ENDOMETRIOSIS and ADENOMYOSIS visual details easy to understand chart
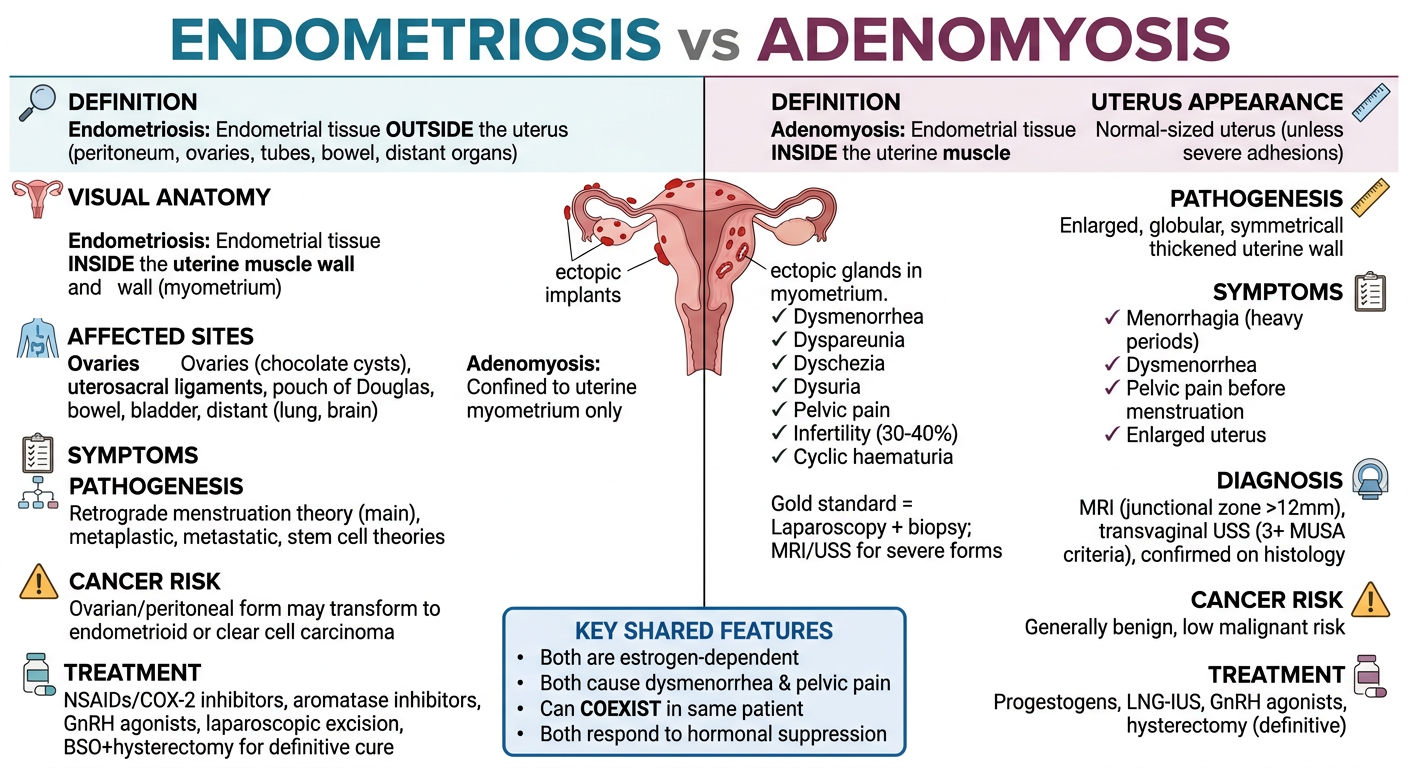
A detailed medical comparison chart titled "ENDOMETRIOSIS vs ADENOMYOSIS" split into two clear columns with a clean white background. Left column header: ENDOMETRIOSIS (in teal/blue). Right column header: ADENOMYOSIS (in purple/burgundy). Each column contains clearly labeled sections with icons: DEFINITION section: - Endometriosis: Endometrial tissue OUTSIDE the uterus (peritoneum, ovaries, tubes, bowel, distant organs) - Adenomyosis: Endometrial tissue INSIDE the uterine muscle wall (myometrium) VISUAL ANATOMY: A simple cross-section diagram of the uterus. Left side shows red dots/implants scattered outside on peritoneum, ovaries, fallopian tubes labeled "ectopic implants". Right side shows red nests/glands embedded deep within the thick muscular uterine wall labeled "ectopic glands in myometrium." Right uterus appears enlarged and globular. AFFECTED SITES: - Endometriosis: Ovaries (chocolate cysts), uterosacral ligaments, pouch of Douglas, bowel, bladder, distant (lung, brain) - Adenomyosis: Confined to uterine myometrium only SYMPTOMS (with checkmark bullets): - Endometriosis: Dysmenorrhea, dyspareunia, dyschezia, dysuria, pelvic pain, infertility (30-40%), cyclic haematuria - Adenomyosis: Menorrhagia (heavy periods), dysmenorrhea, pelvic pain before menstruation, enlarged uterus UTERUS APPEARANCE: - Endometriosis: Normal-sized uterus (unless severe adhesions) - Adenomyosis: Enlarged, globular, symmetrically thickened uterine wall PATHOGENESIS: - Endometriosis: Retrograde menstruation theory (main), metaplastic, metastatic, stem cell theories - Adenomyosis: Invagination of endometrial basalis into myometrium DIAGNOSIS: - Endometriosis: Gold standard = Laparoscopy + biopsy; MRI/USS for severe forms - Adenomyosis: MRI (junctional zone >12mm), transvaginal USS (3+ MUSA criteria), confirmed on histology CANCER RISK: - Endometriosis: Ovarian/peritoneal form may transform to endometrioid or clear cell carcinoma - Adenomyosis: Generally benign, low malignant risk TREATMENT: - Endometriosis: NSAIDs/COX-2 inhibitors, aromatase inhibitors, GnRH agonists, laparoscopic excision, BSO+hysterectomy for definitive cure - Adenomyosis: Progestogens, LNG-IUS, GnRH agonists, hysterectomy (definitive) KEY SHARED FEATURES box at the bottom center: Both are estrogen-dependent | Both cause dysmenorrhea & pelvic pain | Can COEXIST in same patient | Both respond to hormonal suppression Use a clean, professional medical infographic style with readable fonts, color-coded sections, small anatomical icons, and clear visual hierarchy.
