desmoid tumor
Reading File
Finding Sources
Searching PubMed
desmoid tumor treatment
Searching the Web
desmoid tumor 2024 2025 treatment guidelines sorafenib nirogacestat
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Here is the full review:
Desmoid Tumor (Aggressive Fibromatosis / Desmoid-Type Fibromatosis)
Definition and Overview
Desmoid tumors - also called desmoid fibromatosis or aggressive fibromatosis - are rare, locally invasive fibroblastic tumors arising from musculoaponeurotic structures. They are classified as benign (no metastatic potential) but are biologically treacherous due to their propensity for local invasion, infiltration beyond apparent margins, and high recurrence rates.
- Incidence: 2-5 cases per million per year
- Median age at diagnosis: 35 years (range 16-79)
- Female predominance (2-3x more common in women)
- Peak incidence: 3rd-4th decade
Pathogenesis and Molecular Biology
The molecular driver is dysregulation of the WNT/beta-catenin signaling pathway:
| Setting | Molecular Defect | Result |
|---|---|---|
| Sporadic (75-85%) | Somatic CTNNB1 mutation | Stabilized beta-catenin accumulates in nucleus |
| FAP-associated (15-25%) | Germline APC mutation | Same end result - loss of beta-catenin degradation |
Between 80-95% of desmoid tumors harbor CTNNB1 or APC mutations, leading to nuclear accumulation of beta-catenin, which activates transcription factors promoting proliferation. Tumors also highly express NOTCH1 and HES1, which is the target of nirogacestat (gamma-secretase inhibitor).
There is also increased estrogen receptor-beta expression in ~80% of specimens, providing rationale for anti-estrogen therapy.
-
-
- Robbins Pathologic Basis of Disease, p. 1991; Sabiston Textbook of Surgery, p. 1302
-
Anatomic Classification
Three major anatomic groups:
- Abdominal wall - classic presentation; young postpartum women; most common
- Extraabdominal - shoulder girdle, arm, thigh, neck, pelvis, forearm, popliteal fossa
- Intraabdominal / Mesenteric - worst prognosis; may invade bowel, cause obstruction, ischemia, fistulae
FAP-associated desmoids typically occur in surgical incisions, abdominal wall, or small bowel mesentery. APC mutations at the 3' end of the gene confer the highest desmoid risk.
Histopathology
Gross: Gray-white, firm, poorly demarcated masses up to 15 cm. Rubbery and tough. Appear to have a pseudocapsule but microscopically extend beyond it with radial fibrous septae.
Microscopic: Bland fibroblasts (uniform elongated spindle cells) arranged in long parallel fascicles amid abundant dense collagen. Low cellularity. Histologically resembles a scar. No pleomorphism. No mitoses.
MRI appearance: Hypointense on both T1 and T2 (reflecting dense collagen/fibrous content) - an important distinguishing feature.
