Erythropoiesis physiology answer in detailed and simple explanation with flowcharts regulation and origin and formation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full detailed answer.
Erythropoiesis: Complete Physiology Guide
What is Erythropoiesis?
Erythropoiesis is the process of red blood cell (RBC) formation. It is a tightly regulated, continuous process occurring primarily in the red bone marrow of adults. Under normal conditions, approximately 2.5 to 3 million RBCs are produced every second, replacing about 1% of circulating erythrocytes daily (roughly 250 billion cells). Each RBC lives about 120 days, after which it is destroyed and replaced.
1. ORIGIN - Where Does It Begin?
Sites of Hematopoiesis (changes with age)
| Stage of Life | Site |
|---|---|
| Embryo (up to ~2 weeks) | Yolk sac (primitive erythropoiesis) |
| Fetus (2-7 months) | Liver, spleen, thymus |
| Late fetus to birth | Bone marrow takes over |
| Adult | Red bone marrow (sternum, vertebrae, ribs, pelvis, proximal long bones) |
In severe anemia or disease, the liver and spleen can restart production - called extramedullary hematopoiesis.
The Starting Cell: Pluripotent Hematopoietic Stem Cell (HSC)
Everything starts from a single type of cell in the bone marrow:
Pluripotent HSC (LT-HSC)
|
v
Short-term HSC (ST-HSC)
|
v
Common Myeloid Progenitor (CMP)
|
v
Megakaryocyte/Erythrocyte Progenitor (MEP)
|
v
Erythroid-committed progenitors (BFU-E → CFU-E)
- LT-HSC = Long-term hematopoietic stem cell: self-renewing, multipotent
- CMP = Common myeloid progenitor: gives rise to red cells, platelets, and white cells (myeloid lineage)
- MEP = Bipotent progenitor for megakaryocytes/erythrocytes
- BFU-E (Burst-Forming Unit - Erythroid): earliest erythroid-committed cell; only 10-20% are actively cycling at any time
- CFU-E (Colony-Forming Unit - Erythroid): more mature; expresses the highest concentration of EPO receptors - this is where erythropoietin exerts its greatest effect
Key point: Without EPO, CFU-E cells rapidly undergo apoptosis (programmed cell death). EPO is literally a survival signal.
2. FORMATION - Stages of RBC Development
Erythropoiesis requires approximately 7 days from progenitor to circulating RBC, involving 3-5 cell divisions.
The Developmental Sequence (in bone marrow):
Proerythroblast
↓
Early Basophilic Erythroblast
↓
Late Basophilic Erythroblast
↓
Polychromatophilic Erythroblast
↓
Orthochromatophilic Erythroblast (Normoblast)
↓
NUCLEUS EJECTED ← [Macrophages phagocytose the nucleus]
↓
Reticulocyte (stays 1-2 days in marrow, then 1-2 days in blood)
↓
Mature Erythrocyte (circulates for ~120 days)
Each Stage Explained Simply:
| Stage | Size | Nucleus | Cytoplasm | What's Happening |
|---|---|---|---|---|
| Proerythroblast | Large (~20 µm) | Large, loose lacy chromatin, nucleoli visible | Deeply basophilic (blue) | First committed RBC precursor; divides actively |
| Basophilic Erythroblast | Slightly smaller | More condensed chromatin | Intensely basophilic | Lots of ribosomes making hemoglobin; mitosis occurs here |
| Polychromatophilic Erythroblast | Smaller | Condensing nucleus | Mixed blue+pink (both ribosomal RNA + Hb present) | Hemoglobin accumulating; last stage with mitosis |
| Orthochromatophilic Erythroblast (Normoblast) | Small | Pyknotic (dark, shrunken) | Acidophilic (pink) - like a mature RBC | Nucleus is about to be expelled |
| Reticulocyte | Similar to RBC | No nucleus | Faint blue network (residual ribosomes - seen with brilliant cresyl blue stain) | Still makes small amount of Hb; enters circulation; ~1% of blood RBCs |
| Mature Erythrocyte | 7-8 µm biconcave disc | Absent | Uniformly pink | Fully functional O2 carrier |
Where do nuclei go? Macrophages (in the bone marrow "erythroblastic island") phagocytose the extruded nucleus. The globin is broken down, iron is recycled, and heme becomes bilirubin.