ENDOMETRIOSIS vs ADENOMYOSIS - At a Glance
| Feature | 🔵 ENDOMETRIOSIS | 🟣 ADENOMYOSIS |
|---|---|---|
| Definition | Endometrial glands + stroma outside the uterus | Endometrial glands + stroma inside the myometrium |
| Key concept | Ectopic tissue at distant/pelvic sites | Tissue invades the uterine muscle wall |
| Uterus size | Usually normal-sized | Enlarged, globular, thickened wall |
| Prevalence | ~10% of reproductive-age women; ~50% of infertile women | Commonly found at hysterectomy; exact prevalence underdiagnosed |
📍 Affected Sites
- Ovaries (chocolate cysts / endometriomas)
- Uterosacral ligaments
- Rectovaginal septum
- Cul-de-sac / Pouch of Douglas
- Pelvic peritoneum
- Bowel serosa (can mimic cancer)
- Cervix, vagina, fallopian tubes
- Distant sites: lung, brain, bone (rare)
- Confined to the myometrium only - nests of endometrial stroma and glands interposed between muscle bundles
⚙️ Pathogenesis
| Endometriosis | Adenomyosis | |
|---|---|---|
| Main theory | Retrograde menstruation (Sampson's theory) - menstrual tissue flows backward through the fallopian tubes and implants | Invagination of the endometrial basalis layer into the myometrium |
| Other theories | Benign metastasis (via blood/lymphatics), coelomic metaplasia, extrauterine stem cell differentiation | - |
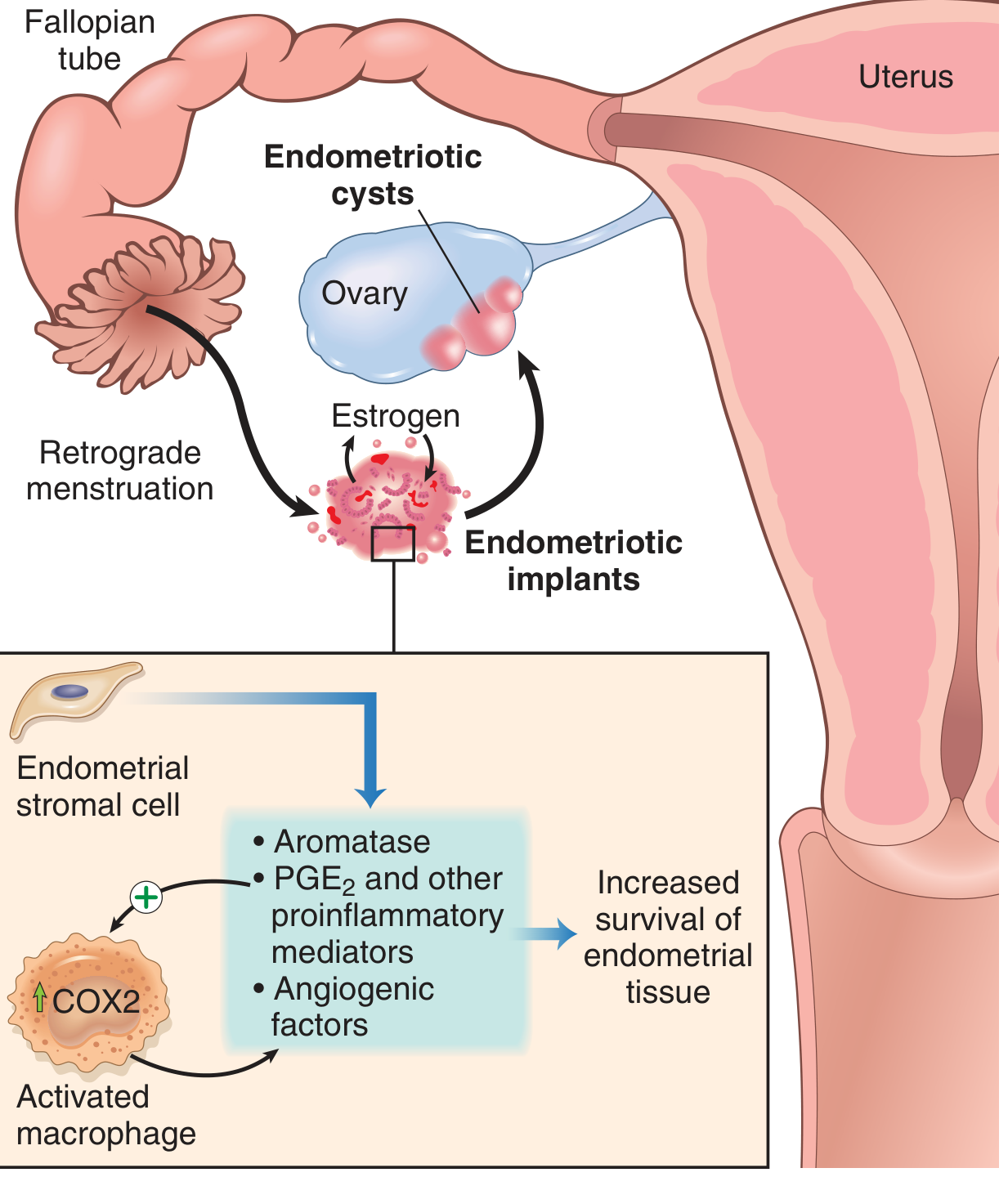
| Molecular | High aromatase → local estrogen production; PGE₂, VEGF, MMP upregulation; activated macrophages sustain implants | Estrogen-driven; reactive myometrial hypertrophy |
🩺 Symptoms
| Symptom | Endometriosis | Adenomyosis |
|---|---|---|
| Dysmenorrhea | ✅ Severe | ✅ Especially pre-menstrual |
| Pelvic pain | ✅ | ✅ |
| Dyspareunia (deep) | ✅ Classic | Less prominent |
| Menorrhagia (heavy bleeding) | Variable | ✅ Major feature |
| Infertility | ✅ 30-40% of patients | Can coexist with infertility |
| Dyschezia / rectal bleeding | ✅ (bowel disease) | Less common |
| Dysuria / haematuria | ✅ (bladder disease) | Less common |
🔬 Gross / Microscopic Appearances
- "Powder burn" / "gunshot" lesions - black, dark brown or bluish puckered nodules
- Red flame-like implants, clear vesicles
- Chocolate cysts (endometriomas) - ovarian cysts filled with thick dark-brown old blood (3-5 cm)
- Fibrous adhesions causing distorted pelvic anatomy

- Enlarged, globular uterus
- Thickened uterine wall (often asymmetric)
- Nests of endometrial tissue within the muscle on cross-section
🔬 Pathogenesis Diagram (Endometriosis)
🩻 Diagnosis
| Endometriosis | Adenomyosis | |
|---|---|---|
| Gold standard | Laparoscopy + histological biopsy | Histology (often post-hysterectomy) |
| Imaging | TVS/MRI for severe forms (endometriomas, deep disease) | MRI (junctional zone >12 mm), TVS (3+ MUSA criteria) |
| USS features | Endometrioma = thick-walled ovarian cyst | Enlarged globular uterus, myometrial cysts, echogenic subendometrial lesions, irregular junctional zone |
| MRI features | Haemosiderin deposits for deep disease | Thickened junctional zone |
💊 Treatment
| Approach | Endometriosis | Adenomyosis |
|---|---|---|
| Analgesia | NSAIDs, COX-2 inhibitors | NSAIDs |
| Hormonal suppression | GnRH agonists + add-back HRT, progestogens, LNG-IUS | Progestogens, LNG-IUS, GnRH agonists |
| Targeted medical | Aromatase inhibitors | Aromatase inhibitors |
| Surgery | Laparoscopic ablation/excision; conservative to preserve fertility | Hysterectomy (definitive) |
| Definitive | Hysterectomy + bilateral salpingo-oophorectomy + total disease excision | Hysterectomy |
⚠️ Cancer Risk
| Endometriosis | Adenomyosis | |
|---|---|---|
| Malignant potential | Ovarian + peritoneal forms → endometrioid carcinoma, clear cell carcinoma | Generally benign; very low risk |
| Deep infiltrating form | Extremely rare to transform | - |
🔗 Key Shared Features
Both conditions are estrogen-dependent | Both cause dysmenorrhea and pelvic pain | They frequently coexist in the same patient | Both respond to hormonal suppression | Both are diseases of reproductive age women
Search PubMed for recent research on adenomyosis stem cell origin and molecular pathways
adenomyosis stem cell origin pathogenesis
adenomyosis molecular pathways signaling
adenomyosis pathogenesis review
PMID: 41968335
PMID: 39595579
PMID: 38885960
PMID: 36736810
PMID: 38103509
PMID: 39125516
PMID: 40287215
PMID: 39936948
PMID: 34131719
Recent PubMed Research: Adenomyosis - Stem Cell Origin & Molecular Pathways
🔬 1. Cellular Origins - The Two Competing Theories
Theory A: Invagination of Basalis Endometrium (Best supported)
Endometrial cells from the deepest (basalis) layer invade the myometrium following disruption of the endometrial-myometrial junction (EMJ) - commonly after pregnancy or surgery.
