Defence mechanisms of lung from Murray and fishman full details with condensed structured answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have all the material needed to construct a thorough, condensed, structured answer. Here is the complete response:
Defence Mechanisms of the Lung
Sources: Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume; Fishman's Pulmonary Diseases and Disorders, 2-Volume Set
Overview
The lung is exposed to >10,000 L of ambient air per day across an epithelial surface the size of a doubles tennis court - the largest epithelial surface in the body. Defence is layered: anatomic/structural → physical/mucociliary → biochemical/antimicrobial → cellular innate → adaptive immune. A key challenge is discriminating harmless inhaled particles from pathogens while avoiding destructive inflammation against innocuous antigens.
1. Anatomic and Structural Barriers
| Level | Mechanism |
|---|---|
| Upper airway | Nasal turbulence, vibrissae (nasal hairs), and mucosal folds deposit particles >10 µm |
| Nasopharynx/oropharynx | Mucociliary escalator of nasal epithelium removes trapped particles |
| Larynx/glottis | Cough reflex and glottic closure prevent aspiration |
| Tracheobronchial tree | Cartilaginous segmentation + branching geometry causes impaction of 2-10 µm particles at bifurcations; >10 µm particles never reach the alveoli |
| Alveolus | <1 µm particles reach alveoli and are handled by alveolar macrophages + surfactant |
Air turbulence from the nose and large airways ensures particles >10 µm deposit on mucus-coated surfaces before reaching the lower respiratory tract.
2. Mucociliary Clearance (MCC)
Structure of the Airway Surface Liquid (ASL)
The ASL has two layers:
- Periciliary liquid (PCL): Low-viscosity aqueous layer in which cilia beat freely. Membrane mucin extensions from cilia tips form "grafted brushes" creating electro-repulsion that lubricates ciliary motion.
- Mucus gel layer: Viscoelastic, sits atop the PCL; traps inhaled particles.
Mechanism of Transport
- Ciliated cells are most numerous in trachea and lobar bronchi, decreasing distally.
- Each cilium performs an asymmetric beat: fast forward power stroke propels mucus, slow backward recovery stroke.
- In dense multiciliated zones, coordinated metachronal waves (sequential, not simultaneous) transport mucus proximally from peripheral air spaces toward the mouth.
- Planar cell polarity - developmentally programmed via Wnt signalling - fixes the proximal-to-distal directional axis; surgical reversal of tracheal segments does not reverse cilia beating direction.
Regulation of Ciliary Beat Frequency
- ATP released into extracellular space activates P2Y2 receptors → mucin secretion + increased cilia beat frequency.
- ATP dephosphorylation → adenosine → A2b receptor → sustained hydration and ciliary potentiation.
- Ca²⁺ increases motility; NO increases beat frequency; oxidative stress depresses motility.
- MCC in healthy subjects clears deposited particles within 24 hours.
Impairment
| Cause | Mechanism |
|---|---|
| Primary ciliary dyskinesia | Genetic defect in dynein arms/cilia components → immotile cilia → mucus stasis, bronchiectasis, sinusitis, male infertility |
| Cystic fibrosis | Defective CFTR → reduced Cl⁻ secretion + increased ENaC activity → mucus dehydration, impaired MCC |
| Smoking/influenza | Acquired cilia injury |
| Post-surgical | Cilia damage from intubation/dry gas; endotracheal tube reduces tracheal mucus velocity; anesthetic inhibition; atelectasis |
| Backup: cough | When MCC fails, cough is the primary alternative clearance; if both fail → retained secretions → airway obstruction + amplified inflammation |
3. Cough Reflex
- Serves as backup to MCC; activated by mechanical and chemical stimuli on airway mucosa.
- Generates high expiratory flows that clear retained secretions.
- Compromised by postoperative pain, narcotic analgesics (depress hypercapnic/hypoxic drive, eliminate sighs), and altered lung mechanics.