Microscopic Appearance of Erythroblast Stages
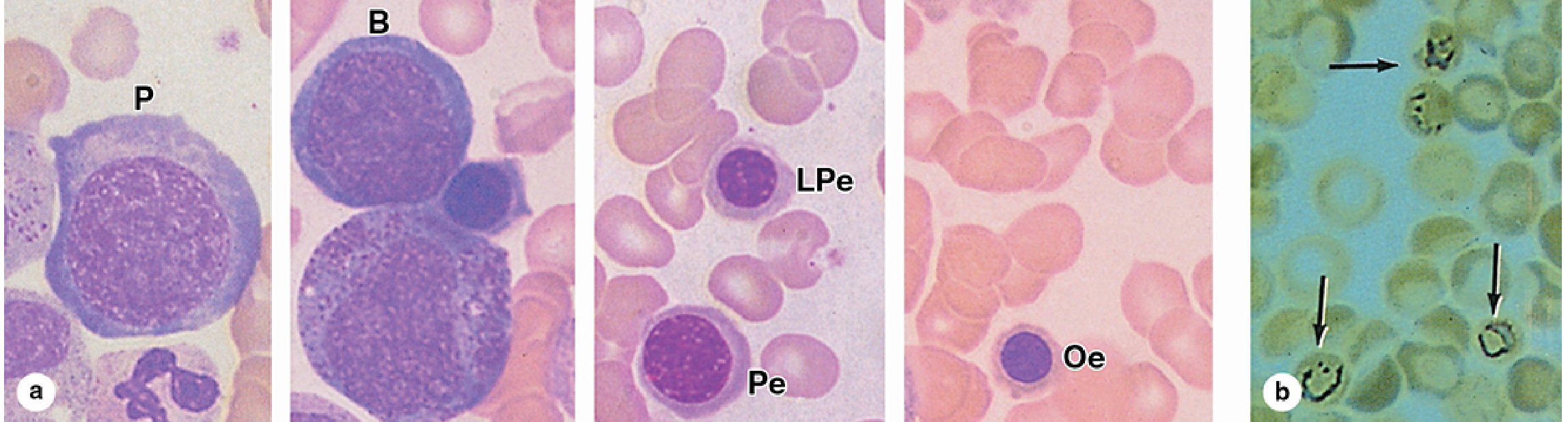
Bone marrow smear showing (a) stages from Proerythroblast (P) through Orthochromatophilic erythroblast (Oe), and (b) reticulocytes identified by brilliant cresyl blue staining - Junqueira's Basic Histology, 17e
3. REGULATION - How Is Erythropoiesis Controlled?
This is the most important part. The body regulates RBC production through a classic negative feedback loop centered on the hormone erythropoietin (EPO).
The Central Feedback Loop
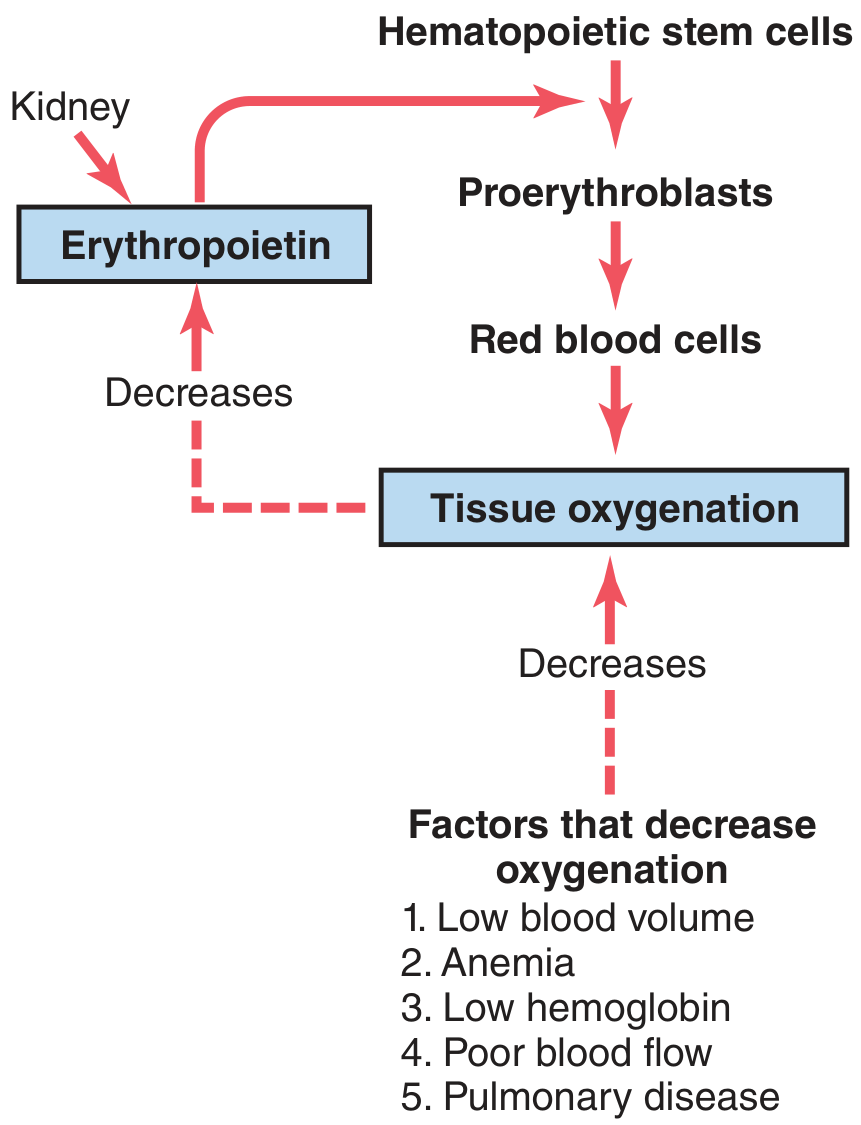
Figure 33.4 from Guyton & Hall Textbook of Medical Physiology - the erythropoietin mechanism
Step-by-Step Regulation Flowchart
DECREASED TISSUE OXYGENATION
(caused by: anemia, hemorrhage, high altitude, cardiac failure, lung disease)
|
↓
KIDNEY senses hypoxia
(90% of EPO from peritubular fibroblast-like cells, cortex/outer medulla)
(10% from liver - insufficient alone)
|
↓
HIF-2α (Hypoxia Inducible Factor-2α) accumulates
(normally degraded by VHL protein in presence of oxygen)
|
↓
HIF-2α + HIF-β + HNF-4 + p300 bind to EPO gene enhancer