[Review . 2021] Adenomyosis pathogenesis: insights from next-generation sequencing - Bulun SE et al., Human Reproduction Update [PMID: 34131719]
- KRAS mutations are found in both basalis endometrial glands AND adjacent adenomyotic epithelial cells of the same uterus - proving they share a common clonal origin
- The same KRAS mutations are also found in co-occurring endometriosis lesions, suggesting adenomyosis and endometriosis are oligoclonal tissues arising from the same endometrial cell population
- KRAS mutations drive progesterone resistance and prolonged cell survival in adenomyotic tissue
- Driver mutations found in uterine fibroids (smooth muscle origin) are absent in adenomyosis - confirming adenomyosis is epithelial, not myometrial, in origin
Theory B: Metaplastic Differentiation of Myometrial Stem/Progenitor Cells
Remnant stem/progenitor cells already within the myometrium undergo endometrial differentiation.
🧬 2. Stem Cell Evidence (Direct Studies)
[Study . 2024] NOTCH1- and CD117-Positive Stem Cells in Human Endometriosis and Adenomyosis Lesions - Metodiev D et al., Diagnostics [PMID: 39125516]
- Both NOTCH1+ and CD117+ stem cell markers are present in adenomyosis lesions - confirming a stem cell component
- However, endometriosis lesions had significantly higher proportions of both stem cell types than adenomyosis (NOTCH1+: 2.26% vs 0.13%, p=0.002; CD117+: 0.44% vs 0.26%, p=0.016)
- In endometriosis, NOTCH1+ and CD117+ cells are positively correlated (coordinated expansion); in adenomyosis, there is no such correlation
- Conclusion: the two conditions have distinct stem cell dynamics, supporting different developmental origins
🔗 3. Single-Cell Transcriptomics - Mapping the Molecular Landscape
WNT/SFRP Pathway (Landmark scRNA-seq study)
[Study . 2023] Adenomyosis: single-cell transcriptomic analysis reveals a paracrine mesenchymal-epithelial interaction involving the WNT/SFRP pathway - Yildiz S et al., Fertility & Sterility [PMID: 36736810]
- Endometrial fibroblasts (36% of endometrial cells) derive from pericyte progenitors - but in adenomyosis, the larger fibroblast population (50% of cells) shows no link to pericyte progenitors, suggesting a different origin
- A unique adenomyotic fibroblast population clusters transcriptomically with endometrial fibroblasts - supporting endometrial stromal cells as progenitors of adenomyosis
- Secreted Frizzled-Related Proteins (SFRP1, 2, 4) - natural WNT inhibitors - are upregulated in adenomyotic fibroblasts, disrupting normal WNT-driven cell signaling
- Multiple WNTs originating from fibroblasts target epithelial and endothelial cells via paracrine signaling networks
- Epithelial cells in adenomyosis show molecular evidence of progesterone resistance and diminished estrogen regulation
Broader Single-Cell Mapping
[Review . 2025] Mapping Human Uterine Disorders Through Single-Cell Transcriptomics - Boldu-Fernández S et al., Cells [PMID: 39936948]
- scRNA-seq has identified novel progenitor cell populations in adenomyosis linked to tissue invasion and neuroinflammation
- Fibroblast-to-myofibroblast transitions drive fibrosis and chronic inflammation
- Disrupted signaling: Wnt and VEGF pathways are consistently flagged
- Also: single-cell approaches identified prolactin receptor as a potential therapeutic target [PMID: 40804233]
⚙️ 4. Unified Molecular Framework (2026 Integrated Review)
[Review . 2026] Pathogenesis of Adenomyosis: An Integrated Review of Cellular Origins, Molecular Mechanisms, and Intersecting Diseases - Yang J et al., J Cell Mol Med [PMID: 41968335]
| Axis | Key Molecules | Effect |
|---|---|---|
| 1. Hormonal Dysregulation | Local aromatase → hyper-estrogenism; progesterone resistance; prolactin paracrine loop | Drives reactive myometrial hypertrophy |
| 2. Immune-Hemostatic Crosstalk | Activated platelets + M2-polarized macrophages → TGF-β1 signaling | Establishes pro-fibrotic niche |
| 3. Hypoxia & Neuroangiogenesis | HIF-1α stabilization → Warburg effect (metabolic reprogramming) + sensory nerve sprouting | Chronic pain mechanism |
| 4. Epigenetic Fibrosis | Oestrogen-Slug-VEGF axis + HDAC-mediated chromatin remodeling → Epithelial-Mesenchymal Transition (EMT) | Drives invasion and lesion persistence |
📡 5. Key Signaling Pathways - Full Map
[Review . 2024] Research Advances in Adenomyosis-Related Signaling Pathways and Promising Targets - Zhang H et al., Biomolecules [PMID: 39595579]
| Pathway | Role in Adenomyosis |
|---|---|
| CXCL/CXCR | Chemokine-driven cell recruitment and migration |
| NLRP3 inflammasome | Inflammatory cascade activation |
| NF-κB | Pro-inflammatory gene expression, cell survival |
| TGF-β/Smad | Fibrosis, EMT, tissue remodeling |
| VEGF | Angiogenesis, lesion vascularization |
| Hippo/YAP | Cell proliferation and organ growth control |
| PI3K/Akt/mTOR | Cell survival, proliferation, metabolism |
| JAK/STAT | Immune signaling, inflammatory response |
| WNT/SFRP | Stromal-epithelial crosstalk (see scRNA-seq above) |
| KRAS/MAPK | Driver mutation pathway - proliferation, progesterone resistance |
🔄 6. Stromal-Epithelial Crosstalk
[Review . 2024] Crosstalk between stromal and epithelial cells in adenomyosis - Zipponi M et al., Human Reproduction [PMID: 38885960]
- Dysregulated collective cell migration and epithelial-to-mesenchymal transition (EMT) drive lesion growth
- Non-coding RNAs and extracellular vesicles carry abnormal signals between stromal and epithelial cells
- Alterations in cell adhesion molecules are shared with deep endometriosis
- Cancer-driving mutations and epigenetic modifications are found in both adenomyosis and deep endometriosis - raising the question: are they differential phenotypes of the same disease?
