disease |
| Rash (malar, livedo reticularis) | SLE, antiphospholipid |
| Lymphadenopathy / organomegaly | Lymphoma, storage disease, sarcoidosis |
| Signs of chronic liver disease | Wilson's, alcohol |
| Xanthomas, corneal arcus | Hyperlipidaemia, cerebrotendinous xanthomatosis |
| Telangiectasia | Ataxia-telangiectasia |
| Café-au-lait spots | Neurofibromatosis |
| Skin changes, alopecia | Mitochondrial, SLE |
Neurological Examination
Higher functions: attention, memory (registration + recall), language (fluency, naming, comprehension, repetition), praxis, visuospatial, executive (abstraction, set-shifting)
Cranial nerves:
- Vertical gaze palsy → PSP, Niemann-Pick type C
- Ophthalmoplegia → mitochondrial (MELAS), Wernicke's
- Optic atrophy → mitochondrial, MS
- Nystagmus → MS, Wernicke's, mitochondrial
Motor system:
- Chorea → Huntington's disease (pathognomonic), neuroacanthocytosis, SLE, antiphospholipid
- Parkinsonism (rigidity, bradykinesia, tremor) → DLB, HD (rigid variant), Wilson's, CBD, MSA
- Alien limb, cortical myoclonus, akinetic-rigid + cognitive → Corticobasal Degeneration (CBD)
- Pyramidal signs (spasticity, extensor plantars) → MS, vascular, metabolic leukodystrophies, HSP
- Lower motor neuron + dementia → ALS-FTD (C9orf72)
- Cerebellar signs → CJD, mitochondrial, prion, alcohol
Primitive reflexes (grasp, palmomental, snout) → frontal lobe involvement → FTD, advanced AD
Gait:
- Apraxic / magnetic gait + urinary incontinence → Normal Pressure Hydrocephalus (NPH)
- Parkinsonian gait → DLB, HD-rigid, Wilson's
- Ataxic gait → CJD, mitochondrial, alcohol, Wernicke's
Psychiatric features:
- Visual hallucinations → DLB (well-formed, animals/people)
- Disinhibition, altered eating behaviour, loss of empathy → FTD
- Catatonia → autoimmune (NMDAR), metabolic
3. INVESTIGATIONS
Tier 1 — All Patients (Mandatory)
| Investigation | Purpose |
|---|---|
| MRI Brain (with gadolinium + DWI + FLAIR + SWI) | Structural lesions, atrophy pattern, vascular changes, DWI ribboning (CJD), iron deposition, white matter disease |
| FBC, ESR, CRP | Inflammatory, infective, haematological |
| Metabolic panel: U&E, LFTs, glucose, calcium, magnesium | Metabolic encephalopathy |
| TFTs | Hypothyroidism, Hashimoto encephalopathy |
| B12, folate, thiamine | Deficiency states (B1 → Wernicke's) |
| Syphilis serology (VDRL/TPHA) | Neurosyphilis |
| HIV test | HIV-associated neurocognitive disorder |
| Urine drug screen | Substance-related cognitive impairment |
Tier 2 — Targeted by Clinical Context
Autoimmune / Inflammatory:
- Autoimmune encephalitis antibodies (serum + CSF): anti-NMDAR, anti-LGI1, anti-CASPR2, anti-AMPAR, anti-GABA-B — the most important treatable causes in young patients
- ANA, anti-dsDNA, ANCA, antiphospholipid antibodies (lupus, vasculitis)
- Anti-TPO, anti-thyroglobulin (Hashimoto encephalopathy / SREAT)
- Angiotensin-converting enzyme (ACE) → neurosarcoidosis
Paraneoplastic:
- Paraneoplastic antibody panel (anti-Hu, anti-NMDAR, anti-Yo, anti-Ri, anti-Ma2)
- CT chest/abdomen/pelvis or PET-CT → occult malignancy
Metabolic / Genetic:
- Serum copper, caeruloplasmin, 24-hr urine copper → Wilson's disease (mandatory in all <45)
- Serum ammonia → hepatic encephalopathy
- Lactate, pyruvate → mitochondrial disease
- Very long-chain fatty acids (VLCFA) → adrenoleukodystrophy
- Lysosomal enzyme panel → storage diseases (Gaucher, Niemann-Pick, GM2 gangliosidosis)
- Arylsulfatase A → metachromatic leukodystrophy
Prion / CSF:
- CSF analysis: opening pressure, cells, protein, glucose, oligoclonal bands (MS), 14-3-3 protein, RT-QuIC (prion)
- CSF Real-time quaking-induced conversion (RT-QuIC) — high sensitivity for CJD
