Osteogenic Sarcoma*** - radiologic, gross*, microscopic* findings 1. Rheumatoid Arthritis ( 2. Primary Bone Tumours - classify*, Osteosarcoma* - morphology, clinical course ( 3. Osteomyelitis - define, Pyogenic Osteomyelitis - gross, microscopic features, clinical course (answer in detail covering imp points as welll in exaam point of view 2mbbs pathology refer harsh moham add diagrams as well cover required points for muhs exam Add histo pathology diagram and gross as well
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Here is your complete, MUHS 2nd MBBS Pathology exam-oriented answer covering all three topics, with diagrams from Robbins & Cotran Pathologic Basis of Disease.
🦴 MUHS 2nd MBBS Pathology - Bone Pathology (Exam Notes)
Reference: Robbins & Kumar / Robbins Cotran Pathologic Basis of Disease (Harsh Mohan equivalent content)
TOPIC 1: OSTEOMYELITIS
Definition
Osteomyelitis = Inflammation of bone and bone marrow, almost always due to bacterial infection. It may be acute, subacute, or chronic.
Pyogenic Osteomyelitis
Etiology / Causative Organisms
| Setting | Organism |
|---|---|
| Most common (all ages) | Staphylococcus aureus (80-90% of culture-positive cases) |
| Neonates | Group B Streptococcus, E. coli |
| Older children | Gram-positive organisms (S. aureus) |
| Sickle cell disease | Salmonella and other gram-negative organisms |
| Open fractures/surgery | Mixed bacterial infections |
| Diabetic foot | Polymicrobial |
Exam tip: S. aureus is most common because its cell wall proteins (e.g., fibronectin-binding proteins) bind to bone matrix components such as collagen, facilitating adherence.
Route of Infection (3 routes - imp for exams)
- Hematogenous spread (most common in children)
- Extension from contiguous site (e.g., diabetic foot ulcer)
- Direct implantation after compound fractures or orthopedic procedures
Age-Related Site of Infection
- Neonates: Metaphysis AND epiphysis (metaphyseal vessels cross the growth plate)
- Children: Metaphysis (rich blood supply, sluggish flow, no phagocytes)
- Adults: Epiphysis and subchondral region (after growth plate closure)
GROSS FEATURES of Pyogenic Osteomyelitis
Acute Phase
- Pus formation in medullary cavity
- Suppurative inflammation -> bone necrosis within 48 hours
- Spread via Haversian canals to periosteum
- Subperiosteal abscess formation (periosteum loosely attached in children)
- Rupture of periosteum -> soft tissue abscess -> draining sinus to skin
Chronic Phase - Key Gross Terms (MUST KNOW FOR EXAM)
| Term | Definition |
|---|---|
| Sequestrum | Dead, devitalized bone that has been separated from living bone (appears pale/white, avascular) |
| Involucrum | Shell of new living reactive bone formed around the sequestrum |
| Brodie's abscess | Walled-off subacute abscess in bone |
| Cloaca | Opening in the involucrum through which pus drains |
Gross image - Osteomyelitis (Robbins):
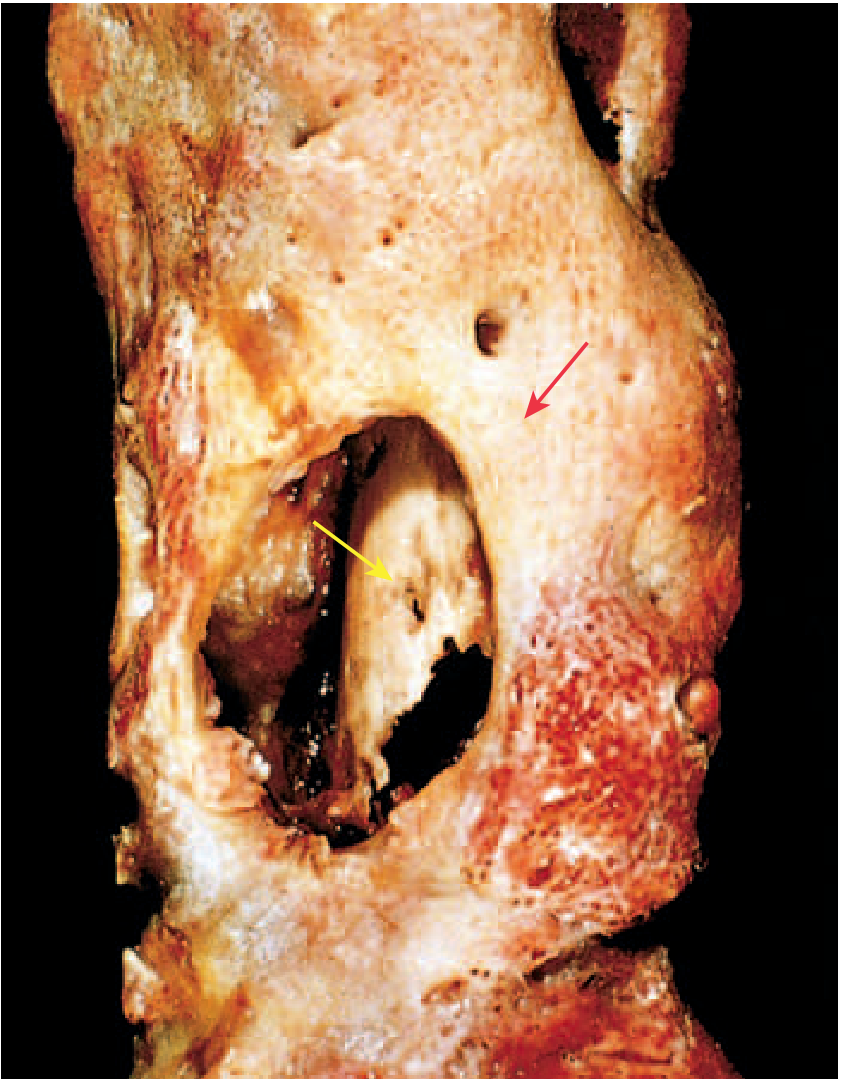
FIG: Resected femur in osteomyelitis - the large cavity contains dead sequestrum (yellow arrow) surrounded by involucrum (red arrow). Drainage tract visible.