[Review . 2024] Endometriosis and Adenomyosis: Similarities and Differences - Donnez J, Stratopoulou CA, Dolmans MM, Best Pract Res Clin Obstet Gynaecol [PMID: 38103509]
- Both conditions affect ~200 million women worldwide; both may derive from estrogen-dependent overproliferation with implantation at ectopic sites; they may represent differential phenotypes of one disease
🔭 7. Clinical Implications & New Therapeutics
[Review . 2025] Adenomyosis: The Missed Disease - Santulli P et al., Reprod Biomed Online [PMID: 40287215]
- Adenomyosis is increasingly diagnosed in young women and adolescents (not just multiparous women over 40)
- Pathogenesis framework: genetic/epigenetic background + estrogen-progesterone receptor imbalance + local immune dysfunction + fibrosis + neuroangiogenesis
- Often co-exists with endometriosis and uterine fibroids
- Still lacks shared diagnostic criteria and management recommendations
- Anti-platelet agents (targeting immune-hemostatic axis)
- Dopamine agonists (targeting prolactin paracrine loop)
- HDAC inhibitors (targeting epigenetic fibrosis)
- PI3K/Akt/mTOR inhibitors
- Anti-VEGF strategies
Summary Table
| Topic | Key Finding | Best Paper |
|---|---|---|
| Origin (genetics) | KRAS mutations shared between basalis endometrium & adenomyosis → invagination theory | Bulun 2021 [PMID: 34131719] |
| Stem cells (markers) | NOTCH1+/CD117+ stem cells present but lower than in endometriosis; distinct dynamics | Metodiev 2024 [PMID: 39125516] |
| scRNA-seq | WNT/SFRP paracrine network; pericyte-independent fibroblast origin | Yildiz 2023 [PMID: 36736810] |
| Unified framework | TIAR/EMID → 4-axis vicious cycle (hormonal, immune-hemostatic, hypoxia, epigenetic) | Yang 2026 [PMID: 41968335] |
| Signaling pathways | NLRP3, NF-κB, TGF-β, VEGF, PI3K/Akt/mTOR, JAK/STAT, WNT, KRAS | Zhang 2024 [PMID: 39595579] |
| Shared with endometriosis | Same KRAS clones, EMT, epigenetic changes - possibly same disease, different phenotypes | Donnez 2024 [PMID: 38103509] |
| Clinical update | Young women increasingly affected; lifelong management needed; new non-hormonal targets | Santulli 2025 [PMID: 40287215] |
instrument with their image there identification and there use with there sterilization Artery Forceps different sizes
artery forceps different sizes identification uses sterilization surgical instrument
Halstead mosquito Kelly Crile Spencer Wells artery forceps identification sizes uses image
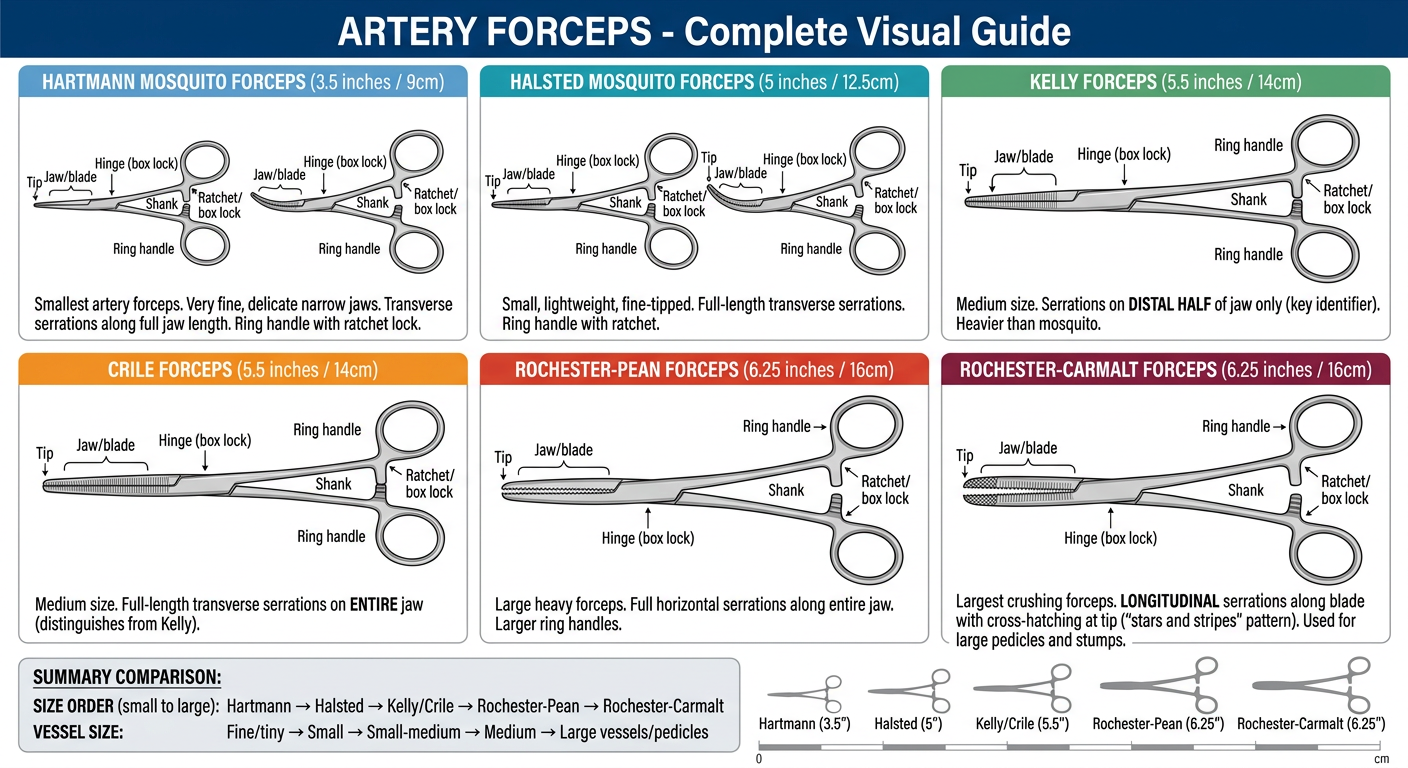
A detailed medical surgical instrument reference chart titled "ARTERY FORCEPS - Complete Visual Guide" on a clean white background. The chart shows 6 types of artery forceps arranged in a grid, each with a clear line-drawing style illustration of the instrument and labeled sections: 1. HARTMANN MOSQUITO FORCEPS (3.5 inches / 9cm) - Smallest artery forceps - Very fine, delicate narrow jaws - Transverse serrations along full jaw length - Ring handle with ratchet lock - Show both STRAIGHT and CURVED versions side by side - Color code: LIGHT BLUE 2. HALSTED MOSQUITO FORCEPS (5 inches / 12.5cm) - Small, lightweight, fine-tipped - Full-length transverse serrations - Ring handle with ratchet - Show STRAIGHT and CURVED - Color code: TEAL 3. KELLY FORCEPS (5.5 inches / 14cm) - Medium size - Serrations on DISTAL HALF of jaw only (key identifier) - Heavier than mosquito - Show STRAIGHT and CURVED - Color code: GREEN 4. CRILE FORCEPS (5.5 inches / 14cm) - Medium size - Full-length transverse serrations on ENTIRE jaw (distinguishes from Kelly) - Show STRAIGHT and CURVED - Color code: ORANGE 5. ROCHESTER-PEAN FORCEPS (6.25 inches / 16cm) - Large heavy forceps - Full horizontal serrations along entire jaw - Larger ring handles - Color code: RED 6. ROCHESTER-CARMALT FORCEPS (6.25 inches / 16cm) - Largest crushing forceps - LONGITUDINAL serrations along blade with cross-hatching at tip ("stars and stripes" pattern) - Used for large pedicles and stumps - Color code: DARK RED/BURGUNDY Below each instrument drawing, add small labeled annotations pointing to: - Ring handle - Ratchet/box lock - Shank - Hinge (box lock) - Jaw/blade - Tip At the bottom, a summary comparison table: SIZE ORDER (small to large): Hartmann → Halsted → Kelly/Crile → Rochester-Pean → Rochester-Carmalt VESSEL SIZE: Fine/tiny → Small → Small-medium → Medium → Large vessels/pedicles Clean white background, professional medical illustration style, instruments shown in silver/metallic gray with color-coded name labels for each type. Include a size comparison silhouette bar showing relative lengths.