|
↓
↑ ERYTHROPOIETIN (EPO) secretion
(Normal: 10-30 IU/L → can rise to 10,000 IU/L in severe anemia)
|
↓
EPO binds to EPO-Receptors on CFU-E and early erythroblasts
|
┌──┴──────────────────────────────────────────┐
↓ ↓
Rescues CFU-E from apoptosis Accelerates maturation of
(↑ survival of progenitors) existing erythroblasts
└──────────────────┬──────────────────────────┘
↓
MORE PROERYTHROBLASTS formed
More rapid transit through erythroblast stages
|
↓ (5-7 days)
↑ RETICULOCYTES in blood
↑ MATURE RBCs
|
↓
IMPROVED TISSUE OXYGENATION
|
↓
↓ EPO secretion (negative feedback complete)
The HIF Mechanism Explained Simply
Think of HIF-2α as an oxygen meter switch:
- Oxygen present → HIF-2α is immediately tagged by the VHL protein and destroyed by the proteasome (like a fuse that burns out fast). No EPO made.
- Oxygen low (hypoxia) → VHL can't work properly → HIF-2α accumulates → enters the nucleus → turns on EPO gene → EPO is made and secreted.
This is why VHL mutations cause polycythemia (too many RBCs) - the HIF-2α never gets degraded, so EPO is always being produced.