MICROSCOPIC FEATURES of Pyogenic Osteomyelitis
Acute Phase (first 48 hours)
- Neutrophilic infiltration of medullary cavity
- Necrosis of bone cells and marrow
- Bacteria proliferating in marrow spaces
Subacute Phase (1-2 weeks)
- Chronic inflammatory cells (lymphocytes, plasma cells, macrophages) appear
- Cytokines stimulate osteoclastic bone resorption
- Fibrous tissue ingrowth begins
- Reactive bone deposition at periphery
Chronic Phase
- Marrow fibrosis
- Sequestrum - dead bone with empty lacunae (osteocytes absent)
- Dense lymphocytic and plasma cell infiltrate
- Granulation tissue with new bone formation (involucrum)
- Draining sinus tracts lined by squamous epithelium
CLINICAL COURSE
Acute Presentation
- Systemic: fever, chills, malaise, leukocytosis
- Local: throbbing pain, tenderness, swelling over affected bone
- Infants: may present with only unexplained fever
- Adults: localized pain
Investigations
- X-ray: lytic focus of bone destruction + reactive bone (changes appear 10-14 days after onset)
- MRI - most sensitive and specific early on
- Blood cultures + bone biopsy for microbial identification
- ESR and CRP elevated
Treatment
- Antibiotics + surgical drainage
Complications (5-25% fail to resolve - become chronic)
- Pathologic fracture
- Septic arthritis (if epiphysis involved - especially in infants)
- Draining sinus with squamous cell carcinoma risk (Marjolin's ulcer)
- Secondary (reactive) amyloidosis
- Endocarditis, sepsis
- Sarcoma in infected bone (rare)
- Osteomyelitis may remain dormant for years and flare up later
Exam Mnemonic for Complications: P-S-D-A-E-S = Pathologic fracture, Septic arthritis, Draining sinus (SCC), Amyloidosis, Endocarditis/sepsis, Sarcoma
TOPIC 2: PRIMARY BONE TUMOURS - Classification + Osteosarcoma
Classification of Primary Bone Tumours
Bone tumors are classified based on the normal cell type they recapitulate or matrix they produce. (Robbins Cotran)
TABLE: Classification of Primary Bone Tumours (MUHS Exam Table)
| Category | Behavior | Tumor | Common Site | Age |
|---|---|---|---|---|
| Bone-forming | Benign | Osteoid osteoma | Femur/tibia cortex | Young males |
| Benign | Osteoblastoma | Vertebral posterior elements | 10-35 yrs | |
| Malignant | Osteosarcoma | Distal femur, proximal tibia | Adolescents | |
| Cartilage-forming | Benign | Osteochondroma | Metaphysis of long bones | 10-30 yrs |
| Benign | Chondroma (Enchondroma) | Small bones of hands/feet | 30-50 yrs | |
| Benign | Chondroblastoma | Epiphysis of long bones | 10-20 yrs | |
| Benign | Chondromyxoid fibroma | Metaphysis | 10-30 yrs | |
| Malignant | Chondrosarcoma | Pelvis, proximal extremities | Adults >40 yrs | |
| Fibrous | Benign | Nonossifying fibroma | Metaphysis of long bones | Children |
| Benign/Malignant | Fibrous dysplasia | Ribs, femur, skull | Teens/adults | |
| Unknown origin | Malignant | Ewing Sarcoma | Diaphysis of femur | 5-20 yrs |
| Benign | Giant cell tumor | Epiphysis of long bones | 20-40 yrs |
Key principle: Benign tumors outnumber malignant ones. In OLDER ADULTS, a bone tumor is more likely to be MALIGNANT (or metastatic).