ARTERY FORCEPS - Complete Reference Guide
🔩 Anatomy of All Artery Forceps
Ring handles ──► [O] [O]
Ratchet/teeth ──► |||
Shanks ──────────► | |
Box lock (hinge) ─► ✕
Blade/jaw ───────► ═══
Tip ─────────────► ●
| Part | Function |
|---|---|
| Ring handles | Finger loops for grip and control |
| Ratchet (box lock) | Locking mechanism - holds jaws closed at variable pressure (1st, 2nd, 3rd tooth) |
| Shanks | Connect handles to box lock |
| Box lock / hinge | Pivot point; most vulnerable to wear |
| Jaw/blade | Serrated gripping surface |
| Tip | Fine end for vessel clamping |
⚠️ The ratchet is the key distinguishing feature from tissue forceps - it keeps the clamp locked without the surgeon holding it.
1. 🔵 HARTMANN MOSQUITO FORCEPS
| Feature | Detail |
|---|---|
| Also known as | Baby mosquito, Hartman forceps |
| Length | 9 cm (3.5 inches) - SMALLEST |
| Jaw serrations | Fine transverse serrations, full jaw length |
| Tip shape | Straight OR curved |
| Material | Stainless steel |
- Clamping tiny capillaries and minute bleeding points
- Neonatal and paediatric surgery
- Ophthalmic and microsurgery
- Fine tissue dissection in very shallow wounds
- Holding fine sutures
2. 🩵 HALSTED MOSQUITO FORCEPS
| Feature | Detail |
|---|---|
| Also known as | Mosquito clamp, Halstead forceps |
| Length | 12.5 cm (5 inches) |
| Jaw serrations | Transverse, full jaw length |
| Tip shape | Straight OR curved |
- Clamping small blood vessels and capillaries
- Holding delicate suture material
- Fine tissue dissection
- Superficial haemostasis
- General and plastic surgery
3. 🟢 KELLY FORCEPS
| Feature | Detail |
|---|---|
| Also known as | Kelly haemostat, Kelly clamp |
| Length | 14 cm (5.5 inches) |
| Jaw serrations | Transverse on DISTAL HALF only ← KEY identifier |
| Tip shape | Straight OR curved |
- Clamping small-to-medium blood vessels
- Grasping and holding fatty tissue
- General surgery (abdominal, gynaecology, urology, orthopaedics)
- Tissue dissection
- Holding gauze or sponges
4. 🟠 CRILE FORCEPS
| Feature | Detail |
|---|---|
| Also known as | Crile haemostat, Crile-Rankin forceps |
| Length | 14 cm (5.5 inches) |
| Jaw serrations | Transverse along ENTIRE jaw length ← KEY identifier |
| Tip shape | Straight OR curved |
- Clamping small-to-medium vessels
- General, vascular, paediatric, and reconstructive surgery
- Microsurgical and soft tissue procedures
- Broader grip than Kelly due to full serrations
5. 🔴 ROCHESTER-PEAN FORCEPS
| Feature | Detail |
|---|---|
| Also known as | Rochester Pean, Pean forceps |
| Length | 16 cm (6.25 inches) |
| Jaw serrations | Full horizontal serrations along entire jaw |
| Tip shape | Straight OR curved |
- Clamping large blood vessels
- Controlling haemorrhage in major surgery
- Abdominal, thoracic, and vascular surgery
- Grasping large tissue bundles
6. 🟤 ROCHESTER-CARMALT FORCEPS
| Feature | Detail |
|---|---|
| Also known as | Carmalt clamp, "stars and stripes" haemostat |
| Length | 16 cm (6.25 inches) - LARGEST |
| Jaw serrations | LONGITUDINAL serrations along blade + cross-hatching at tip ← UNIQUE identifier |
| Tip shape | Straight OR curved |
- Crushing and clamping large tissue pedicles
- Stump ligation before amputation
- Clamping large vascular structures (e.g. ovarian pedicle, appendix base)
- Major abdominal and gynaecological surgery
📐 Size & Use Summary - At a Glance
| Forceps | Size | Vessel Size | Serration Pattern | Key Use |
|---|---|---|---|---|
| Hartmann Mosquito | 9 cm (3.5") | Tiny capillaries | Full, fine | Neonatal/microsurgery |
| Halsted Mosquito | 12.5 cm (5") | Small vessels | Full, horizontal | General fine haemostasis |
| Kelly | 14 cm (5.5") | Small-medium | Distal half only | General surgery |
| Crile | 14 cm (5.5") | Small-medium | Full length | Vascular/general |
| Rochester-Pean | 16 cm (6.25") | Medium-large | Full, heavy | Major vessel clamping |
| Rochester-Carmalt | 16 cm (6.25") | Large pedicles | Longitudinal + cross-hatch | Pedicle ligation |
🧹 STERILIZATION
Step 1 - Pre-cleaning (CRITICAL)
- Open all ratchets fully before cleaning - never autoclave in locked position (damages box lock)
- Rinse immediately after use to prevent blood/protein drying
- Ultrasonic cleaner or enzymatic soak to remove organic material from serrations
- Rinse with distilled water and dry thoroughly
Step 2 - Sterilization Methods
| Method | Temperature/Parameters | Best For | Notes |
|---|---|---|---|
| Steam Autoclave (moist heat) | 134°C / 3 min (porous) OR 121°C / 15 min | ✅ Gold standard - all metal artery forceps | Instruments must be open/unlocked and placed in mesh trays. Fully penetrates serrations. |
| Pre-vacuum autoclave | 134°C / 3.5 min | High-throughput theatre sets | More efficient steam penetration |
| Chemical (cold) sterilization | Glutaraldehyde 2% / 10 hours | Heat-sensitive items; also valid for metal | Rinse thoroughly before use; toxic residue risk |
| Hydrogen peroxide plasma (STERRAD) | 45-50°C | Mixed instrument trays | Not suitable if lumen present |
| Dry heat | 160°C / 2 hours | Metal-only sets | Less common; longer cycle |
