Skin disease by fungal organism 10 marker for MD pathology rguhs university exam
Reading File
Finding Sources
Finding Sources
Searching the Web
fungal skin disease 10 marks MD pathology RGUHS exam answer dermatophytosis candidiasis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
I now have comprehensive material from Robbins Pathology, Fitzpatrick's Dermatology, and Sherris Microbiology. I have enough to write an excellent, exam-standard 10-marker answer for RGUHS MD Pathology.
Skin Diseases Caused by Fungal Organisms
[RGUHS MD Pathology - 10 Marks Answer]
Introduction
Fungal infections of the skin (cutaneous mycoses) are among the most common dermatological conditions worldwide. They are broadly classified into:
- Superficial mycoses - confined to the stratum corneum, hair, and nails
- Subcutaneous mycoses - involving dermis and subcutaneous tissue
- Deep/systemic mycoses - hematogenous spread, often in immunocompromised patients
Classification of Causative Organisms
I. Dermatophytes (Most Common)
Three genera cause superficial keratinolytic infections:
| Genus | Microconidia | Macroconidia | Key Species |
|---|---|---|---|
| Trichophyton | Smooth-walled; diagnostic | Absent/non-diagnostic | T. rubrum (most common), T. tonsurans |
| Microsporum | Absent/non-diagnostic | Rough-walled; diagnostic | M. canis, M. audouinii |
| Epidermophyton | Absent | Smooth-walled; diagnostic | E. floccosum |
Classified further by habitat:
- Anthropophilic (humans) - e.g. T. rubrum, T. tonsurans, E. floccosum
- Zoophilic (animals) - e.g. M. canis (cats/dogs), T. verrucosum (cattle)
- Geophilic (soil) - e.g. M. gypseum
(Source: Fitzpatrick's Dermatology, Table 160-1)
II. Non-Dermatophyte Yeasts
- Malassezia furfur - causes Pityriasis/Tinea versicolor
- Candida albicans - cutaneous candidiasis
Major Clinical Entities
1. Tinea Capitis
- Dermatophytosis of the scalp; mainly in children
- Patchy lesions with erythema, scaling, crust formation, and hair loss
- Causative agents: T. tonsurans (US), M. canis
- Types of hair invasion: ectothrix (Microsporum) vs endothrix (Trichophyton)
- Treatment requires oral antifungals (griseofulvin, terbinafine)
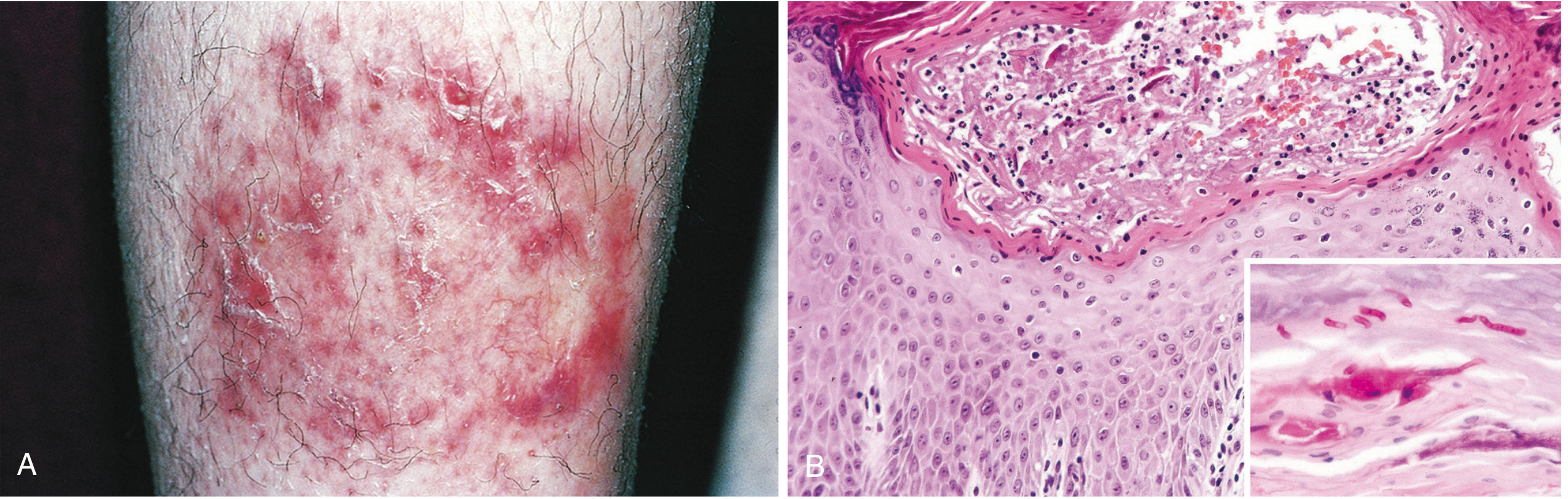
2. Tinea Corporis (Ringworm of the body)
- Most common superficial fungal infection of glabrous skin
- Affects all ages, especially children
- Predisposing factors: excessive heat, humidity, exposure to infected animals
- Clinical: Expanding round plaque with elevated, scaling, erythematous border and central clearing ("ringworm" appearance)
- Histopathology: Mild spongiotic (eczematous) dermatitis with intraepidermal neutrophils and neutrophilic microabscesses in the stratum corneum
3. Tinea Pedis (Athlete's foot)
- Most prevalent form; affects 30-40% of the population at some point
- Diffuse erythema and scaling, initially in toe web spaces
- Predisposing factors: occlusive footwear, communal bathing areas
4. Tinea Cruris (Jock Itch)
- Inguinal areas; predominantly obese males in warm weather
- Moist red patches with raised, scaly, well-defined borders
- Predisposed by heat, friction, and maceration
5. Tinea Unguium / Onychomycosis
- Dermatophytosis of the nails
- Nail thickening, discoloration, onycholysis (separation of nail plate)
- Requires prolonged oral antifungal therapy
6. Tinea Barbae
- Dermatophyte infection of the beard area in adult males
- Relatively uncommon
7. Tinea Versicolor (Pityriasis Versicolor)
- Caused by Malassezia furfur (a yeast, NOT a dermatophyte)
- Located on the upper trunk; highly distinctive
- Lesions: groups of macules of varied color (hypo- or hyperpigmented) with fine peripheral scale
- "Spaghetti and meatballs" pattern on KOH mount - short curved hyphae + round spores
- Hypopigmentation due to azelaic acid produced by Malassezia, which inhibits tyrosinase