OSTEOSARCOMA (Osteogenic Sarcoma)
Definition
A malignant tumor that produces osteoid matrix or mineralized bone from malignant osteoblasts. It is the most common primary malignant bone tumor (excluding hematopoietic tumors).
Epidemiology
- Bimodal age distribution:
- 1st peak: 75% before age 20 (adolescent growth spurt) - primary osteosarcoma
- 2nd peak: Older adults - secondary osteosarcoma (in setting of Paget disease, bone infarcts, prior radiation)
- M:F = 1.6:1 (males more commonly affected)
- Location: Metaphysis of long bones - 50% around the knee (distal femur > proximal tibia > proximal humerus)
Predisposing Factors (Secondary Osteosarcoma)
- Paget disease of bone
- Bone infarcts
- Prior radiation therapy
- Germline RB mutations (1000x increased risk)
- Li-Fraumeni syndrome (TP53 mutations)
Molecular Pathogenesis
| Gene | Role |
|---|---|
| RB gene | Mutated in 70% of sporadic cases |
| TP53 | Mutated in Li-Fraumeni syndrome; common in sporadic tumors |
| MDM2 / CDK4 | Overexpressed in low-grade osteosarcomas |
| CDKN2A (INK4a) | Inactivated - encodes p16 and p14 |
| MYC | Amplified in ~50% - associated with poor prognosis |
RADIOLOGICAL FINDINGS of Osteosarcoma
- Large, destructive, mixed lytic and sclerotic mass with infiltrative margins
- Codman triangle (MOST IMPORTANT SIGN):
- Periosteum is lifted by tumor -> triangular wedge of reactive subperiosteal bone = Codman triangle
- Indicates aggressive tumor but is NOT pathognomonic (also seen in Ewing sarcoma, infection)
- Sunburst pattern - bone formation extending into soft tissue in radiating spicules
- Tumor confined to metaphyseal side of growth plate (does not cross epiphyseal plate)
- Extension into soft tissue frequently seen
Radiograph - Osteosarcoma of distal femur (Robbins):

FIG 19.15: Distal femur osteosarcoma - large destructive mass with prominent bone formation extending into soft tissue. Arrow = Codman triangle (triangular periosteal reactive bone). (Robbins Basic Pathology)
GROSS FINDINGS of Osteosarcoma
- Bulky tumor in the metaphysis
- Gritty, tan-white cut surface (due to calcified/ossified areas)
- Areas of hemorrhage and necrosis (giving brownish discoloration)
- Cortical destruction - breaks through cortex and invades soft tissue
- Intramedullary spread - infiltrates and replaces marrow
- Subperiosteal expansion prominent
- Epiphyseal plate usually NOT crossed (tumor stays in metaphysis)
