Here is the complete, detailed, MUHS exam-oriented answer for 2nd MBBS Pathology covering all your topics, based on Robbins & Kumar Basic Pathology (Harsh Mohan equivalent content).
KIDNEY PATHOLOGY - COMPLETE EXAM NOTES (2nd MBBS / MUHS)
1. RENAL CELL CARCINOMA (RCC)
Introduction
- Most common malignant tumor of the kidney (80-85% of all primary renal malignancies)
- Derived from renal tubular epithelium - located predominantly in cortex
- 2-3% of all adult cancers; ~65,000 cases/year in the USA
- Peak incidence: 6th-7th decade; Males:Females = 2:1
- Risk factors: smoking, hypertension, obesity, cadmium exposure, acquired polycystic disease (30x risk)
Classification (Three Main Types)
| Type | Frequency | Genetics | Gross | Microscopy |
|---|
| Clear Cell | 65% | Loss/inactivation of VHL gene (chr 3p25) | Yellow-orange, variegated | Clear cytoplasm (glycogen + lipid) |
| Papillary RCC | 15% | MET oncogene activation (activating mutations) | Less yellow; bilateral/multiple | Papillary fronds with fibrovascular cores |
| Chromophobe RCC | 5% | Multiple chromosomal losses | Tan-brown | Eosinophilic cytoplasm, perinuclear haloes, prominent cell membranes |
GROSS FEATURES
- Clear cell carcinoma: Large, solitary, well-circumscribed tumor in the cortex; bright yellow-orange due to lipid-laden clear cells; variegated cut surface with areas of hemorrhage, necrosis, and cystic degeneration; frequently invades the renal vein (may extend as a tumor thrombus into the IVC)
- Papillary RCC: Bilateral and multiple; less vibrantly yellow; often shows necrosis, hemorrhage, and cystic degeneration
- Chromophobe RCC: Tan-brown, well-circumscribed
MICROSCOPIC FEATURES