8. Cutaneous Candidiasis
- Caused by Candida albicans
- Sites: intertriginous regions (axillary, inguinal, inframammary folds), oral mucosa, genitalia, nail folds
- Characteristic: Erythematous plaques with satellite lesions (small peripheral pustules/papules)
- Predisposed by diabetes, immunosuppression, antibiotic use, obesity, corticosteroid therapy
Histopathology of Dermatophyte Infections
(Robbins & Cotran Pathologic Basis of Disease)
The histologic features are variable depending on:
- Properties of the organism
- Host immune response
- Degree of secondary bacterial superinfection
Key histologic features:
- Mild spongiotic (eczematous) dermatitis in the epidermis
- Intraepidermal neutrophils and neutrophilic microabscesses - especially in the stratum corneum
- Superficial perivascular lymphocytic infiltrate in the dermis
- Fungi located in the anucleate cornified layer (stratum corneum) of lesional skin, hair, or nails
Special Stains for Diagnosis
| Stain | Appearance |
|---|---|
| PAS (Periodic Acid-Schiff) | Hyphae/spores stain bright pink to red (due to cell walls rich in mucopolysaccharides) |
| Gomori Methenamine Silver (GMS) | Fungi stain black against green background |
| KOH mount | Direct visualization of hyphae and spores in skin scrapings |
Culture & Laboratory Diagnosis
- Sabouraud Dextrose Agar (SDA) with cycloheximide + chloramphenicol: standard isolation medium; incubated at 20-25°C for up to 4 weeks
- Dermatophyte Test Medium (DTM): Contains phenol red indicator; turns red with dermatophyte growth (proteolytic activity raises pH)
- Wood's Lamp: Microsporum species fluoresce green (except M. audouinii/M. canis)
- KOH Preparation: Demonstration of septate hyphae confirms dermatophytosis
Pathogenesis
Dermatophytes produce keratinases that allow them to:
- Attach to and invade keratinized tissues (skin, hair, nails)
- Use keratin as a nutrient source
- Evoke innate immune response (neutrophil recruitment, epidermal spongiosis)
Malassezia is lipophilic and requires exogenous lipids for growth, explaining its predilection for sebaceous areas (upper trunk, scalp).
Treatment Summary
| Infection | Preferred Treatment |
|---|---|
| Tinea corporis/cruris/pedis | Topical azoles or allylamines (terbinafine) |
| Tinea capitis | Oral griseofulvin or terbinafine (6-8 weeks) |
| Onychomycosis | Oral terbinafine or itraconazole (pulse therapy) |
| Tinea versicolor | Topical selenium sulfide, ketoconazole shampoo, or oral itraconazole |
| Candidiasis | Topical/oral azoles; systemic fluconazole for recurrent cases |
Summary Table
| Disease | Organism | Characteristic Feature |
|---|---|---|
| Tinea capitis | Trichophyton / Microsporum | Scalp, children, hair loss |
| Tinea corporis | T. rubrum | Annular plaque, central clearing |
| Tinea pedis | T. rubrum, T. interdigitale | Toe webs, 30-40% prevalence |
| Tinea cruris | E. floccosum, T. rubrum | Inguinal, obese males |
| Onychomycosis | T. rubrum | Nail thickening, onycholysis |
| Tinea versicolor | Malassezia furfur | "Spaghetti & meatballs" on KOH, upper trunk |
| Candidiasis | Candida albicans | Satellite lesions, intertriginous |
Sources:
- Robbins & Cotran Pathologic Basis of Disease, Superficial Fungal Infections, Ch. 25
- Fitzpatrick's Dermatology, 9th Ed., Ch. 160 - Dermatophytes & Superficial Mycoses
- Sherris & Ryan's Medical Microbiology, 8th Ed., Ch. 6
Exam Writing Tip for RGUHS 10-marker: Structure your answer as: (1) Introduction + Classification [2 marks], (2) Clinical types with features [3 marks], (3) Histopathology with special stains [3 marks], (4) Diagnosis/Culture [1 mark], (5) Treatment outline [1 mark]. This covers all examiners' expected points for a complete answer.
This is a shared conversation. Sign in to Orris to start your own chat.