4. ESSENTIAL NUTRIENTS for Erythropoiesis
EPO alone is not enough. Several nutrients are absolutely required:
| Nutrient | Role | Deficiency Causes |
|---|---|---|
| Iron (Fe²⁺) | Core of heme in hemoglobin; required for oxygen carrying | Iron-deficiency anemia (microcytic, hypochromic RBCs) |
| Vitamin B12 (Cobalamin) | Required for DNA synthesis (thymidine triphosphate production) | Megaloblastic anemia - large, abnormal RBCs that can't divide properly |
| Folic Acid (Vitamin B9) | Also required for DNA synthesis | Same as B12 deficiency - megaloblastic anemia |
| Vitamin B6 (Pyridoxine) | Heme synthesis (ALA synthase reaction) | Sideroblastic anemia |
| Erythropoietin | Growth/survival factor | Anemia of chronic kidney disease |
| Protein/Amino acids | Globin chain synthesis | General malnutrition anemia |
| Copper | Iron metabolism | Rare copper-deficiency anemia |
5. FATE OF OLD RED BLOOD CELLS (RBC Destruction)
After 120 days, old RBCs become senescent:
Senescent RBC (120 days old)
|
↓
Phagocytosed by macrophages in:
- Spleen (main site)
- Bone marrow
- Liver (Kupffer cells)
|
┌────┴────┐
↓ ↓
Globin Heme
↓ ↓
Amino Fe²⁺ + Protoporphyrin ring
acids | |
↓ ↓ ↓
Reused Recycled Converted to
for new Biliverdin
Hgb ↓
Bilirubin
↓
Bound to albumin → Liver → Conjugated
bilirubin → bile → excreted in feces (stercobilin)
and urine (urobilin)
6. KEY NUMBERS to Remember
| Parameter | Value |
|---|---|
| RBC lifespan | ~120 days |
| RBCs produced per second | 2.5-3 million |
| RBCs replaced per day | ~1% of total (~250 billion) |
| Normal serum EPO | 10-30 IU/L |
| EPO in severe anemia | Up to 10,000 IU/L |
| EPO source | 90% kidney, 10% liver |
| Time from progenitor to circulation | ~7 days |
| Reticulocytes in normal blood | ~1% of RBCs |
| EPO molecular weight | ~34 kDa glycoprotein |
7. SUMMARY FLOWCHART - Complete Overview
BONE MARROW
|
Pluripotent HSC
|
↓ (CMP → MEP)
BFU-E (EPO-independent)
|
↓ (GATA-1 ↑)
CFU-E ←←←← EPO (most important here!)
| ↑
↓ KIDNEY
Proerythroblast ↑ when hypoxia → HIF-2α → EPO gene → EPO
|
↓
Basophilic Erythroblast (Hb synthesis starts; mitosis active)
|
↓
Polychromatophilic Erythroblast (Hb increasing; last mitosis)
|
↓
Orthochromatophilic Erythroblast / Normoblast
|
↓ NUCLEUS EJECTED ← phagocytosed by macrophages
|
Reticulocyte (released into blood; ~1% of RBCs)
|
↓ (1-2 days)
Mature Erythrocyte
|
Circulates 120 days → Destroyed in spleen/liver/marrow
→ Iron recycled, bilirubin excreted
8. CLINICAL RELEVANCE
| Condition | What Breaks Down |
|---|---|
| Chronic Kidney Disease | Kidneys can't make EPO → anemia despite normal marrow. Treated with recombinant EPO (epoetin alfa) |
| Iron Deficiency Anemia | No iron → no heme → microcytic, hypochromic RBCs |
| Megaloblastic Anemia (B12/Folate) | DNA synthesis fails → large abnormal RBCs (macrocytes) that can't divide |
| Polycythemia Vera | JAK2 mutation causes EPO-independent RBC overproduction |
| Aplastic Anemia | HSCs destroyed → no RBC production; very high EPO with no response |
| High altitude adaptation | Chronic hypoxia → sustained EPO → polycythemia (↑ RBC mass) |
Sources:
- Guyton & Hall Textbook of Medical Physiology (Chapter 33)
- Brenner & Rector's The Kidney (Chapter 55 - Normal Erythropoiesis)
- Junqueira's Basic Histology, 17e
- Medical Physiology (Boron & Boulpaep)
- Histology: A Text and Atlas (Ross)
This is a shared conversation. Sign in to Orris to start your own chat.