- Infrequently, tumor may penetrate the epiphyseal plate and enter the joint
Gross specimen - Osteosarcoma distal femur (Robbins):

FIG 19.16: Osteosarcoma of distal femur. Extensive cortical disruption and subperiosteal expansion. Tumor is confined to the metaphyseal side of the cartilaginous growth plate. Hemorrhagic area = biopsy site. (Robbins)
MICROSCOPIC (HISTOPATHOLOGY) FINDINGS of Osteosarcoma
Key Histological Features:
- Malignant tumor cells with pleomorphism
- Large hyperchromatic nuclei
- Bizarre tumor giant cells
- Abundant mitoses including abnormal (bipolar/tripolar) mitotic figures
- Production of osteoid (DIAGNOSTIC CRITERION)
- Fine, lacelike unmineralized osteoid OR broad sheets OR primitive trabeculae
- Malignant cells must be seen producing the osteoid - this is the sine qua non of diagnosis
- Extensive necrosis
- Intravascular invasion (lymphovascular invasion)
- Preexisting lamellar bone bridged by lacelike osteoid ("bridges" preexisting bone)
Histopathology - Osteosarcoma (Robbins):
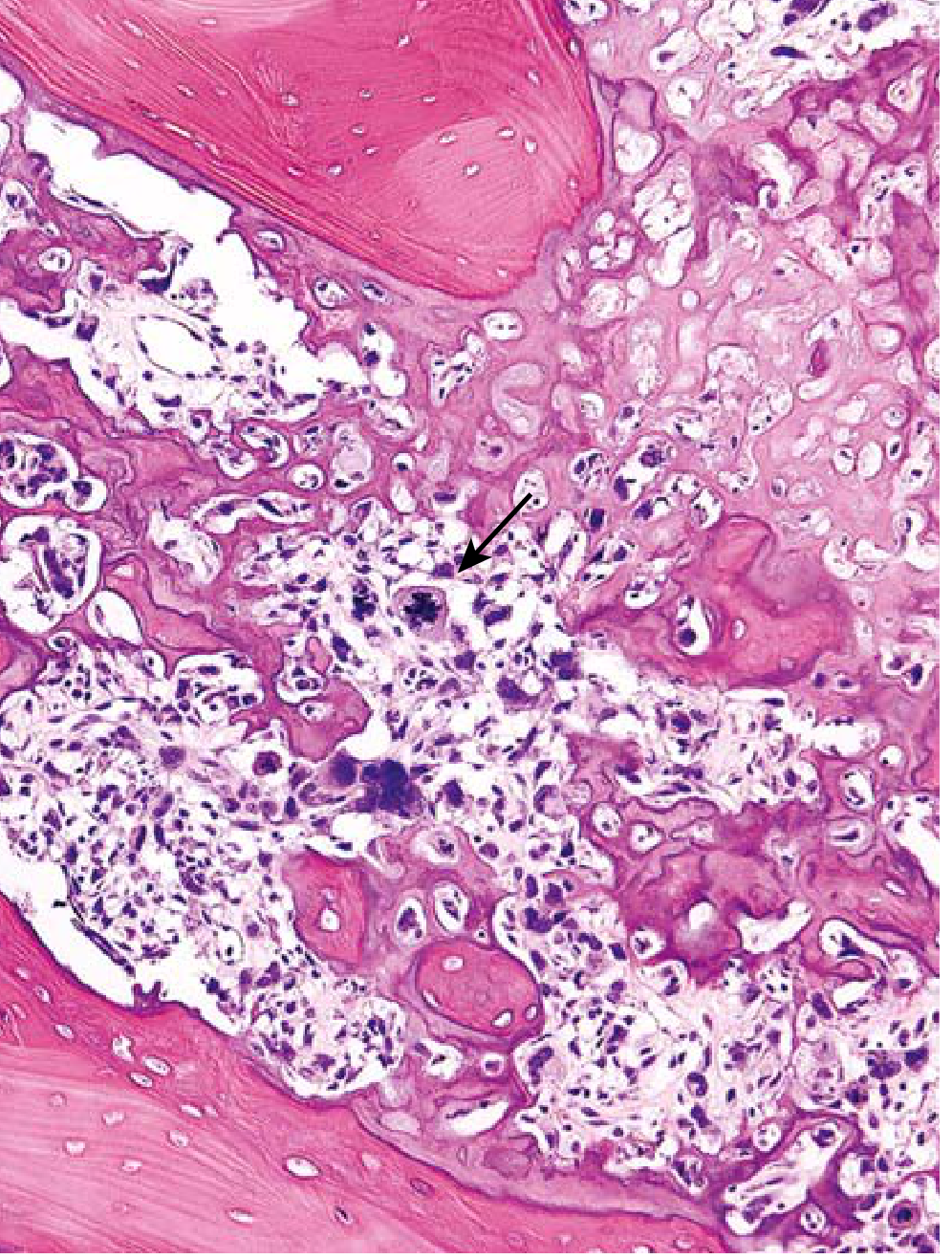
FIG 19.17: Lacelike osteoid produced by pleomorphic malignant tumor cells bridges preexisting lamellar bone. Note the abnormal mitotic figure (arrow). (Robbins Basic Pathology)
Important Histological Variants
| Variant | Feature |
|---|---|
| Osteoblastic | Predominantly osteoid/bone production (most common) |
| Chondroblastic | Prominent cartilage matrix |
| Fibroblastic | Predominantly spindle cells, less osteoid |
| Telangiectatic | Cystic spaces filled with blood (simulates ABC on radiology) |
| Small cell | Resembles Ewing sarcoma |
CLINICAL COURSE of Osteosarcoma
Presentation
- Painful, progressively enlarging mass in the metaphysis of a long bone
- Often adolescent with knee pain / swelling
- Pathologic fracture may be the first sign
Behavior
- All osteosarcomas assumed to have occult metastases at diagnosis
- Metastasizes hematogenously to: Lungs > bones > brain > other sites
Treatment
- Neoadjuvant chemotherapy (pre-operative) + Surgery (limb salvage or amputation) + Post-operative adjuvant chemotherapy
- Key chemotherapy agents: Doxorubicin, Cisplatin, Methotrexate (high-dose), Ifosfamide
Prognosis
- 5-year survival: ~70% in patients without overt metastases at diagnosis
- With clinically evident metastases, recurrent disease, or secondary osteosarcoma: 5-year survival <20%