- Clear cell carcinoma: Sheets or nests of large cells with clear cytoplasm (due to dissolved lipid and glycogen in standard processing); abundant delicate vasculature between cell nests; nucleus varies from small/regular to markedly enlarged, hyperchromatic, pleomorphic; variable mitotic figures; cells form abortive tubules or cords
- Papillary RCC: Cuboidal to low columnar cells with eosinophilic to clear cytoplasm lining papillae with fibrovascular cores; foam cells often present within papillary stalks
- Chromophobe RCC: Cells with eosinophilic cytoplasm mixed with pale granular cells; very prominent, distinct cell membranes and perinuclear haloes - classic feature
Clinical Features ("Classic Triad" - seen in only 10%)
- Painless hematuria (most frequent; >50% of cases - intermittent, macroscopic)
- Palpable abdominal/flank mass
- Dull flank pain
Paraneoplastic syndromes (important for exam):
- Polycythemia (5-10%) - erythropoietin secretion
- Hypercalcemia (PTHrP)
- Hypertension (renin secretion)
- Cushing syndrome (ACTH)
- Feminization/masculinization
Metastases: Lungs ("cannonball"), bones; "metastasis from unknown primary" presentations are common.
2. CLASSIFICATION OF GLOMERULAR DISEASES
Normal Glomerulus (Quick Recap)
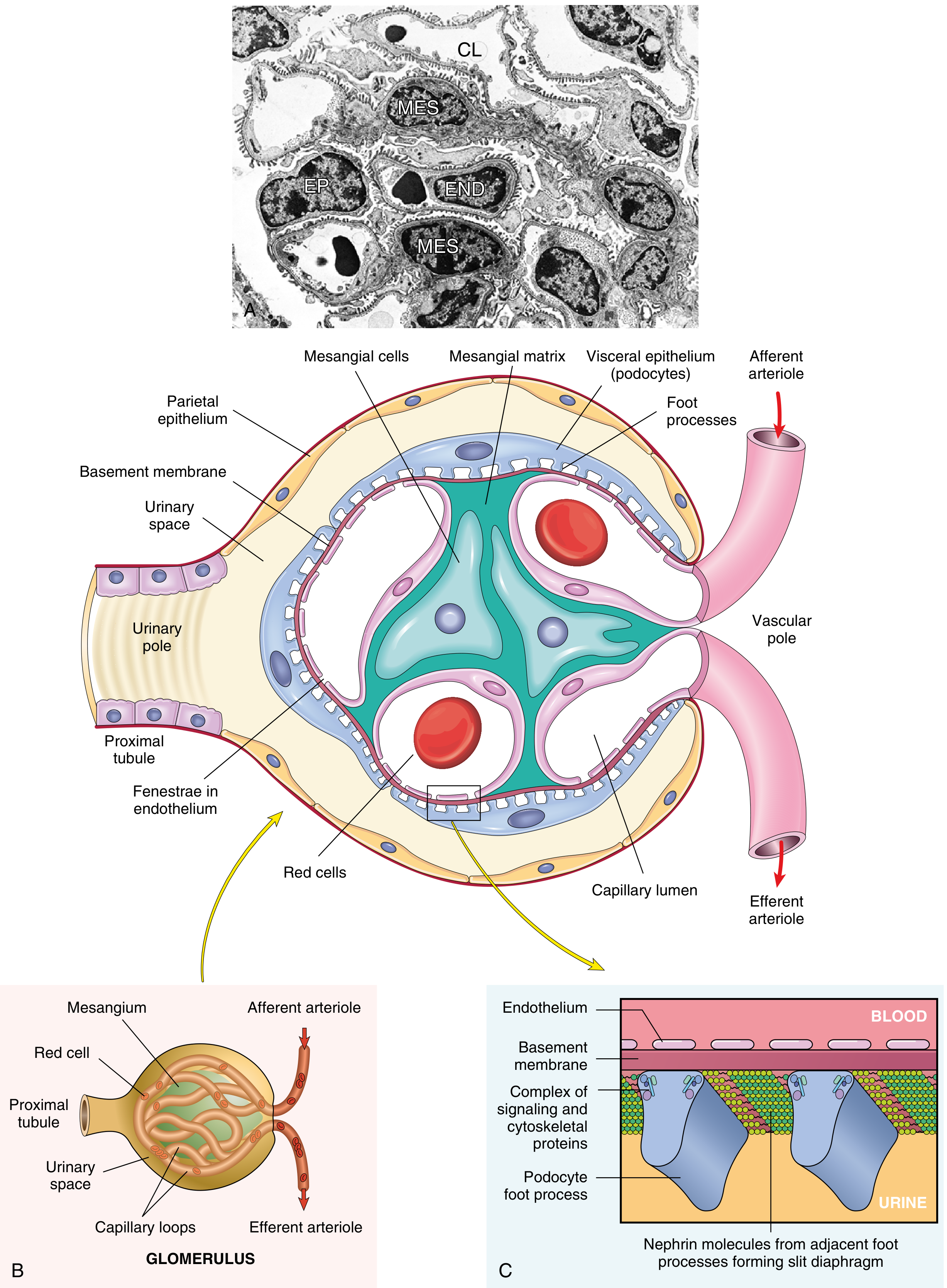
Fig. 12.1 - Normal glomerulus showing CL (capillary lumen), END (endothelium), EP (epithelial cell/podocyte), MES (mesangium), foot processes, slit diaphragm (Nephrin/Podocin), and GBM.
Mechanisms of Glomerular Injury
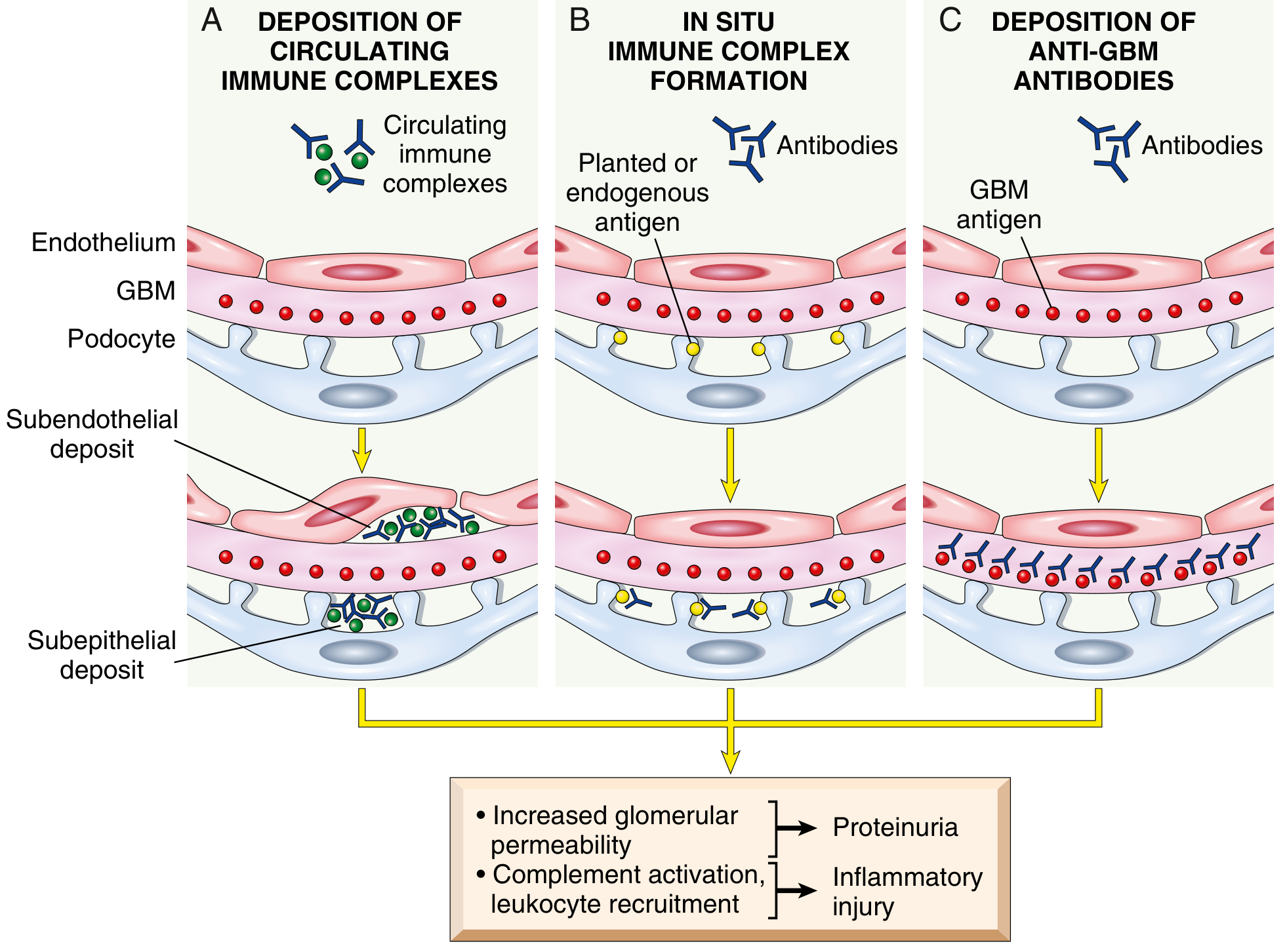
Fig. 12.2 - Three mechanisms: (A) Deposition of circulating immune complexes → granular IF pattern; (B) In situ immune complex formation → granular IF pattern; (C) Anti-GBM antibodies → linear IF pattern. All lead to increased glomerular permeability and inflammatory injury.