4. Biochemical and Antimicrobial Defences
Airway Surface Liquid (ASL) Antimicrobials
Maintained at modestly acidic pH (~6.6) which enhances antimicrobial peptide activity.
| Factor | Source | Mechanism |
|---|---|---|
| β-Defensins (hβD-1, -2, -3, -4) | Large airway epithelial cells | Cationic peptides; bind bacteria/virus; form pores in bacterial membranes; suppress pathogen replication; induce cytokine expression. hβD-1 constitutively secreted; others induced by LPS/inflammatory mediators |
| Cathelicidin (LL37/hCAP18) | Airway epithelium | Broad antimicrobial activity; induced by LPS and proinflammatory mediators |
| Lactoferrin | Airway secretory cells, submucosal glands | Iron sequestration (bacteriostatic); direct membrane disruption |
| Lysozyme | Airway epithelium, neutrophils | Cleaves peptidoglycan of bacterial cell walls |
| Bactericidal permeability-increasing protein (BPI) family | Epithelium | Binds lipid A of gram-negative LPS; bactericidal |
Soluble Pattern Recognition Receptors (PRRs)
| Molecule | Class | Action |
|---|---|---|
| Surfactant Protein-A (SP-A) | Collectin | Opsonization; complement activation; phagocytosis promotion; inhibits RSV, adenovirus, influenza A; modulates inflammatory responses |
| Surfactant Protein-D (SP-D) | Collectin | Binds bacterial carbohydrates/lipids; promotes neutrophil-mediated phagocytosis; aggregates pathogens; also suppresses immune activation against harmless particles (tonic suppression) |
| Mannose-binding lectin (MBL) | Collectin | Activates lectin complement pathway against fungi, bacteria, viruses |
| Complement C3/C5 | Complement | Expressed in airway epithelial cells (C3 highest in club cells); opsonizes bacteria; recruits phagocytes; mediates local inflammation. Activated in asthma, CF, obliterative bronchiolitis |
5. Innate Cellular Immunity
A. Airway Epithelial Cells
The airway epithelium is not merely a passive barrier - it is an active immune sentinel:
- Tight junctions provide a physical barrier to pathogen entry.
- Express Toll-like receptors (TLRs) and other PRRs that recognise PAMPs.