- CSF autoimmune encephalitis antibodies (when serum negative)
Neuroimaging (advanced):
- FDG-PET: hypometabolism patterns — posterior temporal/parietal (AD), frontal (FTD), striatal (HD)
- Amyloid PET (florbetapir/florbetaben): early-onset AD confirmation
- DaTscan (123I-FP-CIT SPECT): dopaminergic deficit → DLB vs AD
Genetic Testing:
- Huntingtin gene CAG repeat → Huntington's disease (if chorea + family history)
- FMR1 CGG repeat → Fragile X-associated neurological disorders (FXAND)
- Early-onset familial AD panel: PSEN1, PSEN2, APP
- FTD/ALS panel: MAPT, PGRN, C9orf72, TARDBP
- PRND / PRNP → familial CJD if rapid progressive dementia
- Whole-exome sequencing if no diagnosis reached
Neurophysiology:
- EEG: periodic sharp wave complexes (CJD), non-convulsive status epilepticus, subclinical seizures
- NCS/EMG: peripheral neuropathy (B12, mitochondrial, paraneoplastic)
Neuropsychological Testing:
- Formal neuropsychological battery to characterise cognitive profile, assist in differential, and provide baseline
4. DIFFERENTIAL DIAGNOSIS
By Age Group (Critical Distinction)
| Age Group | Top Causes |
|---|---|
| 17–45 | FTD, Huntington's, MS, autoimmune encephalitis, neuropsychiatric lupus, mitochondrial, storage disease, prion, vasculitis, Wilson's |
| 45–65 | Alzheimer's (early-onset), vascular dementia, FTD, alcohol-related, DLB, HD, MS, Down syndrome |
Organised by Category
Neurodegenerative:
- Frontotemporal dementia (FTD) — most common in <60; behaviour variant (bvFTD) or language variant (PPA); ALS-FTD overlap (C9orf72)
- Early-onset Alzheimer's disease — familial (PSEN1 most common), posterior cortical atrophy variant
- Huntington's disease — autosomal dominant, chorea + psychiatric + cognitive, CAG >36
- Dementia with Lewy Bodies (DLB) — REM sleep behaviour disorder, visual hallucinations, fluctuating cognition, parkinsonism
- Corticobasal Degeneration (CBD) — alien limb, apraxia, asymmetric akinetic-rigid
- Progressive Supranuclear Palsy (PSP) — vertical gaze palsy, falls, subcortical dementia
Autoimmune / Inflammatory:
- Autoimmune encephalitis (anti-NMDAR, anti-LGI1, anti-CASPR2) — most important treatable cause; must not miss
- Hashimoto encephalopathy (SREAT) — anti-TPO+, fluctuating, responds to steroids
- CNS vasculitis (primary or secondary to SLE, ANCA)
- Neuropsychiatric SLE
- Neurosarcoidosis
- MS — relapsing or progressive, white matter lesions, OCBs
Prion:
- Sporadic CJD — rapidly progressive dementia + myoclonus + ataxia + periodic EEG, 14-3-3+, DWI cortical ribboning
- Variant CJD — young patients, psychiatric onset, thalamic DWI signal, prion-contaminated beef exposure
Toxic / Nutritional:
- Alcohol-related brain damage — Wernicke-Korsakoff (B1 deficiency), direct neurotoxicity
- B12 deficiency — subacute combined degeneration + cognitive decline
- Drug toxicity — lithium, methotrexate, immunosuppressants, chronic cannabis
Metabolic / Genetic Metabolic:
- Wilson's disease — copper accumulation, <45, psychiatric + neurological + liver disease, KF rings
- Mitochondrial disease (MELAS, MERRF, POLG) — multisystem, stroke-like episodes, lactic acidosis
- Storage diseases — Gaucher (GBA), Niemann-Pick type C (NPC1/2), GM2 gangliosidosis — vertical gaze palsy, organomegaly
- Metachromatic leukodystrophy (MLD) — arylsulfatase A deficiency, white matter disease
- Adrenoleukodystrophy — X-linked, posterior white matter, VLCFA elevated
- Neurodegeneration with brain iron accumulation (NBIA) — basal ganglia iron on MRI
Structural / Vascular:
- Vascular dementia — stepwise decline, lacunar infarcts, white matter disease, vascular risk factors
