Dandy walker syndrome
Reading File
Finding Sources
Searching PubMed
Dandy-Walker syndrome
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Dandy-Walker Syndrome (DWS)
Definition and Spectrum
Dandy-Walker malformation (DWM) describes a spectrum of cystic posterior fossa malformations. The classic (most severe) form has three cardinal features:
- Cystic dilation of the fourth ventricle (ballooning of the posterior half of the fourth ventricle, often with failure of patency of the foramen of Magendie)
- Aplasia or hypoplasia of the cerebellar vermis (with vermian rotation and splaying of the cerebellar hemispheres)
- Enlargement of the posterior fossa with elevation of the tentorium, torcular herophili, and straight sinus above the lambdoid suture
- Bradley and Daroff's Neurology in Clinical Practice
- Creasy & Resnik's Maternal-Fetal Medicine
The Posterior Fossa Spectrum (Mildest to Severest)
| Entity | Key Feature |
|---|---|
| Mega cisterna magna | Normal cerebellum + fourth ventricle; infracerebellar CSF expansion; incidental, no significance |
| Blake pouch cyst | Failure of foramen of Magendie to perforate; normal vermis; obstructive hydrocephalus may develop |
| DW Variant | Partial vermian hypoplasia, mild posterior fossa enlargement |
| Classic DWM | Full triad: fourth ventricle cyst, vermis aplasia, posterior fossa enlargement |
Posterior fossa arachnoid cysts are not in continuity with the fourth ventricle and are distinguished by mass effect and absence of vermian dysplasia.
- Grainger & Allison's Diagnostic Radiology
Epidemiology and Pathogenesis
-
Incidence: 1 in 30,000 births
-
Accounts for 4-12% of all infantile hydrocephaly
-
Results from developmental arrest in the hindbrain between 4-6 weeks of gestation
-
Various incomplete forms (DW variants) are described; classification remains debated
-
Creasy & Resnik's Maternal-Fetal Medicine
Clinical Presentation
Infants typically present with:
- Macrocephaly (from progressive hydrocephalus)
- Developmental delay (motor and cognitive)
- Hydrocephalus - present in 70-80% of cases, with progressive postnatal ventriculomegaly