Classification of Glomerular Diseases
A. By Clinical Syndrome:
I. Nephrotic Syndrome (Proteinuria >3.5 g/day)
| Disease | Light Microscopy | IF | EM |
|---|
| Minimal Change Disease | Normal | Negative | Effacement of foot processes only |
| Focal Segmental Glomerulosclerosis | Focal, segmental sclerosis + hyalinosis | Usually negative (IgM, C3 in scars) | Effacement of foot processes; epithelial denudation |
| Membranous Nephropathy | Diffuse capillary wall thickening, "spikes" | Granular IgG + C3 along GBM | Subepithelial deposits |
| MPGN Type I | Mesangial proliferation, double contour ("tram-track") | Granular IgG + C3 | Subendothelial deposits |
II. Nephritic Syndrome (Hematuria, Hypertension, Oliguria, Azotemia)
| Disease | IF | Key Feature |
|---|
| Acute Poststreptococcal GN | Granular IgG + C3 | Subepithelial "humps" on EM |
| RPGN (Crescentic GN) | Linear (anti-GBM) / Granular / Negative | Crescents in Bowman's space |
| IgA Nephropathy | Mesangial IgA | Recurrent hematuria |
| Lupus Nephritis | Full house (IgG, IgA, IgM, C3, C4, C1q) | Wire-loop lesions |
B. By Immunopathology (important for RPGN classification - see below)
Morphology of Membranous Glomerulopathy (Membranous Nephropathy)
Definition: Glomerular disease characterized by subepithelial deposits of antigen-antibody complexes along the GBM, causing the nephrotic syndrome. Most common cause of nephrotic syndrome in adults (30-60 years).
Etiology:
- Primary (80%): Autoantibodies against podocyte antigen Phospholipase A2 Receptor (PLA2R) - present in 70-80% of primary cases
- Secondary (20%):
- Infections: chronic Hepatitis B, syphilis, schistosomiasis, malaria
- Malignancies: carcinomas, B-cell tumors (CLL)
- Autoimmune: SLE
- Drugs: penicillamine, captopril, NSAIDs
- Heavy metals: gold, mercury
Pathogenesis: In-situ immune complex formation - anti-PLA2R antibodies bind to podocyte antigen → subepithelial immune complex deposition → complement activation (sublytic MAC) → podocyte injury → proteinuria. Unlike subendothelial deposits, subepithelial deposits cause little inflammation (less access to complement/leukocytes from blood).