- Normal Pressure Hydrocephalus (NPH) — Hakim's triad: gait apraxia + urinary incontinence + dementia; treatable with VP shunt
- Chronic subdural haematoma — head injury (may be forgotten), fluctuating, bilateral
- CNS lymphoma — periventricular ring-enhancing lesions, immunocompromised
Infective:
- HIV-associated neurocognitive disorder (HAND) — must screen in all young patients
- Neurosyphilis — psychiatric + cognitive + tabes dorsalis, VDRL/TPHA
- Viral encephalitis (HSV, CMV, EBV) — acute onset, fever, seizures
- Whipple disease — rare, oculomasticatory myorhythmia + cognitive decline, gut symptoms
- Fungal / TB meningitis — immunocompromised, subacute
Psychiatric Mimics:
- Depression ("pseudodementia") — history of depression, onset of mood before cognition, cognitive symptoms worse subjectively than objectively, responds to antidepressants
- Schizophrenia — long-standing psychosis, cognitive impairment, young onset
- Functional cognitive disorder — internal inconsistency on testing
Red Flags for Urgent Assessment
| Flag | Implication |
|---|---|
| Rapid progression (weeks) | CJD, autoimmune encephalitis, CNS lymphoma |
| Fever + cognitive decline | Infectious encephalitis, Whipple |
| Seizures + cognitive decline | Autoimmune encephalitis, NCSE |
| Visual hallucinations | DLB, autoimmune |
| Chorea + young patient | Huntington's, SLE, antiphospholipid |
| Vertical gaze palsy | PSP, Niemann-Pick C |
| Psychiatric onset in teens–20s | Variant CJD, anti-NMDAR encephalitis, Wilson's |
| Gait + urinary incontinence + dementia | NPH — treatable! |
| Kayser-Fleischer rings | Wilson's — treatable! |
Mnemonic for Treatable/Reversible Causes — "DEMENTIAS"
Drugs & toxins · Endocrine (thyroid, Addison's, parathyroid) · Metabolic (B12, thiamine, Wilson's, hepatic) · Epilepsy (NCSE) · Normal pressure hydrocephalus · Tumour / trauma (SDH) · Infection (HIV, syphilis, HSV) · Autoimmune / inflammatory encephalitis · Structural / vascular
Core principle: In young-onset dementia, a thorough aetiological workup is mandatory — up to 20–30% of cases have a treatable or reversible cause that will be missed without systematic investigation. — Bradley and Daroff's Neurology in Clinical Practice
In viva style and crisp
Young Patient with Dementia — Viva Style
Q: Define young-onset dementia.
Dementia with onset before age 65. Onset before 45 is termed "true" young-onset. The younger the patient, the broader and more treatable the differential.
Q: What is the most important thing to establish first?
Time course of onset — it dictates the entire differential:
- Acute/subacute (days–weeks) → autoimmune encephalitis, CJD, CNS vasculitis, NCSE, Wernicke's
- Months → paraneoplastic, lymphoma, prion, metabolic
- Gradual over years → FTD, early-onset AD, HD, storage diseases, MS
Q: What history would you take?
Cognitive domain affected:
- Memory → AD
- Behaviour/personality change, disinhibition, loss of empathy → FTD
- Visuospatial → posterior cortical atrophy, DLB
- Fluctuating cognition + visual hallucinations → DLB
Key targeted questions:
- Family history — dementia, chorea, MND? (HD, familial AD, FTD)
- Alcohol — quantity, duration (Wernicke-Korsakoff)
- Drug history — lithium, methotrexate, anticholinergics
- HIV risk factors, sexual history → HAND, syphilis
- Involuntary movements → Huntington's
- Psychiatric symptoms before cognition → variant CJD, anti-NMDAR, Wilson's
- Gait difficulty + urinary incontinence → NPH (treatable!)
- Weight loss, cancer history → paraneoplastic
- Autoimmune history — SLE, thyroid disease
- REM sleep behaviour disorder → DLB
- Seizures → autoimmune encephalitis, NCSE
Q: What would you look for on examination?