- Seizures
- Signs of cerebellar dysfunction (ataxia, hypotonia)
Neurological handicaps (spastic diplegia, intellectual disability) relate more to associated brain malformations than to the hydrocephalus itself.
- Bailey & Love's Short Practice of Surgery
- Bradley and Daroff's Neurology in Clinical Practice
Key Diagnostic Features (Imaging)
MRI and CT findings:
- Large cisterna magna communicating with the fourth ventricle
- Absent or hypoplastic vermis
- Cerebellar hemispheres splayed apart
- Elevated tentorium and torcular herophili (torcular-lambdoid inversion - torcular above lambdoid suture, visible on plain X-ray, CT, and MRI)
- Ventriculomegaly / hydrocephalus
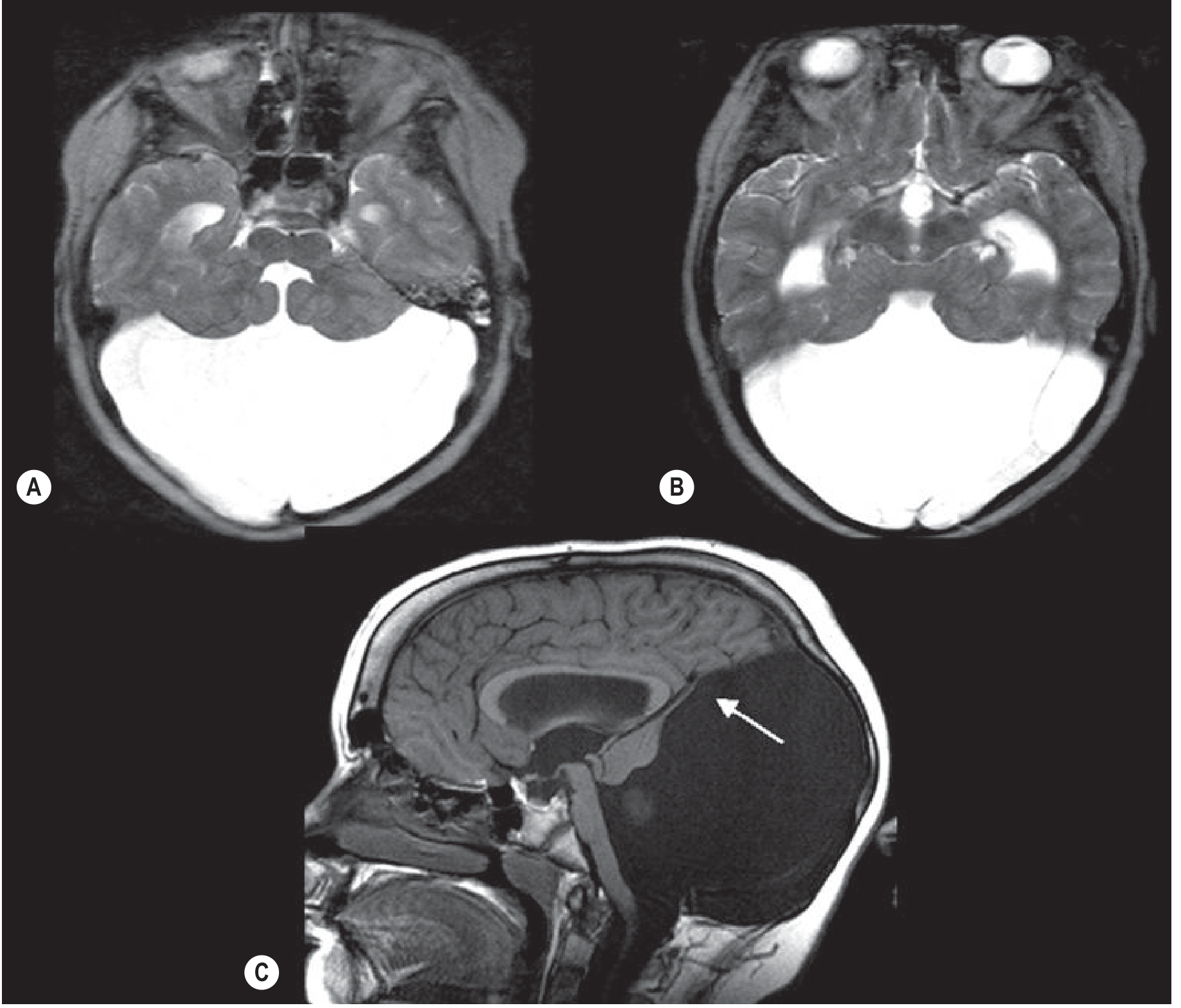
The MRI below shows the classic findings - the fourth ventricle opens into a large posterior fossa cyst, the cerebellum is hypoplastic with a thin rim of cerebellar tissue forming the cyst wall (arrow), and the venous structures are elevated:
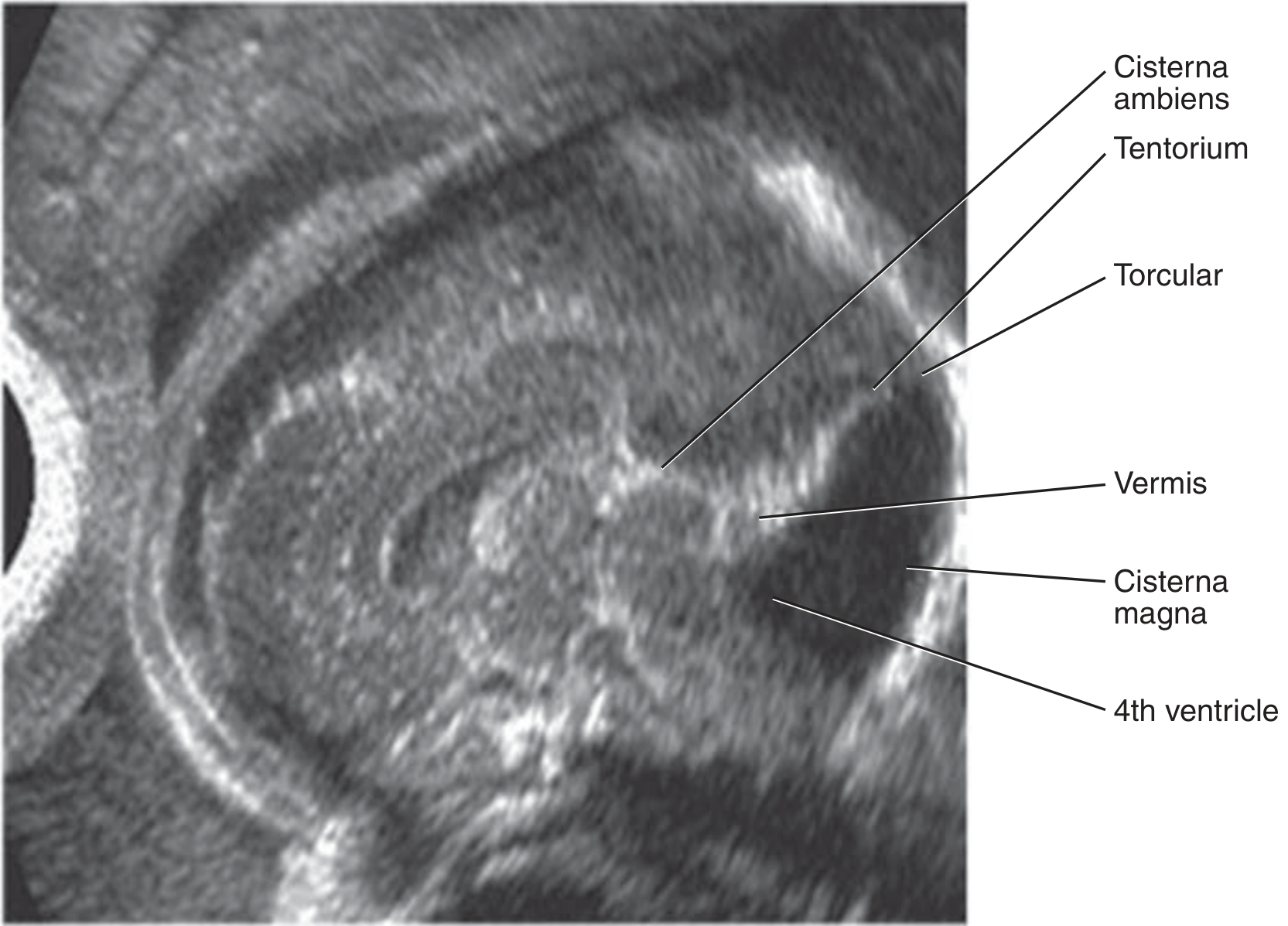
Fetal ultrasound (median view): shows large posterior fossa with elevated tentorium and torcular, communicating fourth ventricle, and hypoplastic upwardly-rotated vermis:
Differential Diagnosis
- Posterior fossa arachnoid cyst (no communication with 4th ventricle)
- Blake pouch cyst
- Mega cisterna magna
- Vermian hypoplasia (isolated)
- Joubert syndrome (molar tooth sign on MRI, ciliopathy)
Associated Anomalies
Found in 50-70% of postnatal cases and ~60% of prenatally diagnosed cases.
CNS anomalies (most common):
- Agenesis or dysgenesis of the corpus callosum
- Holoprosencephaly
- Cephaloceles
- Cortical migrational disorders (pachygyria, heterotopias)
- Inferior olivary heterotopia
Non-CNS anomalies:
- Congenital heart disease
- Craniofacial anomalies
- Renal and limb anomalies
- Abdominal wall defects, diaphragmatic hernia
- Ambiguous genitalia
- Fetal growth restriction
Chromosomal anomalies:
- Trisomy 9, 21, 18, 13
- Triploidy
- 6p and 3q22-q24 deletions
Genetic syndromes:
-
Walker-Warburg syndrome (congenital muscular dystrophy)
-
Joubert syndrome (ciliopathy)
-