Morphology:
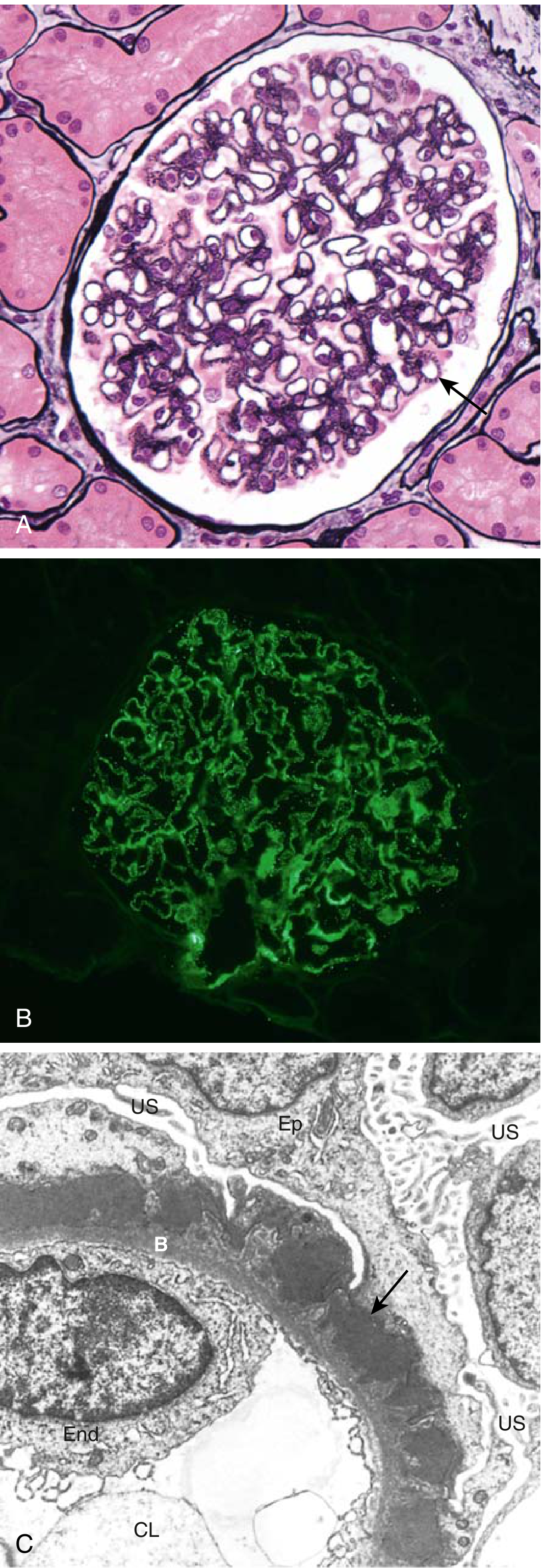
Fig. 12.6 - Membranous nephropathy: (A) Diffuse thickening of GBM without cellular proliferation or inflammation (silver stain highlights GBM spikes). (B) Granular deposits of IgG by immunofluorescence along the GBM. (C) Subepithelial deposits (arrow), effacement of foot processes.
- Light Microscopy: Diffuse thickening of glomerular capillary walls without endothelial/mesangial proliferation or leukocytic infiltration; silver stain shows characteristic "spike and dome" pattern - spikes of GBM material projecting between subepithelial deposits (best seen on Jones methenamine silver stain)
- Immunofluorescence: Granular deposits of IgG and C3 along the entire GBM ("continuous granular")
- Electron Microscopy: Subepithelial electron-dense deposits ("humps"); effacement of podocyte foot processes; GBM projects around the deposits as "spikes"
Clinical Course:
- Nephrotic syndrome (massive proteinuria, hypoalbuminemia, edema, hyperlipidemia)
- Slow, indolent course
- "Rule of thirds": 1/3 spontaneous remission, 1/3 persistent proteinuria but stable renal function, 1/3 progressive renal failure over 10-20 years
- Increased risk of renal vein thrombosis (loss of antithrombin III in urine)
- Treatment: Immunosuppression (steroids + cyclophosphamide or calcineurin inhibitors); monitor PLA2R antibody levels
3. CHRONIC PYELONEPHRITIS
Definition: Clinicopathologic entity in which interstitial inflammation is associated with grossly visible scarring of the kidneys and deformity of the pelvicalyceal system in patients with a history of UTI. It is a known cause of chronic kidney disease.
Pathogenesis:
- Reflux nephropathy (most common) - due to vesicoureteric reflux (VUR); recurrent infections lead to repeated renal inflammation and scarring
- Obstructive pyelonephritis - due to calculi, posterior urethral valves, unilateral obstructive ureteral lesions; obstruction can be unilateral or bilateral
GROSS APPEARANCES
- Hallmark: Coarse, discrete, irregular corticomedullary scars (not fine or symmetric)
- Overlying dilated, blunted, or deformed calyces and flattening of the papillae
- One or both kidneys may be involved
- When bilateral, scarring is asymmetric (distinguishes from chronic GN which gives fine, symmetrical scarring)
- Kidneys are asymmetrically contracted on imaging
DIAGRAM: Cross-section of kidney in Chronic Pyelonephritis
_____________________________________________
| SCAR (coarse, irregular) |
| ↕ ↕ ↕ ↕ |
| Cortex [thinned over scarred calyx] |
| _________ ___________ _________ |
| | Normal | | Dilated | | Scarred | |
| | Calyx | | Blunted | | Area | |
|_|_________|_|_Calyx_____|_|_________|_____|
← Asymmetric involvement characteristic →
MICROSCOPIC APPEARANCES
- Patchy interstitial fibrosis with infiltrate of lymphocytes, plasma cells, and occasionally neutrophils
- Tubular atrophy alternating with tubular dilation
- Dilated tubules contain PAS-positive, pink-to-blue glassy casts - "colloid casts" or "thyroidization" (tubules resemble thyroid follicles - pathognomonic)
- Glomeruli: normal or show variable periglomerular fibrosis and sclerosis
- Blood vessels: arteriolar sclerosis (due to hypertension)
Clinical Features:
- Gradual onset of renal insufficiency; sometimes detected incidentally
- Hypertension (common)
- Bilateral progressive disease: tubular dysfunction → inability to concentrate urine → hyposthenuria, polyuria, nocturia
- Radiologic: asymmetrically contracted kidneys with calyceal blunting/deformity
- Some progress to secondary glomerulosclerosis with proteinuria
4. RAPIDLY PROGRESSIVE GLOMERULONEPHRITIS (RPGN)
Definition
Clinical syndrome characterized by:
- Acute renal failure (renal function deteriorates over days to weeks)
- Features of nephritic syndrome (hematuria, hypertension, oliguria)
- Often severe oliguria progressing to anuria
- Histologic counterpart = Crescentic GN
Classification (Three Types) - Most Important for Exam
| Type | Mechanism | IF Pattern | Serologic Marker | Example |
|---|
| Type I (Anti-GBM) | Anti-GBM antibodies | Linear IgG + C3 | Anti-GBM Ab (Goodpasture) | Goodpasture disease/syndrome |
| Type II (Immune Complex) | IC deposition | Granular IgG + C3 | Low complement (C3) | Post-streptococcal GN, SLE, IgA nephropathy |
| Type III (Pauci-immune) | ANCA-mediated | Negative (pauci-immune) | ANCA (PR3-ANCA or MPO-ANCA) | Wegener's (GPA), MPA, Churg-Strauss |
Memory Aid: "LGN" = Linear (Type I), Granular (Type II), Negative (Type III)
Key Note on Goodpasture Syndrome (Type I): Anti-GBM antibodies also cross-react with pulmonary alveolar capillary BM → pulmonary hemorrhage + renal failure = Goodpasture syndrome. Antibodies directed against type IV collagen alpha-3 chain.