- Histologic response to neoadjuvant chemotherapy is the best prognostic indicator
TOPIC 3: RHEUMATOID ARTHRITIS
Definition
Rheumatoid Arthritis (RA) = A chronic systemic autoimmune disorder that principally attacks the synovial joints, producing a nonsuppurative, proliferative and inflammatory synovitis, which often progresses to destruction of articular cartilage and, in some cases, joint fusion (ankylosis).
- Prevalence: 0.25-1% of the population
- F:M = 3:1 (three times more common in females)
- Peak incidence: 3rd to 5th decades of life
Pathogenesis
Key Mechanism
- Initiated by CD4+ helper T cells reacting to a joint antigen (collagen, citrullinated peptides)
- Molecular mimicry: citrullinated vinculin mimics microbial epitopes -> presented by HLA-DR4
- HLA-DR4 allele strongly associated with ACPA-positive RA
Key Inflammatory Mediators
| Mediator | Source | Effect |
|---|---|---|
| TNF | Macrophages | Key mediator; recruits leukocytes, activates synoviocytes to produce proteases -> cartilage destruction |
| IL-1, IL-6 | Macrophages | Inflammation, acute phase response |
| IL-17 | Th17 cells | Recruits neutrophils and monocytes |
| RANKL | Activated T cells | Stimulates osteoclasts -> bone resorption |
| IFN-γ | Th1 cells | Activates macrophages |
Autoantibodies
- ACPA (Anti-citrullinated peptide antibody): Present in 70% of RA patients - diagnostic marker
- Rheumatoid Factor (RF): IgM or IgA antibodies against Fc region of IgG; present in 80% of RA patients
- RF deposits in joints as immune complexes
- NOT specific to RA (also present in some healthy individuals and other diseases)
- ~20% of patients are seronegative (no RF or ACPA)
MORPHOLOGY (Histopathology)
Joint Changes (Synovium)
The synovium becomes edematous, thickened, and hyperplastic. Five characteristic histologic features:
- Synoviocyte hyperplasia and proliferation (synovial lining becomes multilayered)
- Dense inflammatory infiltrates - CD4+ T cells, B cells, plasma cells, macrophages, dendritic cells; lymphoid follicles with germinal centers
- Increased vascularity (angiogenesis)
- Fibrin-rich exudate with neutrophils on synovial and joint surfaces
- Osteoclastic activity in subchondral bone -> periarticular erosions and subchondral cysts
PANNUS (KEY TERM - MUST KNOW)
Pannus = A mass of edematous synovium + inflammatory cells + granulation tissue + fibroblasts that grows over and erodes the articular cartilage.