- Upon PAMP recognition, secrete CXCL8 (IL-8) → neutrophil recruitment.
- Three basic pathogen clearance responses: (1) direct killing by soluble PRR or interferon production + phagocytosis; (2) epithelial cell effector recruitment (e.g., neutrophils via IL-8); (3) DC activation → adaptive immunity.
B. Dendritic Cells (DCs)
- Network throughout airway epithelium; particularly dense in trachea and large airways.
- Continuously sample airway lumen by extending processes through tight junctions.
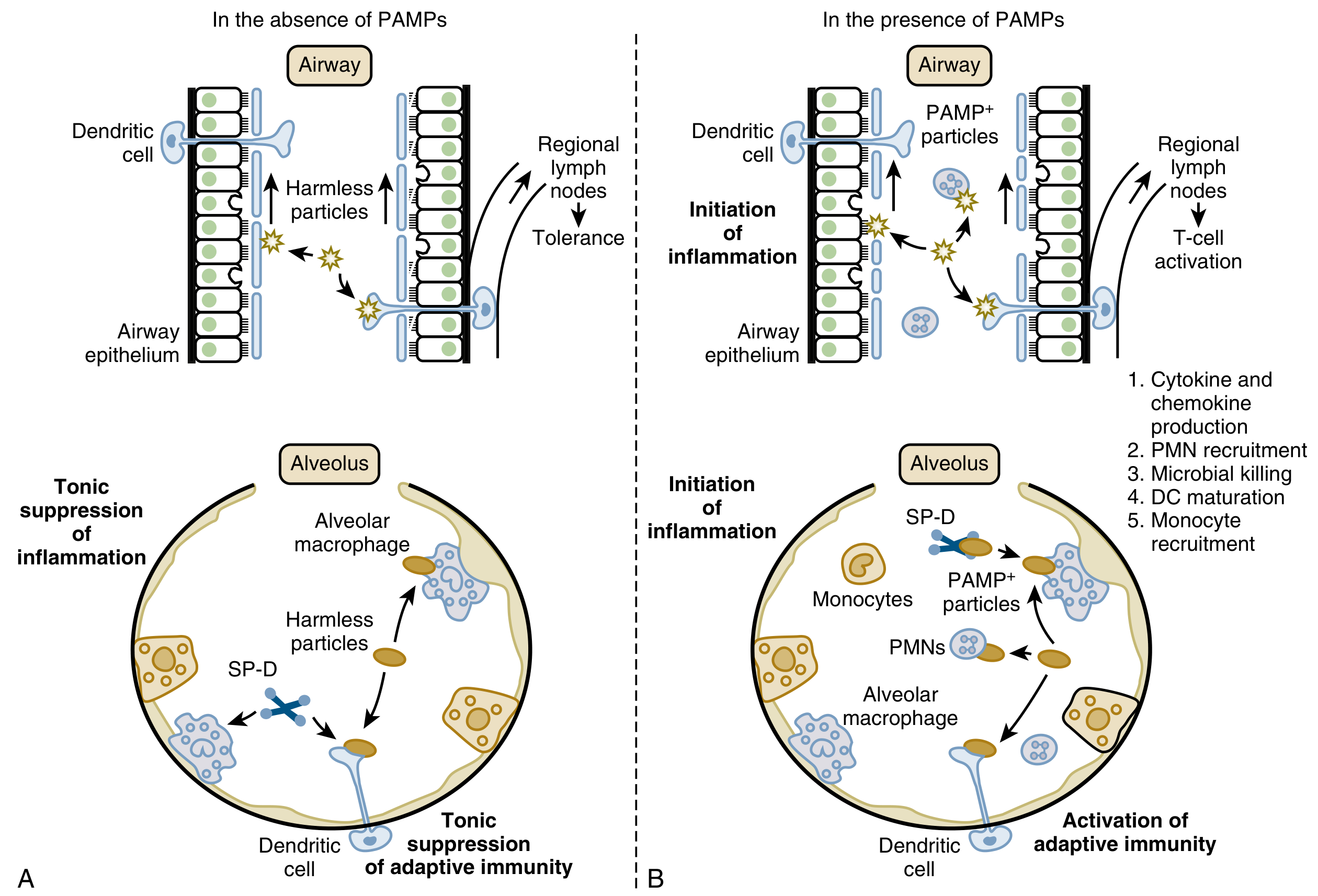
- Without PAMPs: capture antigens → migrate to regional lymph nodes → present antigens to T cells → tolerance (prevents harmful responses to harmless inhaled antigens).
- With PAMPs: undergo maturation → present antigen to T cells → T-cell activation → adaptive immune response.
C. Alveolar Macrophages
- Primary cellular defence of the alveolus for particles <5 µm that reach alveolar surfaces.
- Express TLRs, scavenger receptors (SRs), Fc receptors, complement receptors.
- Functions: phagocytosis, intracellular killing of microbes, antigen presentation, orchestration of inflammatory response.
- In the absence of PAMPs: tonically suppress alveolar inflammation and adaptive immunity (prevent destructive responses to harmless particles).
- In the presence of PAMPs: initiate inflammation: cytokine/chemokine production → recruit PMNs and monocytes → DC maturation → adaptive immunity.
D. Interstitial Macrophages
- Reside in lung interstitium; distinct from alveolar macrophages.
- Participate in local innate sensing and contribute to tissue homeostasis.
E. Neutrophils (PMNs)
- Not resident in healthy lung; rapidly recruited from blood when alveolar macrophages or epithelial cells detect PAMPs.
- Arrive within hours; primary effectors of acute microbial killing.
- Mechanisms: phagocytosis, respiratory burst (reactive oxygen species), degranulation, neutrophil extracellular traps (NETs).
F. Innate Lymphoid Cells (ILCs)
- Resident innate immune cells that provide rapid cytokine responses.