Pathogenesis of Crescent Formation
CRESCENT FORMATION DIAGRAM:
Severe glomerular injury
↓
Breaks in GBM → fibrin leaks into Bowman's space
↓
Fibrin acts as scaffold
↓
Proliferation of PARIETAL epithelial cells
+
Migration of MONOCYTES/MACROPHAGES into Bowman's space
↓
CRESCENT formation (fills Bowman's space)
↓
Compresses glomerular tuft → obliterates blood flow
↓
Progressive glomerulosclerosis → ESRD
MORPHOLOGY (RPGN / Crescentic GN)
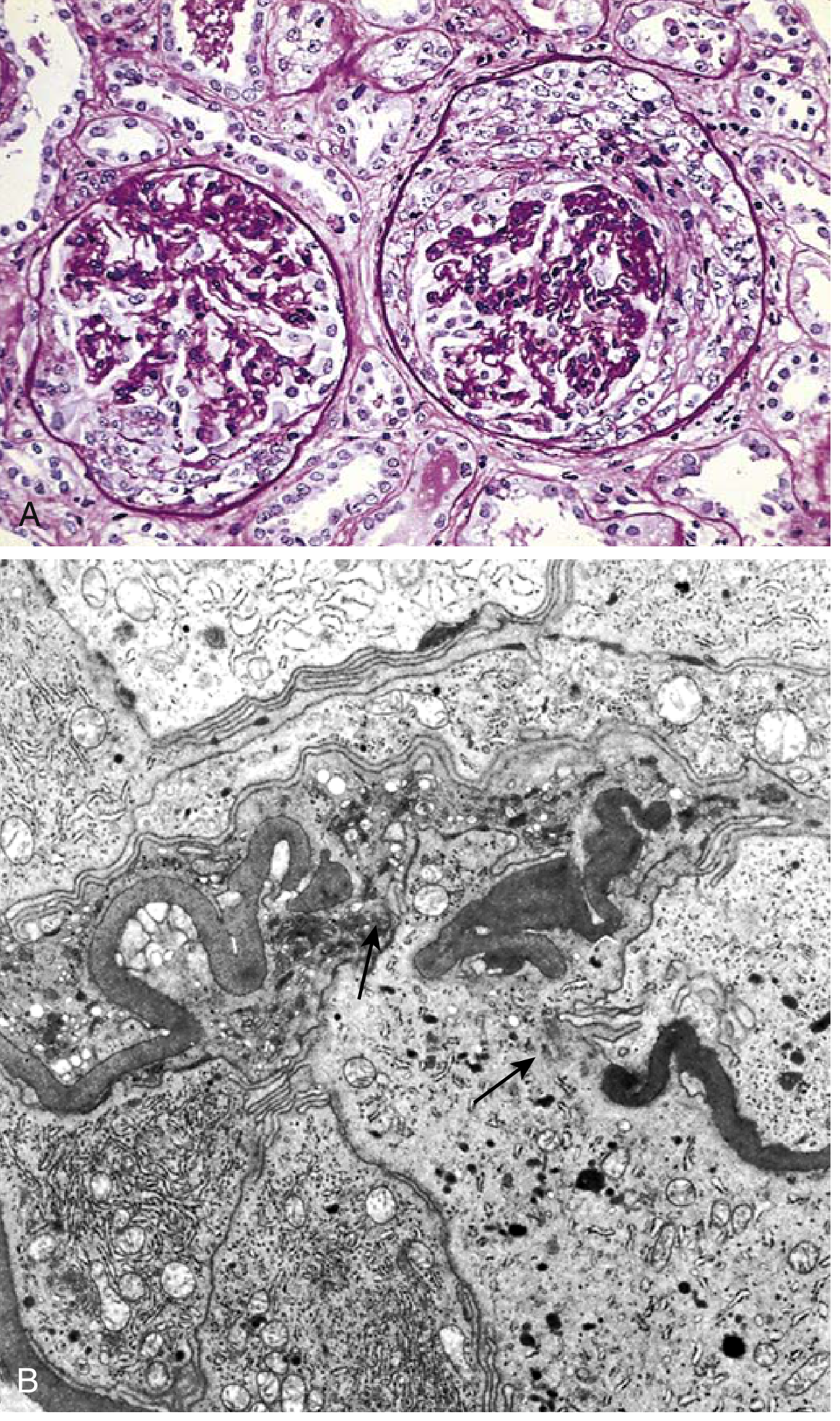
Fig. 12.10 - Crescentic GN: (A) Compressed glomerular tufts with crescent-shaped mass of proliferating epithelial cells and leukocytes within Bowman's capsule (PAS stain). (B) EM showing wrinkled GBM with focal disruptions (arrows) - sign of severe injury.