- Pannus destroys articular cartilage
- In advanced disease, pannus bridges apposing bones -> fibrous ankylosis
- Fibrous ankylosis eventually ossifies -> bony ankylosis (joint fusion)
RA Joint Diagram and Histopathology (Robbins):
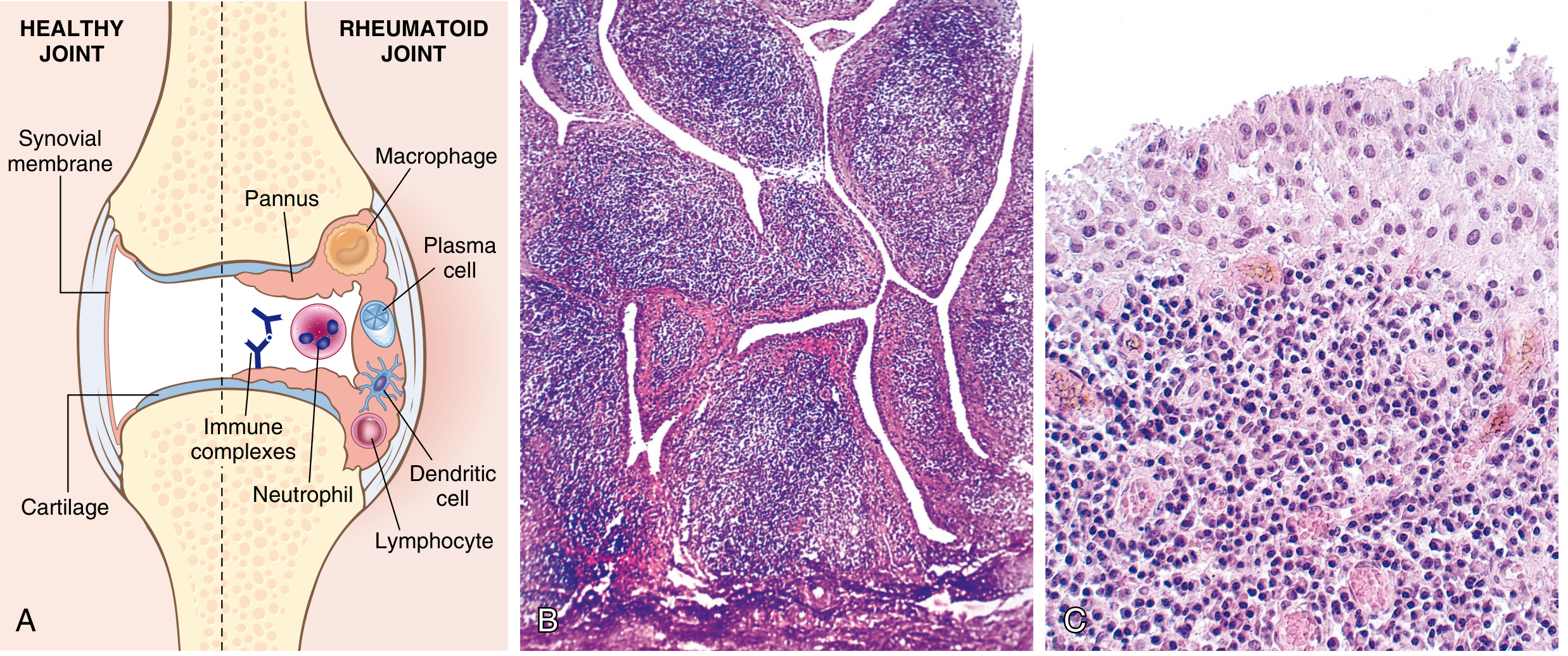
FIG 26.34: Rheumatoid arthritis. (A) Schematic of rheumatoid joint showing pannus formation, macrophages, plasma cells, neutrophils, immune complexes destroying cartilage. (B) Synovial hypertrophy with villi (low power). (C) Dense lymphoid aggregate in subsynovial tissue (high power). (Robbins Cotran)
Rheumatoid Nodules
- Infrequent manifestation
- Located subcutaneously over: forearm, elbows, occiput, lumbosacral area
- Gross: Small, firm, nontender, oval masses
- Micro: Central zone of fibrinoid necrosis surrounded by palisaded macrophages (activated), with lymphocytes and plasma cells at periphery
- Resemble necrotizing granulomas
Rheumatoid Nodule (Robbins):
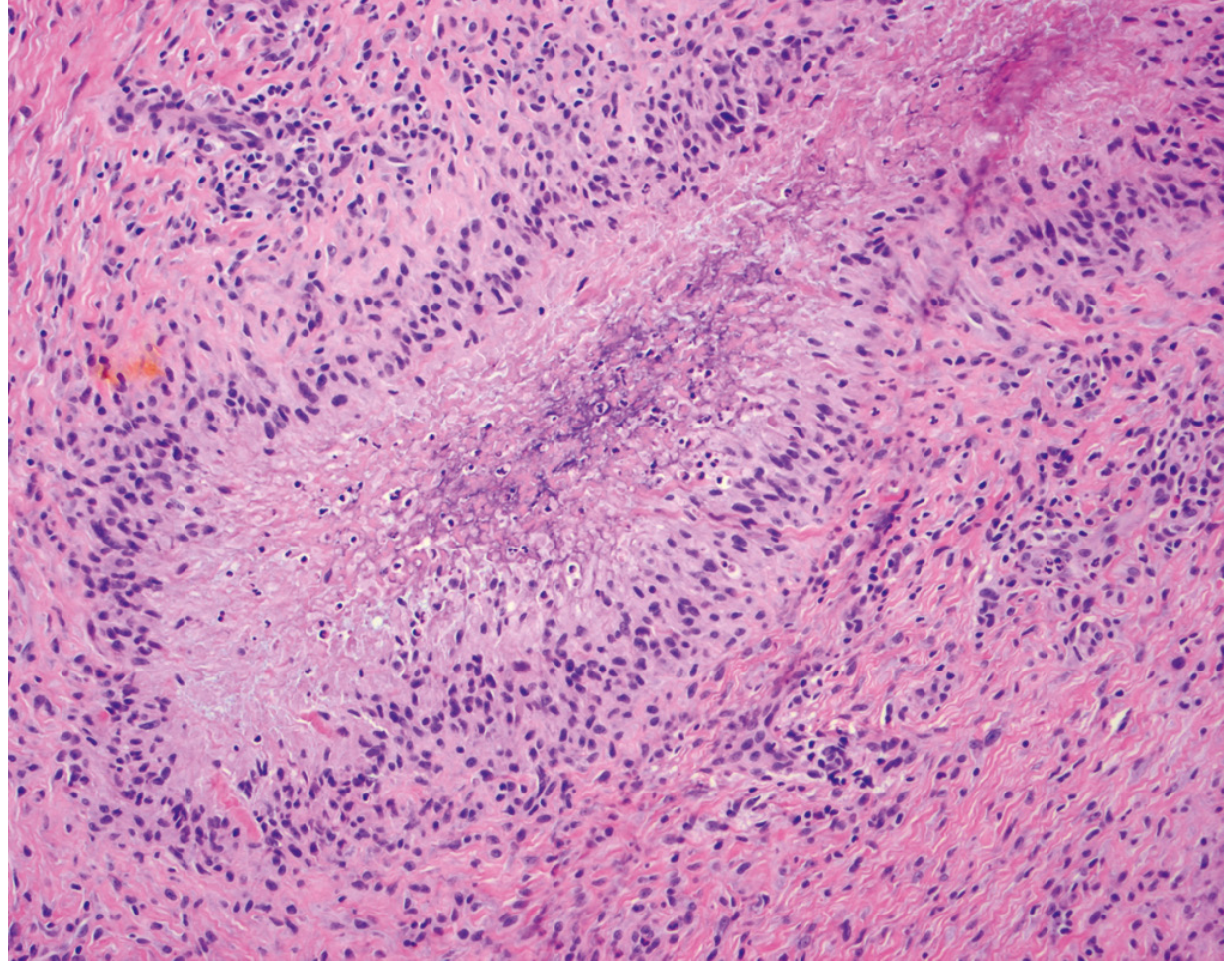
FIG 26.35: Rheumatoid nodule with central necrosis rimmed by palisaded macrophages. (Robbins Cotran)
Extraarticular Manifestations
- Skin: Rheumatoid nodules, vasculitis
- Lungs: Interstitial lung disease, rheumatoid nodules, pleural effusion
- Heart: Pericarditis, rheumatoid nodules in myocardium
- Vessels: Leukocytoclastic vasculitis
- Eyes: Uveitis, keratoconjunctivitis sicca (Sjogren overlap)
CLINICAL FEATURES of Rheumatoid Arthritis
Onset
- Insidious: malaise, fatigue, generalized musculoskeletal pain over weeks-months
- Then joints become involved
Joint Distribution (Symmetric Polyarthritis)
- Hands and feet first -> wrists, ankles, elbows, knees
- MCP (Metacarpophalangeal) and PIP (Proximal Interphalangeal) joints involved
- (Unlike OA which affects DIP joints)