- Bridge innate and adaptive immunity; grouped as ILC1 (IFN-γ), ILC2 (IL-4/IL-5/IL-13), ILC3 (IL-17/IL-22) based on cytokine profile.
- ILC2s are especially important in type 2 airway inflammation (asthma, helminth infection).
G. Monocytes
- Circulating precursors that are recruited to the lung during infection/inflammation.
- Differentiate into macrophages or DCs in the tissue.
6. Recognition System - PAMPs and PRRs
The entire cellular innate response is built on pathogen-associated molecular pattern (PAMP) recognition by pattern recognition receptors (PRRs):
| PRR Class | Location | PAMPs Recognised |
|---|---|---|
| Toll-like receptors (TLRs) | Cell surface + endosomal | LPS (TLR4), peptidoglycan (TLR2), flagellin (TLR5), dsRNA (TLR3), CpG DNA (TLR9) |
| Scavenger receptors (SRs) | Macrophage surface | Oxidised lipids, LPS, bacterial debris |
| Collectins (SP-A, SP-D, MBL) | Secreted into ASL/serum | Oligosaccharides/lipids of bacteria, fungi, viruses |
| Complement | Secreted (classical, lectin, alternative pathways) | Bacterial surfaces, mannose residues |
| NOD-like receptors (NLRs) | Cytoplasmic | Bacterial cell wall components; danger signals |
| RIG-I / MDA5 | Cytoplasmic | Viral RNA |
PAMPs include: complex lipids, carbohydrates, unmethylated CpG DNA sequences, and double-stranded RNAs. Their recognition is the trigger that switches the lung from tonic immune suppression to active defence.
7. Adaptive Immunity
While beyond the innate system, adaptive immunity is primed by the innate arm:
- DCs matured by PAMPs migrate to regional lymph nodes and activate cognate T cells.
- Secretory IgA is the principal antibody in airway secretions; prevents microbial adherence to mucosa.
- B cells/IgG/IgM contribute in lower airways and alveoli.
- CD4+ T helper cells coordinate macrophage activation (Th1) and antibody responses (Th2).
- CD8+ cytotoxic T cells eliminate virally-infected cells.
8. Physiologic Integration - Tonic Suppression vs. Active Defence
A central principle in Murray & Nadel is the discriminative nature of lung immunity:
| State | Airways | Alveolus |
|---|---|---|
| No PAMPs (harmless particles) | DCs capture antigen → lymph node → tolerance | Alveolar macrophages + SP-D tonically suppress inflammation and adaptive immunity |
| PAMPs present (pathogens) | Epithelium initiates inflammation; DCs mature → T-cell activation | Alveolar macrophages activate; recruit PMNs + monocytes; DCs mature → adaptive immunity |
This ensures the lung does not mount harmful inflammatory responses to the tonnes of innocuous dust and pollens inhaled daily, while remaining capable of vigorous defence when true pathogens arrive.
Summary Table: Layered Defence
| Layer | Components | Particles Handled |
|---|---|---|
| Anatomic | Nasal turbulence, vibrissae, airway branching | >10 µm |
| Mucociliary | Mucus gel + ciliary escalator + cough | 2-10 µm; soluble inhaled material |
| Biochemical | β-Defensins, cathelicidin, lactoferrin, lysozyme, BPI, complement, SP-A/D | All sizes; especially at epithelial surface |
| Innate cellular - airways | Epithelial cells (TLRs), DCs | All particles; PAMP discrimination |
| Innate cellular - alveoli | Alveolar macrophages, PMNs, ILCs, interstitial macrophages | <5 µm |
| Adaptive | IgA, IgG, CD4+/CD8+ T cells, B cells | Specific antigens; memory response |
- Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume, Chapter 15 (Innate Immunity), Chapter 4 (Airway Epithelium/MCC), Chapter 13 (Mucociliary Clearance and Disease), Chapter 102 (Perioperative Lung Defence)
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set, Lung Defence Mechanisms section
This is a shared conversation. Sign in to Orris to start your own chat.