Gross: Kidneys are enlarged and pale, often with petechial hemorrhages on the cortical surface.
Microscopy:
- Hallmark: Crescents - crescent-shaped accumulations of cells filling Bowman's space
- Crescents composed of: parietal epithelial cells + monocytes/macrophages + fibrin
- The glomerular tuft is compressed
- Segmental necrosis of capillary loops (fibrinoid necrosis)
- Breaks/disruptions in GBM
- In immune complex types: additional endocapillary proliferation and leukocyte infiltration within the tuft
IF:
- Type I: Linear IgG + C3
- Type II: Granular IgG + C3
- Type III: Negative (pauci-immune)
EM: Wrinkling and disruptions of GBM; electron-dense immune complex deposits in Type II
Clinical Course:
- Onset resembles nephritic syndrome but oliguria and azotemia are more pronounced
- Proteinuria may approach nephrotic range
- If untreated: renal failure within weeks to months; some become anuric
- Prognosis: Correlated to % glomeruli with crescents - <80% crescents = better prognosis
- Treatment: Immunosuppressive agents (high-dose steroids + cyclophosphamide); plasmapheresis for Type I (anti-GBM) and Type III (ANCA-associated)
5. NEPHROTIC SYNDROME
Definition
Characterized by massive proteinuria (>3.5 g/24h in adults) due to primary glomerular damage.
Classic Tetrad of Features
┌─────────────────────────────────────────────────────────┐
│ NEPHROTIC SYNDROME │
│ │
│ 1. MASSIVE PROTEINURIA (>3.5 g/24h) │
│ ↓ (loss of serum proteins) │
│ 2. HYPOALBUMINEMIA │
│ ↓ (reduced oncotic pressure) │
│ 3. GENERALIZED EDEMA (Anasarca) │
│ ↓ (secondary hyperaldosteronism) │
│ 4. HYPERLIPIDEMIA + LIPIDURIA │
│ (compensatory liver synthesis; lipoprotein lipase │
│ lost in urine) │
└─────────────────────────────────────────────────────────┘
Additional Features
- Lipiduria: Oval fat bodies (tubular cells + free lipid) seen on urinalysis; Maltese cross pattern under polarized light
- Increased thrombotic tendency: Loss of antithrombin III, Protein C and S in urine → deep vein thrombosis, renal vein thrombosis (especially in membranous nephropathy)
- Increased susceptibility to infections: Loss of immunoglobulins (IgG) in urine → encapsulated organisms (Pneumococcal peritonitis in children)
- Lipoid nephrosis = old term for minimal change disease
Causes by Age
| Age Group | Most Common Cause |
|---|
| Children (1-8 years) | Minimal Change Disease (lipoid nephrosis) |
| Adults (>40 years) | Membranous Nephropathy |
| All ages | FSGS (secondary most common overall) |
| Diabetics | Diabetic nephropathy |
| SLE patients | Lupus nephritis (diffuse proliferative - Class IV) |
Pathophysiology of Edema
- Proteinuria → hypoalbuminemia → ↓oncotic pressure → fluid shifts to interstitium
- ↓ circulating volume → RAAS activation → sodium and water retention → generalized edema
- Edema is typically pitting and most pronounced in areas of low tissue tension (periorbital in children, ankle in adults)
6. POST-STREPTOCOCCAL GLOMERULONEPHRITIS (PSGN)
Definition
Acute proliferative (nephritic) glomerulonephritis following infection by nephritogenic strains of Group A β-hemolytic Streptococcus (Streptococcus pyogenes).