- Symmetric involvement - bilateral
Symptoms
- Morning stiffness lasting >1 hour (key distinguishing feature from OA)
- Warm, swollen, painful joints
- Waxing and waning course
- Progressive joint enlargement and decreased range of motion
Deformities (Chronic RA - Exam Favourites)
| Deformity | Mechanism |
|---|---|
| Ulnar deviation of fingers | Inflammation of MCP joints + tendon involvement |
| Swan-neck deformity | Hyperextension of PIP + flexion of DIP |
| Boutonniere deformity | Flexion of PIP + hyperextension of DIP |
| Z-deformity of thumb | Flexion of MCP + hyperextension of IP joint |
Radiographic Hallmarks
- Joint effusions
- Juxtaarticular osteopenia (periarticular bone loss)
- Erosion and narrowing of joint space
- Loss of articular cartilage
Diagnosis
- ACPA positive (~70%)
- Rheumatoid factor positive (~80%)
- 20% are seronegative - diagnosis by clinical/radiographic findings
- ACR/EULAR criteria used
Treatment
- NSAIDs (symptomatic)
- Corticosteroids
- DMARDs: Methotrexate (cornerstone)
- Biologic agents: TNF antagonists (Infliximab, Etanercept, Adalimumab) - most important advance; not curative, must be maintained
- Risk: Reactivation of latent TB with anti-TNF therapy
- Other biologics: Anti-IL-6 (Tocilizumab), Anti-CD20 (Rituximab), CTLA4-Ig (Abatacept)
Comparison: RA vs OA (MUHS Exam Favourite Table)
| Feature | Rheumatoid Arthritis | Osteoarthritis |
|---|---|---|
| Nature | Autoimmune/inflammatory | Degenerative |
| Age | 30-50 yrs | >50 yrs |
| Sex | F > M (3:1) | F > M (post-menopausal) |
| Joints involved | MCP, PIP - symmetric | DIP, weight-bearing joints |
| Morning stiffness | >1 hour | <30 minutes |
| Synovitis | Prominent (pannus) | Mild/secondary |
