Melasma treatment
Reading File
Finding Sources
Searching PubMed
melasma treatment
Searching the Web
melasma treatment guidelines 2025 topical systemic procedures
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive, structured overview of melasma treatment based on Fitzpatrick's Dermatology, Dermatology 2-Volume Set (5e), Andrews' Diseases of the Skin, and current 2025 evidence.
Melasma: Treatment
Overview
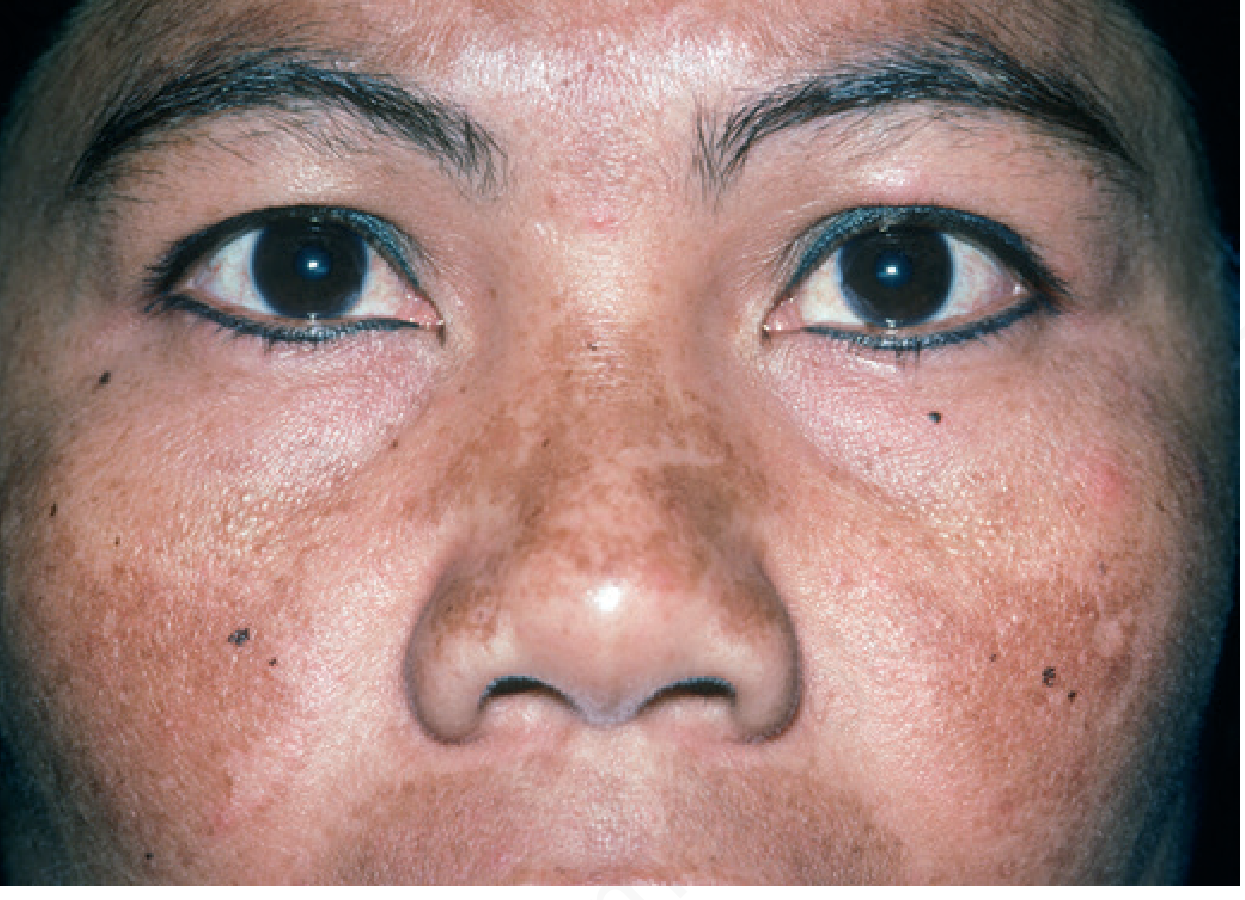
Melasma is a chronic, relapsing acquired hyperpigmentation disorder. It disproportionately affects women (>90%) and darker skin types (Fitzpatrick IV-VI), particularly Hispanic, Asian, and Black individuals. Triggers include UV/visible light, female hormones (pregnancy, OCP, HRT), and certain drugs (phenytoin, finasteride). Treatment is chronic - relapse after stopping therapy is the rule, not the exception.
Step 1: Photoprotection (Foundation of All Treatment)
This is non-negotiable and must continue indefinitely.
- Broad-spectrum SPF ≥30 daily, with UVA coverage - physical blockers (zinc oxide, titanium dioxide) preferred
- Tinted sunscreens containing iron oxide are preferred because visible light (not just UV) drives pigmentation in melasma
- Sun-protective clothing and hats
- Camouflage makeup with iron oxide
- Discontinue OCPs or HRT if clinically feasible
Sunscreen alone produces modest improvement but significantly enhances the efficacy of all other treatments.