Meckel-Gruber syndrome (ciliopathy)
-
Lissencephaly (tubulopathies)
-
Blake pouch cyst: ZIC2 and ZIC5 gene haploinsufficiency (distal 13q deletion)
-
Creasy & Resnik's Maternal-Fetal Medicine
Management
Postnatal
- Shunt placement is the primary treatment for hydrocephalus (ventriculoperitoneal shunt or cyst-peritoneal shunt)
- Multidisciplinary care: neurology, neurosurgery, developmental pediatrics
- Long-term developmental support and rehabilitation
Antenatal (Prenatal Diagnosis)
When identified on fetal ultrasound:
-
Detailed anatomic survey
-
Fetal neurosonography
-
Fetal echocardiography
-
Genetic counseling; karyotype, subtelomeric deletion testing, chromosomal microarray
-
Fetal MRI (to identify associated anomalies more precisely)
-
Consultation with maternal-fetal medicine, neonatology, pediatric neurology
-
Offer termination of pregnancy
-
For ongoing pregnancies: serial scans to monitor ventriculomegaly progression
-
Vaginal delivery is not contraindicated
-
Creasy & Resnik's Maternal-Fetal Medicine; Bailey & Love's Short Practice of Surgery
Prognosis
- If hydrocephalus is treated promptly, prognosis may be good
- Outcome depends heavily on the extent and severity of associated brain malformations, not hydrocephalus alone
- Isolated DWM without associated anomalies carries a better prognosis
- Intellectual disability, spastic diplegia, and cerebellar dysfunction are common long-term sequelae
Recent Evidence (2025)
Two recent systematic reviews are relevant:
- A 2025 systematic review (PMID 41396485) examined DWM with occipital encephalocele - a particularly severe association
- A 2025 meta-analysis (PMID 40785453) on outcomes of isolated fetal posterior fossa anomalies provides updated prognostic data that may refine counseling for prenatally diagnosed cases
Sources: Bradley and Daroff's Neurology in Clinical Practice | Grainger & Allison's Diagnostic Radiology | Creasy & Resnik's Maternal-Fetal Medicine | Bailey & Love's Short Practice of Surgery | Adams and Victor's Principles of Neurology
This is a shared conversation. Sign in to Orris to start your own chat.