Etiology
- Causative organism: Group A β-hemolytic Streptococcus (Streptococcus pyogenes) - specific nephritogenic strains
- Nephritogenic antigens:
- Streptococcal Exotoxin B (SpeB) - highly immunogenic, detected in GBM deposits
- Streptokinase (plasminogen-related)
- Neuraminidase
- Common following:
- Pharyngeal infection (throat): latent period 1-3 weeks
- Skin infection (impetigo): latent period 3-6 weeks
- Other postinfectious GN: Pneumococcus, Staphylococcus, mumps, measles, hepatitis B/C
Etiopathogenesis
Group A β-hemolytic Streptococcus (nephritogenic strains)
↓
Infection: Pharyngitis or Pyoderma/Impetigo
↓ (1-4 weeks latent period)
Formation of STREPTOCOCCAL ANTIGENS (e.g., Exotoxin B)
↓
Two mechanisms operate:
(A) Preformed circulating immune complexes deposit in GBM
+
(B) In situ complex formation - Ag deposits in GBM, then Ab binds
↓
GRANULAR immune complex deposits (IgG + C3) in GBM
↓
CLASSICAL COMPLEMENT PATHWAY ACTIVATION
↓
Chemotaxis of neutrophils + monocytes
↓
Release of proteases, reactive oxygen species
↓
GBM damage → HEMATURIA
Endothelial/mesangial proliferation → ↓GFR → OLIGURIA, AZOTEMIA
Sodium + water retention → HYPERTENSION, EDEMA
↓
ACUTE NEPHRITIC SYNDROME
GROSS FEATURES
- Kidneys are bilaterally enlarged and swollen
- Pale cortical surface with petechial hemorrhages (flea-bitten appearance)
- Pale gray cut surface - due to diffuse glomerular involvement
- Congestion and hemorrhage visible
GROSS DIAGRAM:
_____________________
/ KIDNEY \
| ● ● ● ● ● ● ● | ← Petechial hemorrhages
| ● ● ● ● | ("flea-bitten" appearance)
| enlarged, pale |
| (bilateral) |
\______________________ /
MICROSCOPIC FEATURES
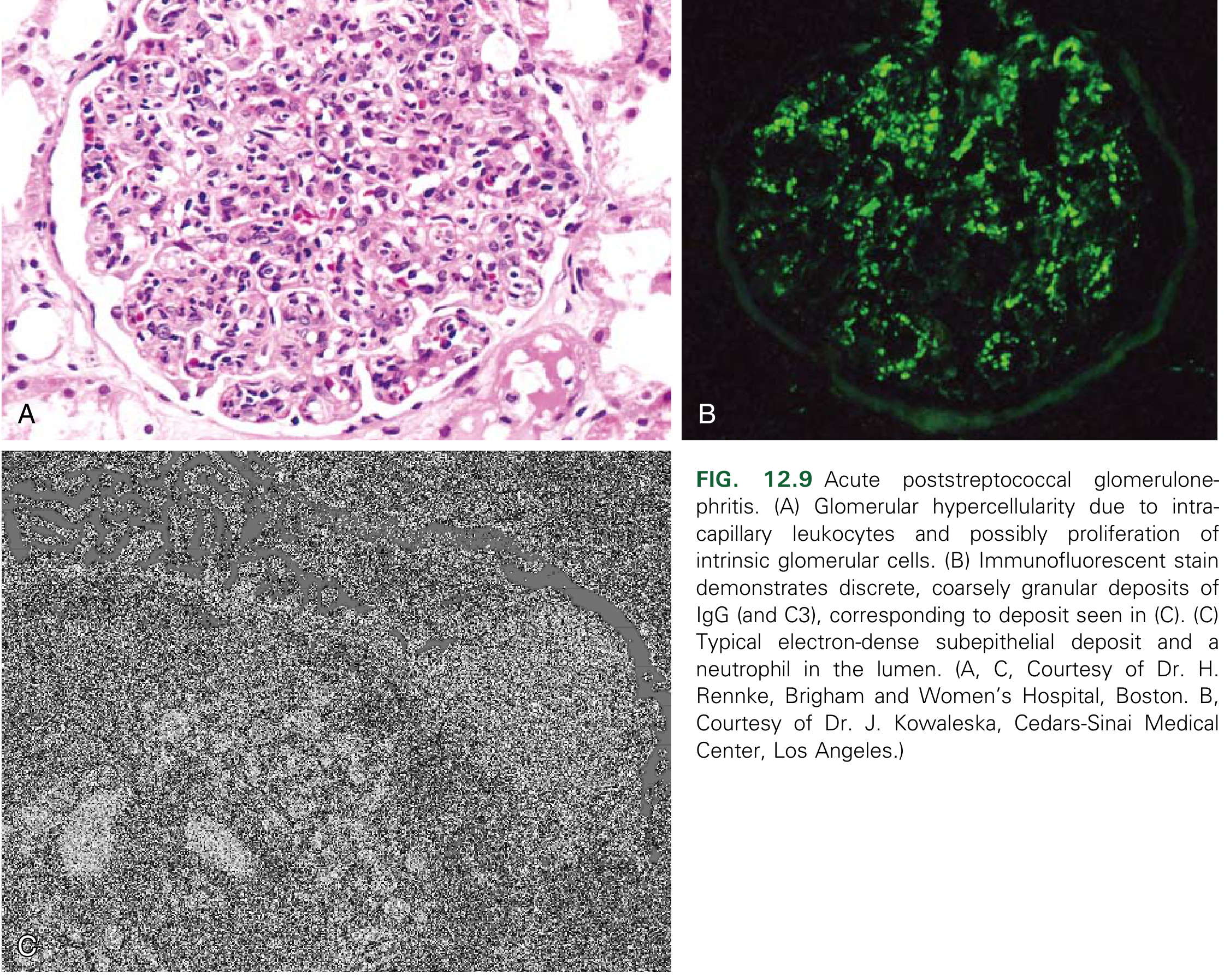
Fig. 12.9 - Acute PSGN: (A) Diffuse glomerular hypercellularity - H&E. (B) Coarsely granular ("lumpy-bumpy") IgG and C3 deposits - immunofluorescence. (C) Subepithelial electron-dense "humps" and neutrophil in capillary lumen - EM.