Step 2: First-Line Topical Therapies
Triple Combination ("Kligman's Formula") - Gold Standard
Hydroquinone 4% + tretinoin 0.05-0.1% + mild corticosteroid (class 5-7)
- Most effective topical regimen available
- Applied at bedtime
- Results take up to 6 months
- Use daily for 2-4 months, then reduce to 1-2x/week for maintenance
- Risks of overuse: exogenous ochronosis (HQ), perioral dermatitis and atrophy (corticosteroid), acneiform eruption, hypertrichosis
Hydroquinone (HQ) Alone
- 2% OTC; 4% prescription
- Inhibits tyrosinase, the rate-limiting enzyme in melanin synthesis
- Moderately effective as monotherapy; best combined with retinoid
- Long-term daily use risks exogenous ochronosis (especially in darker skin)
Azelaic Acid (15-20%)
- Competitive tyrosinase inhibitor; also anti-inflammatory
- Well tolerated; safe in pregnancy
- Comparable to 4% HQ in several trials
Topical Retinoids (Tretinoin)
- Reduces melasma but less effective than HQ alone
- Acts by increasing epidermal turnover and dispersing melanin granules
- Can cause initial irritation - advise patients to expect this
Step 3: Adjunctive Topical Agents
| Agent | Mechanism | Concentration |
|---|---|---|
| Tranexamic acid (TXA) | Blocks UV-induced plasminogen activation; reduces prostaglandin-driven melanogenesis | 2-5% |
| L-ascorbic acid (Vitamin C) | Tyrosinase inhibitor, antioxidant | 10-15% |
| Kojic acid | Copper chelation, tyrosinase inhibition | 1-4% |
| Niacinamide | Inhibits melanosome transfer to keratinocytes | 4% |
| Cysteamine | Potent antioxidant, competes with DOPA in melanin synthesis | 5% |
| Thiamidol | Highly selective tyrosinase inhibitor; newer agent | varies |
| Glycolic acid | Chemical exfoliant; enhances penetration of other agents | 10-20% |
A 2023 systematic review (PMID 37128827) confirmed topical vitamin C improves melasma, though evidence quality remains moderate.
Step 4: Systemic Therapy
Oral Tranexamic Acid (TXA) - Major Advance
- Dose: 250 mg BID for 8-12 weeks
- Mechanism: inhibits UV-induced plasminogen activation, reducing arachidonic acid and prostaglandin E2 production in keratinocytes, which drives melanogenesis
- Particularly effective for moderate-to-severe or refractory melasma, used as an adjunct to topical therapy + photoprotection
- Screen for contraindications before prescribing: history of thrombosis, thrombophilia, pregnancy, current estrogen-containing contraception
- A multicenter propensity score-matched cohort found no association between oral TXA for melasma and thromboembolism in appropriately screened patients (StatPearls 2025 update)
- A 2025 RCT compared oral vs. topical TXA directly, showing comparable efficacy
Step 5: Procedural Therapies (Second/Third Line)
Use only after topical treatment is established. Always pre-treat with HQ or retinoid for ≥2 weeks to reduce post-procedure hyperpigmentation risk. Always perform a test spot first in darker skin types.
Chemical Peels (Second-Line)
- Glycolic acid (start 30%, titrate up) or salicylic acid (20-30%) every 4-6 weeks
- TCA, tretinoin 1% peels also used
- Important: peels alone do not reproducibly improve on 4% HQ and carry hyperpigmentation risk if irritation occurs
- A 2024 systematic review (PMID 38530985) confirmed efficacy of chemical peels as adjuncts but highlighted relapse risk
Laser and Light Therapies (Third-Line)
These must be used with great caution, particularly in darker skin types:
| Modality | Notes |
|---|---|
| Low-fluence Q-switched Nd:YAG (1064 nm) | Most studied; can worsen if settings are too aggressive; risk of punctate leukoderma |
| IPL (intense pulsed light) | Can improve melasma but high relapse rate |
| Non-ablative fractional laser | Adjunct option; risk of PIH in darker skin |
| Pulsed dye laser | May enhance combination topical treatment |
| Picosecond lasers | Emerging data; lower thermal injury profile |
The 2025 Delphi consensus (Sarkar et al., J Eur Acad Dermatol Venereol 2025) and the 2025 Melanin Hyperpigmentation global guideline both support Q-switched Nd:YAG as the primary laser option, with careful patient selection.
Long-Term Maintenance
Melasma recurs; maintenance is essential:
- Daily SPF ≥30 tinted sunscreen - indefinitely
- Topical retinoid (e.g. tretinoin 0.025-0.05%, 2-3x/week)
- Topical alpha-hydroxy acid (glycolic acid cream)
- Other agents rotated: L-ascorbic acid, azelaic acid, kojic acid, TXA 2-5%
- Triple combination HQ/retinoid/steroid reduced to 1-2x/week
- Minimize/eliminate hormonal triggers if possible
Special Considerations
- Pregnancy (chloasma): Azelaic acid and topical retinoids (carefully, avoid high-strength tretinoin) are safest; HQ is category C - avoid if possible; melasma often resolves months post-partum
- Darker skin types (IV-VI): Aggressive peels and lasers carry high PIH risk; prefer topical-first approach; use low-fluence laser settings with test spots
- Exogenous ochronosis: Paradoxical darkening from long-term HQ overuse - banana-shaped yellow-brown deposits on histology; switch to non-HQ alternatives if suspected
- Dermal melasma: Less responsive to all therapies than epidermal type; regardless of Wood's lamp findings, a therapeutic trial is always warranted
Evidence Summary (Recent PubMed, 2023-2025)
| PMID | Year | Topic |
|---|---|---|
| 37128827 | 2023 | Topical Vitamin C - systematic review confirms benefit in melasma |
| 38530985 | 2024 | Chemical peels for melasma - systematic review |
| 39444151 | 2025 | Glutathione as skin-lightening agent - systematic review |
Sources: Andrews' Diseases of the Skin p.993-994 | Dermatology 2-Volume Set 5e (Dermatology Vol. 2 Table 67.4) | Fitzpatrick's Dermatology | 2025 Melanin Hyperpigmentation Global Guideline | StatPearls 2025
This is a shared conversation. Sign in to Orris to start your own chat.