| Ethylene oxide (EtO) | 55-60°C | Heat/moisture sensitive | Long aeration time needed; less used now |
Step 3 - After Sterilization
- Inspect jaw alignment, ratchet function, and tip condition before use
- Store in sterile wrapping or closed trays
- Estimated instrument lifespan: 300-900 sterilization cycles
- Replace when: box lock cracks, jaws misalign, ratchet slips, or tips are damaged
⚠️ Key Rules
- Never autoclave with jaws locked - the ratchet pressure + steam expansion cracks the box lock
- Never use artery forceps to clamp rubber tubing - use tube-occluding clamps instead
- Inspect serrations after each sterilization cycle for protein buildup (biofilm risk)
- Lubricate hinges with instrument-grade (water-soluble) oil before autoclaving if needed
I need this information in poster form so consize and make in only One page with images and I say point
A professional one-page medical educational poster titled "ARTERY FORCEPS" in bold white text on a deep navy blue header banner. Subtitle: "Identification • Uses • Sterilization" in gold/yellow. The poster is divided into 3 horizontal sections on a light gray background: ───────────────────────────────────────────────────────── SECTION 1 — TOP: "TYPES & IDENTIFICATION" (teal section header) ───────────────────────────────────────────────────────── Six instrument cards in a row, each showing a REALISTIC metallic silver line illustration of the forceps (both straight and curved side by side), with the name on top in bold and bullet points below: Card 1 — HARTMANN MOSQUITO (light blue border) Drawing: tiny, ultra-fine forceps 9cm • 9 cm (3.5") — SMALLEST • Full jaw serrations • Straight & curved • Identifies: finest tip of all Card 2 — HALSTED MOSQUITO (teal border) Drawing: fine mosquito forceps 12.5cm • 12.5 cm (5") • Full horizontal serrations • Straight & curved • Identifies: lightweight, delicate Card 3 — KELLY (green border) Drawing: medium forceps 14cm • 14 cm (5.5") • Serrations: DISTAL HALF only ← key ID • Straight & curved • Identifies: half-serrated jaw Card 4 — CRILE (orange border) Drawing: medium forceps 14cm • 14 cm (5.5") • Full-length serrations ← key ID • Straight & curved • Identifies: like Kelly but full jaw Card 5 — ROCHESTER-PEAN (red border) Drawing: large heavy forceps 16cm • 16 cm (6.25") • Full heavy serrations • Large ring handles • Identifies: large & heavy Card 6 — ROCHESTER-CARMALT (dark burgundy border) Drawing: large forceps with distinct groove pattern • 16 cm (6.25") — LARGEST • LONGITUDINAL serrations + cross-hatch tip • "Stars & stripes" pattern ← unique ID • For large pedicles only Below the six cards, one clean SIZE RULER graphic showing relative sizes from smallest to largest with arrows: Hartmann → Halsted → Kelly = Crile → Pean = Carmalt ───────────────────────────────────────────────────────── SECTION 2 — MIDDLE: "USES" (green section header) ───────────────────────────────────────────────────────── A compact 3-column layout: Column A — ALL TYPES (general uses with a scissors/forceps icon): • Clamp & occlude bleeding vessels • Haemostasis during surgery • Grasp & hold tissue/fascia • Expose deep surgical sites • Hold suture material Column B — BY SIZE (with graduated arrow icon small→large): • Mosquito → tiny capillaries, fine sutures, microsurgery, neonates • Kelly/Crile → small-medium vessels, general/gynae/urology • Pean/Carmalt → large vessels, pedicle ligation, major abdominal surgery Column C — ⚠️ NEVER USE FOR (red warning icon): • Do NOT clamp rubber tubes (cracks box lock) • Do NOT over-clamp (damages ratchet) • Do NOT use as needle holder • Always check jaw alignment before use ───────────────────────────────────────────────────────── SECTION 3 — BOTTOM: "STERILIZATION" (purple section header) ───────────────────────────────────────────────────────── Four steps shown as numbered boxes in a horizontal process flow with arrows between them: STEP 1 — PRE-CLEAN (blue box with water drop icon) • Open ratchet FULLY • Rinse immediately post-use • Enzymatic soak or ultrasonic clean • Remove blood from serrations • Rinse with distilled water & dry STEP 2 — STERILIZE (orange box with autoclave icon) ★ GOLD STANDARD: Steam Autoclave • 134°C / 3 min (pre-vacuum) • OR 121°C / 15 min (gravity) • Instruments OPEN/UNLOCKED in mesh tray Other options: • Chemical (glutaraldehyde 2%/10h) • H₂O₂ plasma (STERRAD) • Ethylene oxide (EtO) STEP 3 — INSPECT (green box with magnifier icon) • Check jaw alignment • Test ratchet click • Inspect tip for damage • Check box lock for cracks • Lifespan: 300–900 cycles STEP 4 — STORE (purple box with package icon) • Wrap in sterile packaging • Store in closed sterile tray • Label with sterilization date • Replace if jaws misalign or ratchet slips ───────────────────────────────────────────────────────── FOOTER BAR (navy): "All artery forceps = stainless steel | Autoclavable | Always sterilize OPEN (ratchet unlocked)" ───────────────────────────────────────────────────────── Style: clean modern medical infographic, navy/teal/white color scheme, bold readable fonts, realistic metallic instrument illustrations, professional hospital educational poster quality, A3 landscape orientation.