Light Microscopy (H&E):
- Diffuse (all glomeruli involved) glomerulonephritis
- Increased cellularity of glomerular tufts - the hallmark
- Proliferation of endothelial cells and mesangial cells
- Infiltration by neutrophils and monocytes (intracapillary)
- Glomeruli appear hypercellular, enlarged, bloodless
- Occasional capillary wall necrosis
- In severe cases: crescents (RPGN superimposed)
Immunofluorescence:
- Granular (lumpy-bumpy) deposits of IgG and C3 in the capillary walls and mesangium
- Complement is activated by the classical pathway → C3 levels reduced in serum
Electron Microscopy (most characteristic feature):
- Subepithelial electron-dense deposits ("humps") - pathognomonic
- These are located on the epithelial side of GBM (between podocytes and GBM)
- Also: subendothelial and mesangial deposits may be seen
- Deposits cleared within 2 months after resolution of infection
Summary Table - PSGN on Biopsy:
| Modality | Finding |
|---|
| Light Microscopy | Diffuse endocapillary proliferative GN; hypercellularity |
| Immunofluorescence | Granular IgG + C3 ("lumpy-bumpy") |
| Electron Microscopy | Subepithelial "humps" (pathognomonic) |
Clinical Course
Presentation (typically 1-4 weeks after streptococcal infection in children):
- Acute nephritic syndrome: sudden onset hematuria (cola/smoky/tea-colored urine), oliguria, hypertension, periorbital edema, mild to moderate azotemia
- Proteinuria (usually <3.5 g/day; occasionally nephrotic range)
Lab findings:
- ↑ ASO (Antistreptolysin O) titer - rises after pharyngitis
- ↑ Anti-DNase B - rises after skin infection (ASO may be normal in pyoderma)
- ↓ Serum C3 (complement consumed via classical pathway) during active disease
- Urinalysis: RBC casts (pathognomonic of GN), proteinuria, granular casts
- ↑ Blood urea, creatinine
Prognosis:
- Children: Excellent - >95% recover completely; C3 normalizes in 6-8 weeks
- Adults: More guarded - 15-50% develop chronic renal disease over years to decades
- Poor prognostic indicators: crescents in >80% of glomeruli, persistent proteinuria, hypertension, elderly age
- Small percentage develop RPGN (crescentic GN) - requires aggressive treatment
QUICK COMPARISON: NEPHROTIC vs. NEPHRITIC SYNDROME
| Feature | Nephrotic | Nephritic |
|---|
| Proteinuria | Massive (>3.5 g/day) | Mild to moderate (<3.5 g/day) |
| Hematuria | Absent or mild | Hallmark (RBC casts) |
| Edema | Marked (anasarca) | Mild (periorbital) |
| Hypertension | Absent or mild | Prominent |
| Oliguria | Absent | Present |
| Azotemia | Absent | Present |
| Hypoalbuminemia | Marked | Mild |
| Hyperlipidemia | Present | Absent |
GLOMERULAR SYNDROMES - ENUMERATION
- Nephrotic Syndrome - Minimal Change Disease, FSGS, Membranous Nephropathy, MPGN
- Nephritic Syndrome - Post-infective GN, RPGN, IgA Nephropathy, Lupus Nephritis
- Rapidly Progressive (Crescentic) GN - Type I (anti-GBM), Type II (IC), Type III (Pauci-immune)
- Asymptomatic hematuria/proteinuria - IgA nephropathy, thin basement membrane disease
- Chronic renal failure - End-stage of any progressive GN
ACUTE PROLIFERATIVE GN (SAME AS PSGN - see Section 6 above)
Additional points on Etiopathogenesis for exam:
- The term "proliferative" refers to endocapillary (inside the capillary loop) proliferation
- "Diffuse" = >50% of glomeruli involved
- Immunological basis: Type III hypersensitivity (immune complex mediated)
- Complement pathway: Classical (IC activates C1q → C3 consumption → low serum C3)
- Exotoxin B acts as a "planted antigen" in the GBM → in situ IC formation adds to circulating IC deposition
Prognosis Key points (for MCQs):
- Children: >95% complete recovery
- The fact that most are caused by specific nephritogenic M-types of Strep means not all Strep infections cause GN
- The incidence has declined in high-income countries due to antibiotic use
Source: Robbins & Kumar Basic Pathology (equivalent to Harsh Mohan Textbook of Pathology - content aligned with 2nd MBBS MUHS syllabus)