Bedside cognition: MoCA — characterise the profile (memory vs behaviour vs visuospatial vs language)
Examine for aetiological clues:
| Sign | Diagnosis |
|---|---|
| Kayser-Fleischer rings | Wilson's disease |
| Chorea | Huntington's, SLE, antiphospholipid |
| Vertical gaze palsy | PSP, Niemann-Pick C |
| Alien limb + cortical myoclonus | CBD |
| Parkinsonism + visual hallucinations | DLB |
| Magnetic gait + urinary incontinence | NPH |
| Cerebellar signs + myoclonus + rapid course | CJD |
| Peripheral neuropathy | B12, mitochondrial, paraneoplastic |
| Rash, serositis | SLE |
| Ophthalmoplegia + ataxia + confusion | Wernicke's triad |
| Primitive reflexes (grasp, palmomental) | Frontal involvement → FTD, advanced AD |
Q: How would you investigate?
Tier 1 — everyone:
- MRI brain (DWI + FLAIR + SWI + gadolinium)
- FBC, ESR, CRP, metabolic panel
- TFTs, B12, folate, thiamine
- Syphilis serology, HIV test (mandatory in young)
- Urine drug screen
Tier 2 — targeted:
Autoimmune (most important treatable group):
- Anti-NMDAR, anti-LGI1, anti-CASPR2, anti-AMPAR, anti-GABA-B (serum + CSF)
- ANA, anti-dsDNA, ANCA, antiphospholipid antibodies
- Anti-TPO (Hashimoto encephalopathy)
Metabolic/genetic:
- Copper + caeruloplasmin + 24-hr urine copper → Wilson's (mandatory <45)
- Lactate, pyruvate → mitochondrial
- VLCFA → adrenoleukodystrophy
- Lysosomal enzymes → storage diseases
Prion:
- CSF 14-3-3, RT-QuIC (high sensitivity for CJD)
- EEG — periodic sharp wave complexes
Genetic:
- Huntingtin CAG repeat (if chorea/family history)
- PSEN1, PSEN2, APP (familial AD)
- C9orf72, MAPT, PGRN (FTD/ALS)
Advanced imaging:
- FDG-PET — hypometabolism pattern
- DaTscan — if DLB suspected
- Amyloid PET — if early-onset AD suspected
Q: Give the differential diagnosis.
17–45 years (Kelley et al., Mayo Clinic — most common):
- Frontotemporal dementia
- Huntington's disease
- Multiple sclerosis
- Autoimmune encephalitis
- Neuropsychiatric lupus
- Mitochondrial disease
- Storage disease
- Prion disease (CJD/vCJD)
- Vasculitis
45–65 years (Harvey et al.):
- Alzheimer's disease
- Vascular dementia
- FTD
- Alcohol-related dementia
- DLB
- Huntington's disease
- Multiple sclerosis
- Down syndrome–related AD
- CBD / prion disease / Parkinson's dementia
Q: What are the treatable/reversible causes you must not miss?
Use DEMENTIAS:
- D — Drugs & toxins
- E — Endocrine (hypothyroid, Addison's)
- M — Metabolic (B12, thiamine, Wilson's, hepatic)
- E — Epilepsy (non-convulsive status)
- N — Normal pressure hydrocephalus
- T — Tumour / Trauma (SDH)
- I — Infection (HIV, syphilis, HSV encephalitis)
- A — Autoimmune/inflammatory encephalitis
- S — Structural (subdural, hydrocephalus)
Q: What are the red flags for rapid referral?
- Weeks of progression → CJD, autoimmune encephalitis
- Fever + cognitive decline → encephalitis
- Seizures + confusion → NCSE, anti-NMDAR
- Chorea in a young patient → Huntington's, SLE
- Vertical gaze palsy → PSP, Niemann-Pick C
- Triad of gait + incontinence + dementia → NPH — refer for shunting
- Psychiatric onset in teens → vCJD, Wilson's, anti-NMDAR
Q: One sentence bottom line?
In young-onset dementia, up to 30% have a treatable cause — a systematic workup starting with time course, cognitive profile, and targeted investigations (especially autoimmune, metabolic, genetic) is non-negotiable.
In flowcharts manner
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.