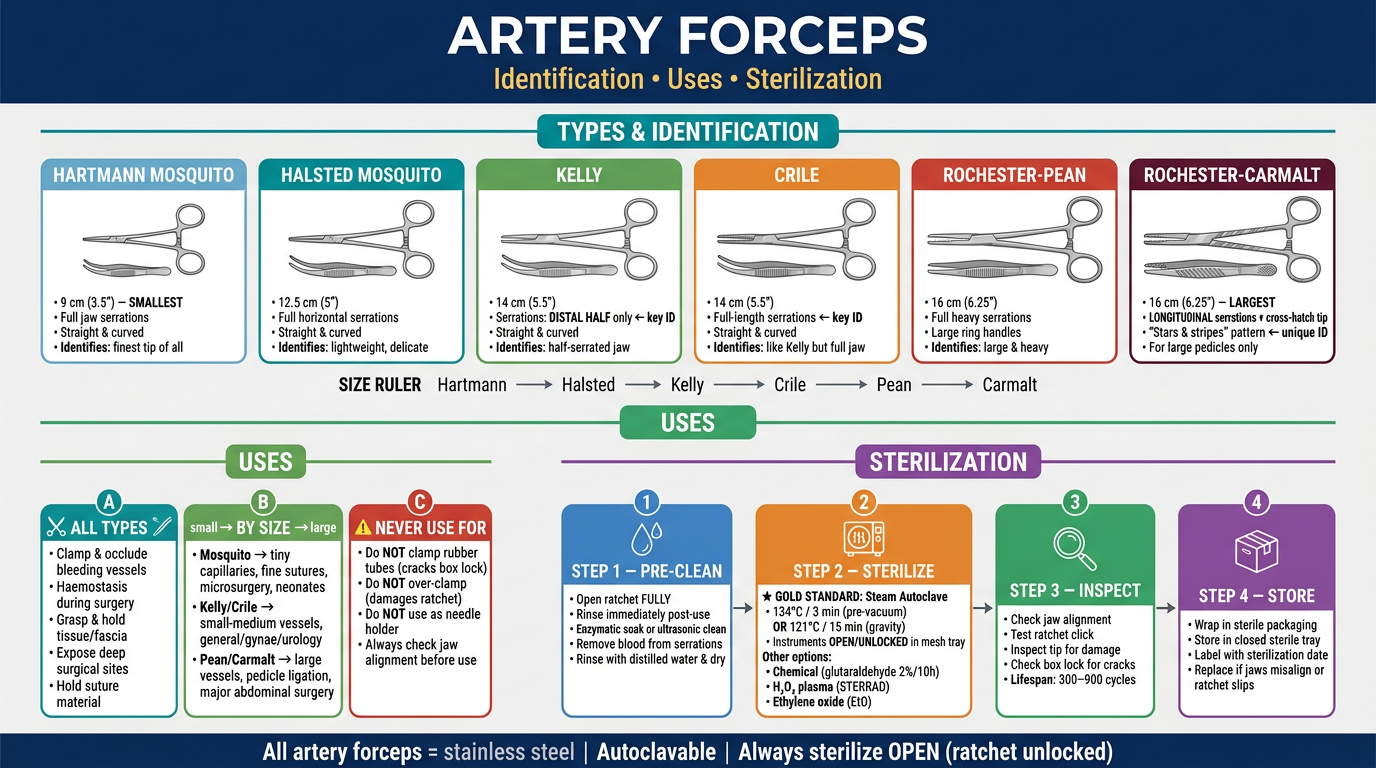
- Top section - all 6 types with instrument illustrations, sizes, and key identification points
- Middle section - uses by type and what NOT to do (warnings)
- Bottom section - 4-step sterilization process (pre-clean → sterilize → inspect → store)
- Footer - the golden rule: always autoclave with ratchet open/unlocked
- Hartmann = tiniest (9 cm)
- Halsted = small, fully serrated (12.5 cm)
- Kelly = distal half serrations only
- Crile = full-length serrations (same size as Kelly)
- Rochester-Pean = large, heavy, full serrations
- Rochester-Carmalt = longitudinal "stars & stripes" pattern - largest crushing clamp
Make a quick-reference laminated wallet card on artery forceps
A laminated wallet card design showing FRONT and BACK side by side, credit card size (85mm x 54mm each), with a thin white border gap between them, on a neutral background. ═══════════════════════════════════════════════════════ FRONT CARD (left side) — deep navy blue background ═══════════════════════════════════════════════════════ TOP HEADER (gold/yellow band): 🔧 ARTERY FORCEPS Quick Reference Card Main content — 6 rows, each in a colored left-border strip: ┃🔵 HARTMANN MOSQUITO 9cm • Full serrations • Tiny capillaries • Neonates ┃🩵 HALSTED MOSQUITO 12.5cm • Full serrations • Small vessels • Fine sutures ┃🟢 KELLY 14cm • Distal ½ serrations only • Sm-Med vessels ┃🟠 CRILE 14cm • Full serrations • Sm-Med vessels • Vascular ┃🔴 ROCHESTER-PEAN 16cm • Full heavy serrations • Large vessels ┃🟤 CARMALT 16cm • LONGITUDINAL grooves • Pedicle ligation SIZE BAR at bottom: ◄─────────────────────────────► Hartmann → Halsted → Kelly=Crile → Pean=Carmalt SMALLEST ←——————————→ LARGEST Very tiny footer in white: Both straight & curved available ═══════════════════════════════════════════════════════ BACK CARD (right side) — dark teal/dark green background ═══════════════════════════════════════════════════════ TOP HEADER (orange band): ⚕ USES & STERILIZATION USES section (white text, compact): ALL TYPES: • Clamp bleeding vessels • Hold tissue • Expose surgical site • Hold sutures BY SIZE: • Mosquito → fine/capillary haemostasis • Kelly/Crile → general surgery • Pean/Carmalt → major vessels & pedicles ⚠️ NEVER: clamp tubing | use as needle holder DIVIDER LINE STERILIZATION (numbered, ultra-compact): 1️⃣ OPEN ratchet fully before cleaning 2️⃣ Enzymatic soak → rinse → dry 3️⃣ AUTOCLAVE: 134°C/3min OR 121°C/15min (instruments OPEN in mesh tray) 4️⃣ Inspect jaws + ratchet before use 5️⃣ Lifespan: 300–900 cycles GOLD RULE BOX (bright yellow box, black text): ⭐ ALWAYS autoclave UNLOCKED ⭐ ⭐ REPLACE if jaws misalign ⭐ Tiny footer: All types = 420 stainless steel | Autoclavable ═══════════════════════════════════════════════════════ Style: crisp laminated card look, glossy finish appearance, rounded corners on both cards, very compact readable text, white and light colored text on dark backgrounds, color-coded strips for each forceps type, professional medical pocket reference card aesthetic, realistic card dimensions.
400, message: Got more than 4194304 bytes when reading: b'data: {"candidates": [{"content": {"role": "model","parts": [{"inlineData": {"mimeType": "image/png"...'.
We encountered an error while processing your request. Please try again or reach out to us for help.