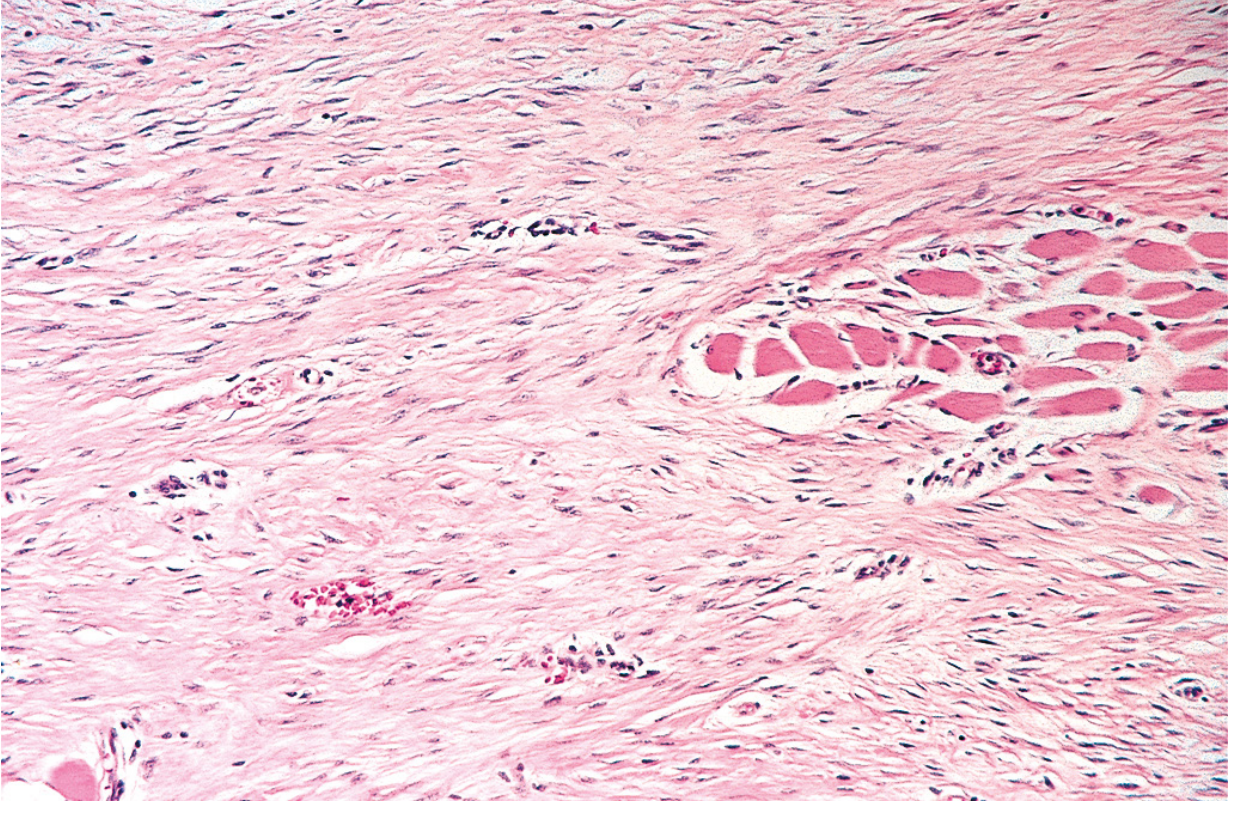
Fig: Deep fibromatosis infiltrating skeletal muscle. Note bland spindle cells in dense collagenous stroma infiltrating skeletal muscle bundles (top right).
- Robbins Pathologic Basis of Disease, Fig. 26.44
IHC: ~70-75% of cell nuclei stain positive for beta-catenin (nuclear) - diagnostically useful.
Clinical Features
- Usually presents as a firm, painless (or minimally painful) mass > 5 cm with indolent growth
- Can cause pain, functional limitation, or neurovascular compromise depending on location
- Intraabdominal: bowel obstruction, hemorrhage, ischemia, perforation, ureteral obstruction
- Cervical/thoracic outlet desmoids can be life-threatening
Natural history is highly variable and unpredictable:
- ~10% grow rapidly
- ~10% undergo spontaneous regression
- ~20-30% regress spontaneously
- ~30% alternate between growth and regression
- ~50% remain stable or grow very slowly
This unpredictable biology is why treatment decisions are complex.
Diagnosis
- CT / MRI for staging and local extent - cross-sectional imaging is useful but not diagnostic
- Core-needle biopsy required to confirm diagnosis and exclude other soft tissue sarcoma subtypes
- Family history and screening colonoscopy should be obtained in all patients with desmoid tumors to rule out FAP/Gardner syndrome
- Mutations in CTNNB1 correlate with local recurrence risk
Association with FAP / Gardner Syndrome
- 15-30% of FAP patients develop desmoids
- Desmoids are the 2nd leading cause of death in FAP (after colorectal cancer)
- Develop typically 2-3 years after surgery, around age 30
- FAP-associated desmoids are more likely to recur than sporadic or pregnancy-associated tumors
- Risk factors in FAP: mutations at 3' end of APC gene, female sex, extraintestinal manifestations, family history of desmoid disease
Treatment
Paradigm Shift: Active Surveillance First
Surgery was once the standard of care but is no longer first-line. The modern approach:
Active surveillance (watchful waiting) as initial management for most asymptomatic or stable tumors, with systemic or local treatment reserved for progressive or symptomatic disease.