| RF/ACPA | Positive (80%/70%) | Negative |
| Histology | Pannus, lymphocytic infiltrate, germinal centers | Cartilage fibrillation, osteophytes |
| X-ray | Erosions, juxta-articular osteopenia | Osteophytes, joint space narrowing, subchondral sclerosis |
| Systemic features | Yes (nodules, vasculitis, lung, heart) | No |
QUICK REVISION BOXES (Exam Points)
Osteomyelitis - Must Remember
Sequestrum = dead bone | Involucrum = new bone around sequestrum | Cloaca = opening in involucrum Most common organism = S. aureus Site in children = Metaphysis Most sensitive investigation early = MRI
Osteosarcoma - Must Remember
Most common primary malignant bone tumor (excluding hematopoietic) Age peak = adolescents | Site = distal femur / proximal tibia (around knee) X-ray = Codman triangle + sunburst pattern | Gross = gritty, tan-white, hemorrhagic Micro = lacelike osteoid from pleomorphic malignant cells + abnormal mitoses Prognosis = 70% 5-year survival with chemotherapy + surgery (without metastases) Genes = RB (70%), TP53, MYC amplification
Rheumatoid Arthritis - Must Remember
Autoimmune | F:M = 3:1 | Peak 30-50 yrs Key lesion = PANNUS (synovium + inflammatory cells + granulation tissue + fibroblasts) Antibodies = RF (80%) + ACPA (70%) Histology = synoviocyte hyperplasia, lymphoid follicles, fibrinoid necrosis (nodules) Deformities = ulnar deviation, swan-neck, boutonniere Treatment = MTX + TNF antagonists | Morning stiffness >1 hr is key feature Complications = fibrous/bony ankylosis, AA amyloidosis, atlantoaxial subluxation (C1-C2 cervical spine - dangerous!)
Sources: Robbins & Kumar Basic Pathology (9780323790185) and Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528)
This is a shared conversation. Sign in to Orris to start your own chat.