Ye poster vertical form A4 size me bna do na
A professional A4 size PORTRAIT/VERTICAL orientation medical educational poster. Clean, modern design. HEADER (full width, deep navy blue background): Title in large bold white text: ARTERY FORCEPS Subtitle in gold: Identification • Uses • Sterilization Small text in white: Haemostatic Instruments Quick Reference ══════════════════════════════════════════ SECTION 1 — "TYPES & IDENTIFICATION" (teal left-accent bar, white background section) ══════════════════════════════════════════ Two columns × 3 rows = 6 instrument cards, stacked vertically in 2 columns: LEFT COLUMN: [Card 1 — light blue border] HARTMANN MOSQUITO [illustration: tiny fine straight+curved forceps, silver metallic] • 9 cm (3.5") — SMALLEST • Full serrations, entire jaw • Tiny capillaries, neonates • Micro & ophthalmic surgery [Card 2 — teal border] HALSTED MOSQUITO [illustration: fine mosquito forceps, silver] • 12.5 cm (5") • Full horizontal serrations • Small vessels & fine sutures • General & plastic surgery [Card 3 — green border] KELLY [illustration: medium forceps, silver] • 14 cm (5.5") • ★ Distal HALF serrations only • Small–medium vessels • General, gynae, urology RIGHT COLUMN: [Card 4 — orange border] CRILE [illustration: medium forceps, silver] • 14 cm (5.5") • ★ FULL-length serrations • Small–medium vessels • Vascular & reconstructive [Card 5 — red border] ROCHESTER-PEAN [illustration: large heavy forceps, silver] • 16 cm (6.25") • Full heavy serrations • Large vessels • Major abdominal surgery [Card 6 — dark burgundy border] ROCHESTER-CARMALT [illustration: large forceps with longitudinal groove pattern, silver] • 16 cm (6.25") — LARGEST • ★ LONGITUDINAL grooves + cross-hatch tip • Large pedicle ligation • "Stars & stripes" pattern SIZE COMPARISON BAR (full width, gradient small→large): ◄ SMALLEST ——————————————————————— LARGEST ► Hartmann → Halsted → Kelly = Crile → Pean = Carmalt (9cm) (12.5cm) (14cm) (14cm) (16cm) (16cm) ══════════════════════════════════════════ SECTION 2 — "USES" (green left-accent bar) ══════════════════════════════════════════ Three compact columns: Column 1 — ALL TYPES (scissors icon): • Clamp & occlude bleeding vessels • Achieve haemostasis • Grasp & hold tissue/fascia • Expose deep surgical fields • Hold suture material Column 2 — BY SIZE (arrow icon): Mosquito → capillaries, fine sutures, microsurgery, paediatrics Kelly/Crile → small-medium vessels, general/gynae/ENT Pean/Carmalt → large vessels, pedicles, major surgery Column 3 — ⚠️ NEVER (red warning): ✗ Clamp rubber/silicone tubes ✗ Use as needle holder ✗ Over-clamp (damages ratchet) ✗ Autoclave with jaws LOCKED ══════════════════════════════════════════ SECTION 3 — "STERILIZATION" (purple left-accent bar) ══════════════════════════════════════════ Four steps in horizontal numbered boxes with arrows between: ① PRE-CLEAN (blue box, water icon) • Open ratchet FULLY • Rinse immediately post-use • Enzymatic soak • Ultrasonic clean • Rinse distilled water & dry ② STERILIZE (orange box, autoclave icon) ★ GOLD STANDARD: Steam Autoclave 134°C / 3 min OR 121°C / 15 min Instruments OPEN in mesh tray Others: Chemical, H₂O₂ plasma, EtO ③ INSPECT (green box, magnifier icon) • Jaw alignment • Ratchet function • Box lock integrity • Tip damage check • Life: 300–900 cycles ④ STORE (purple box, package icon) • Sterile wrap/tray • Label sterilization date • Replace if: – Jaws misalign – Ratchet slips – Box lock cracked ══════════════════════════════════════════ FOOTER (full width, navy blue): All types: 420 Stainless Steel | Fully Autoclavable | Always sterilize OPEN (ratchet unlocked) ══════════════════════════════════════════ Style: A4 portrait orientation, clean professional hospital poster, navy/teal/white color scheme, realistic metallic silver instrument illustrations in each card, bold readable fonts, color-coded instrument cards, modern infographic aesthetic, print-ready quality.
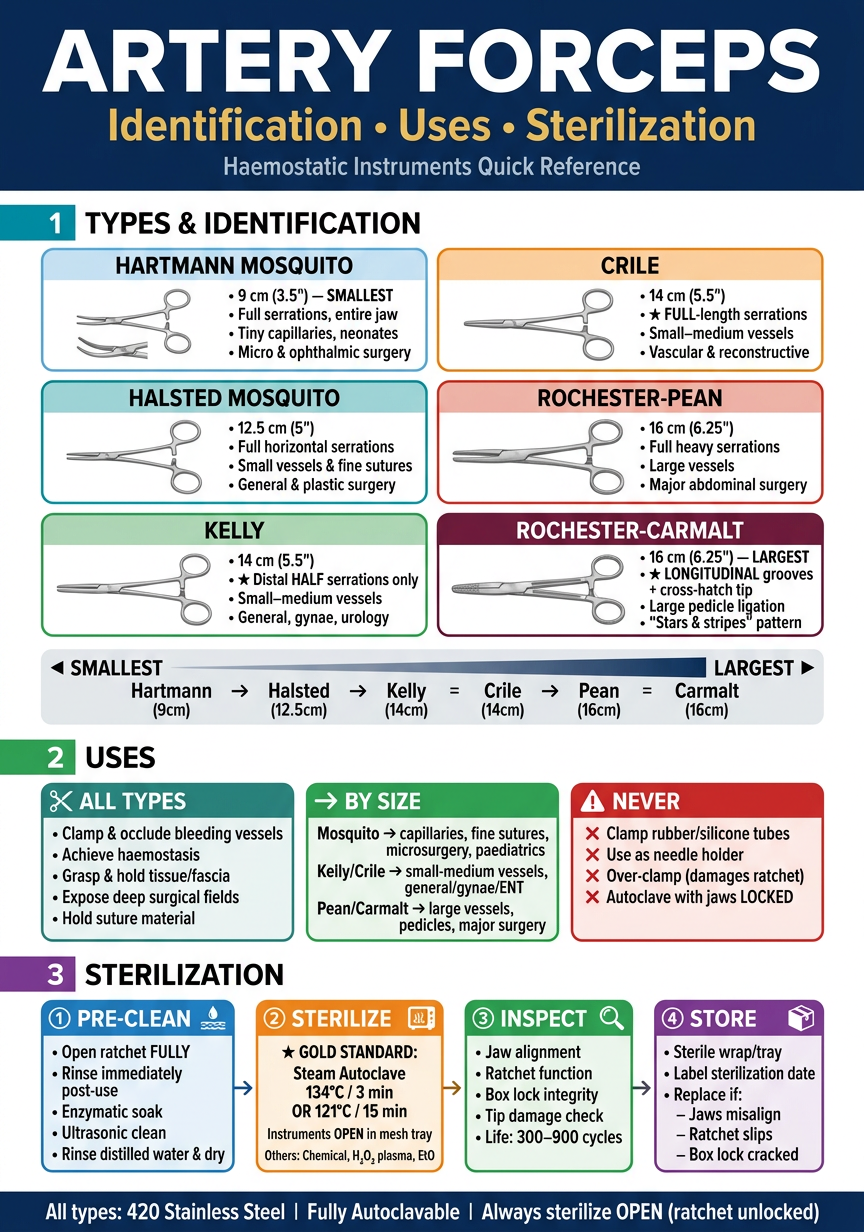
- Types & Identification - 6 forceps ke illustrations + size, serration pattern, aur key ID points
- Uses - sabke common uses + size ke hisaab se uses + ⚠️ warning (kya NAHI karna)
- Sterilization - 4 steps: Pre-clean → Autoclave → Inspect → Store
- Hartmann = sabse chota (9cm)
- Halsted = fine, full serrations (12.5cm)
- Kelly = aadha jaw serrated
- Crile = poora jaw serrated (Kelly jaisa size)
- Pean = bada, heavy
- Carmalt = longitudinal lines - bilkul alag dikhta hai