This shift is justified by:
- High surgical recurrence rates (20-50%)
- Spontaneous regression in 20-30% of cases
- Morbidity of wide resection, especially for mesenteric/intraabdominal tumors
Treatment Ladder
| Approach | Role | Notes |
|---|---|---|
| Active surveillance | First-line for most | Preferred at experienced centers |
| NSAIDs (sulindac, celecoxib) | Systemic - early line | Used with/without tamoxifen |
| Anti-estrogens (tamoxifen, toremifene, raloxifene) | Systemic - early line | Tamoxifen + sulindac combination effective |
| Sorafenib (TKI) | Systemic - progressive/refractory | Phase III RCT proven; prolongs PFS |
| Pazopanib (TKI) | Systemic | Active for progressive disease |
| Cytotoxic chemo | Systemic - aggressive disease | Vinblastine/methotrexate, doxorubicin/dacarbazine, navelbine, liposomal doxorubicin |
| Nirogacestat (gamma-secretase inhibitor) | Targeted - progressive | Phase III RCT; FDA-approved (2023), EC-approved (2025) |
| Radiotherapy | Local control | Improves local control with surgery; risk of bowel necrosis/fistula intraabdominally |
| Cryoablation | Local - small/moderate extraabdominal | Effective in retrospective series |
| Surgery | Reserved, rarely needed | Only when other options exhausted; wide negative margins; 1-cm margin recommended for extraabdominal |
Key Drug Highlights
Sorafenib: A multi-kinase inhibitor proven in a phase III RCT to significantly improve progression-free survival vs. placebo in patients with desmoid tumors. Now considered the standard systemic agent for progressive disease.
Nirogacestat: An oral gamma-secretase inhibitor that blocks NOTCH pathway activation. In the international phase III randomized DeFi trial, nirogacestat was associated with significant improvement in PFS, symptom burden, function, and quality of life vs. placebo. It received FDA approval in November 2023 and European approval in August 2025 as the first approved targeted therapy for adults with progressing desmoid tumors requiring systemic treatment. Under evaluation in pediatric patients (NCT04195399). NICE technology appraisal ongoing as of July 2025.
Special Situations
- Pregnancy: Desmoids may grow during pregnancy. Women contemplating pregnancy may be considered for resection pre-pregnancy.
- Mesenteric desmoids (FAP): Primarily medical management. Diversion/bypass may palliate if unresectable. Ureteral obstruction managed with stenting.
- Cervical/thoracic outlet desmoids: Location limits options and increases morbidity; multidisciplinary center management essential.
- Recurrence: Local recurrence linked to larger tumor size, extraabdominal location, and older age. CTNNB1 mutation type also predicts recurrence.
Prognosis
- No metastatic potential - desmoids do not spread to lymph nodes or distant organs
- Morbidity and mortality are entirely from local disease - invasion of vital structures
- R0 resection still results in recurrence ~50% of the time
- Intraabdominal desmoids (especially mesenteric) carry the worst prognosis due to surgical inaccessibility and risk of fatal complications
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1991-2001
- Sabiston Textbook of Surgery, p. 1302
- Current Surgical Therapy 14e, p. 2052-2060
- Mulholland and Greenfield's Surgery, p. 3152-3164
- Campbell's Operative Orthopaedics 15e, p. 3710-3737
- Goldman-Cecil Medicine, p. 1549-1558
- Andrews' Diseases of the Skin, p. 547-549
- Nirogacestat FDA approval (Nov 2023) / EC approval (Aug 2025) - nirogacestat case report PMC12689391
- Sporadic Desmoid Tumor Working Group consensus, JAMA Oncology 2024
This is a shared conversation. Sign in to Orris to start your own chat.