Cicatricial ectropion
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching PubMed
cicatricial ectropion surgery treatment
Loading Image
Here is a complete, structured overview of cicatricial ectropion based on Kanski's Clinical Ophthalmology (10th ed.) and Wills Eye Manual.
Cicatricial Ectropion
Definition and Mechanism
Cicatricial ectropion is outward turning (eversion) of the eyelid margin caused by scarring or contracture of the anterior lamella (skin and underlying subcutaneous tissues), which pulls the eyelid away from the globe. The pathology is fundamentally a vertical deficiency of the anterior lamella - the shortened, scarred skin tethers the eyelid downward and outward.
Clinical bedside test: Pushing the skin upward over the orbital margin with a finger temporarily relieves the ectropion. Opening the mouth tends to accentuate the eversion (because facial skin is placed under tension).

Causes
The defect may be local or generalized:
| Type | Examples |
|---|---|
| Trauma | Lacerations, post-surgical scarring (blepharoplasty, subciliary incision) |
| Burns | Thermal, chemical |
| Skin disease | Eczema/contact dermatitis, ichthyosis, actinic damage |
| Chronic inflammation | Chronic dermatitis, rosacea |
| Infection | Herpes zoster |
| Tumor excision | Post-Mohs or excisional surgery |
Both upper and lower lids may be involved depending on the cause. Generalized causes (burns, ichthyosis) tend to involve both lids and multiple areas.
Symptoms
- Tearing (epiphora) - from punctal malposition and lacrimal pump failure
- Irritation and redness
- Mucous discharge
- May be asymptomatic in mild cases
Signs
Critical:
- Outward turning of the eyelid margin
Other:
- Eyelid skin scarring (key distinguishing feature from involutional ectropion)
- Superficial punctate keratopathy (SPK) from corneal exposure
- Conjunctival injection, thickening, and eventual keratinization from chronic dryness
- Exposed, inflamed palpebral conjunctiva
Workup
- History - prior surgery, trauma, chemical burns, skin disease
- External examination - assess orbicularis oculi function, horizontal eyelid laxity, punctal location; look for scarring, eyelid tumors
- Slit lamp examination - evaluate for exposure keratopathy and conjunctival inflammation
Treatment
Medical (temporizing)
- Lubricating drops and ointments to address exposure keratopathy
- Warm compresses + antibiotic ointment (e.g., bacitracin or erythromycin q.i.d.) for inflamed exposed eyelid margin
- Short course of antibiotic-steroid combination ointment if closely monitored
- Eyelid taping as a temporizing measure
Surgical (definitive)
Definitive treatment requires addressing the vertical skin deficit. The approach depends on severity and extent:
| Severity | Procedure |
|---|---|
| Mild, localized | Excision of offending scar tissue + Z-plasty (lengthens vertical skin deficiency) |
| Moderate, localized | Local transposition flaps |
| Severe or generalized | Free skin grafts - full-thickness preferred |
Skin graft donor sites: upper eyelids, posterior auricular (retroauricular), preauricular, supraclavicular areas.
The key principle is always to add vertical dimension to the anterior lamella - horizontal procedures alone (as used for involutional ectropion) are insufficient and will fail.
Comparison with Other Ectropion Types
| Feature | Cicatricial | Involutional | Paralytic |
|---|---|---|---|
| Mechanism | Anterior lamellar shortening | Horizontal eyelid laxity | CN VII palsy |
| Bedside test | Finger pushes skin up - relieved | Snap/distraction test positive | Associated lagophthalmos |
| Surgery | Vertical augmentation (Z-plasty/graft) | Horizontal tightening (tarsal strip) | Canthoplasty/weight implant |
| Both lids? | Possible (e.g., burns) | Usually lower lid | Upper + lower |
Key Points
- The hallmark is scarring of the anterior lamella pulling the lid outward - treatment must always address the vertical skin deficit.
- Z-plasty is the workhorse for mild localized cases; it lengthens the scar while redirecting tension vectors.
- Full-thickness skin grafts are preferred over split-thickness grafts for reconstruction because split-thickness grafts are more prone to secondary contracture, which risks recurrence of the ectropion.
- Reconstruction after tumor excision (subciliary approach) is a recognized surgical cause.
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., p. 84; Wills Eye Manual, 7th ed., p. 384-386
Surgeries in detail
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Excellent - I now have comprehensive material from multiple textbooks. Here is the detailed surgical answer:
Surgical Treatment of Cicatricial Ectropion - In Detail
The fundamental surgical principle is the same for every case: vertical skin deficiency must be corrected by adding or rearranging tissue - horizontal tightening procedures alone (used for involutional ectropion) are both ineffective and contraindicated here.
Surgical Options by Severity
| Severity | Procedure |
|---|---|
| Mild, localized | Scar excision + Z-plasty |
| Moderate, localized | Local transposition/rotation flaps |
| Severe or generalized | Free skin grafts (full-thickness preferred) |
1. Z-Plasty (Mild Localized Cases)
Principle
Z-plasty is a transposition flap technique that lengthens a contracted scar while simultaneously redirecting it along more favorable lines.
Mechanism
- The scar forms the central limb of the "Z"
- Two triangular flaps are raised from each end of the scar at equal angles
- The two flaps are then "flip-flopped" - transposed into each other's original positions
- This borrows tissue from the width of the scar to gain length in its longitudinal axis
Geometry
- Classic 60-degree Z-plasty = the limbs are cut at 60° to the central scar
- Gain in length = 75% of the original scar length
- The scar is redirected 90 degrees from its original axis
- Angles can range from 30° to 90°: wider angles give greater length gain but more tension on closure
- All three limbs (central + two arms) must be of equal length
Steps
- Mark the contracted scar as the central limb
- Mark two limbs of equal length at 60° from each end of the central limb (in opposite directions, creating the "Z" shape)
- Incise along all three lines
- Elevate the two triangular subcutaneous flaps
- Transpose them: flap A goes into flap B's bed and vice versa
- Close with fine absorbable sutures
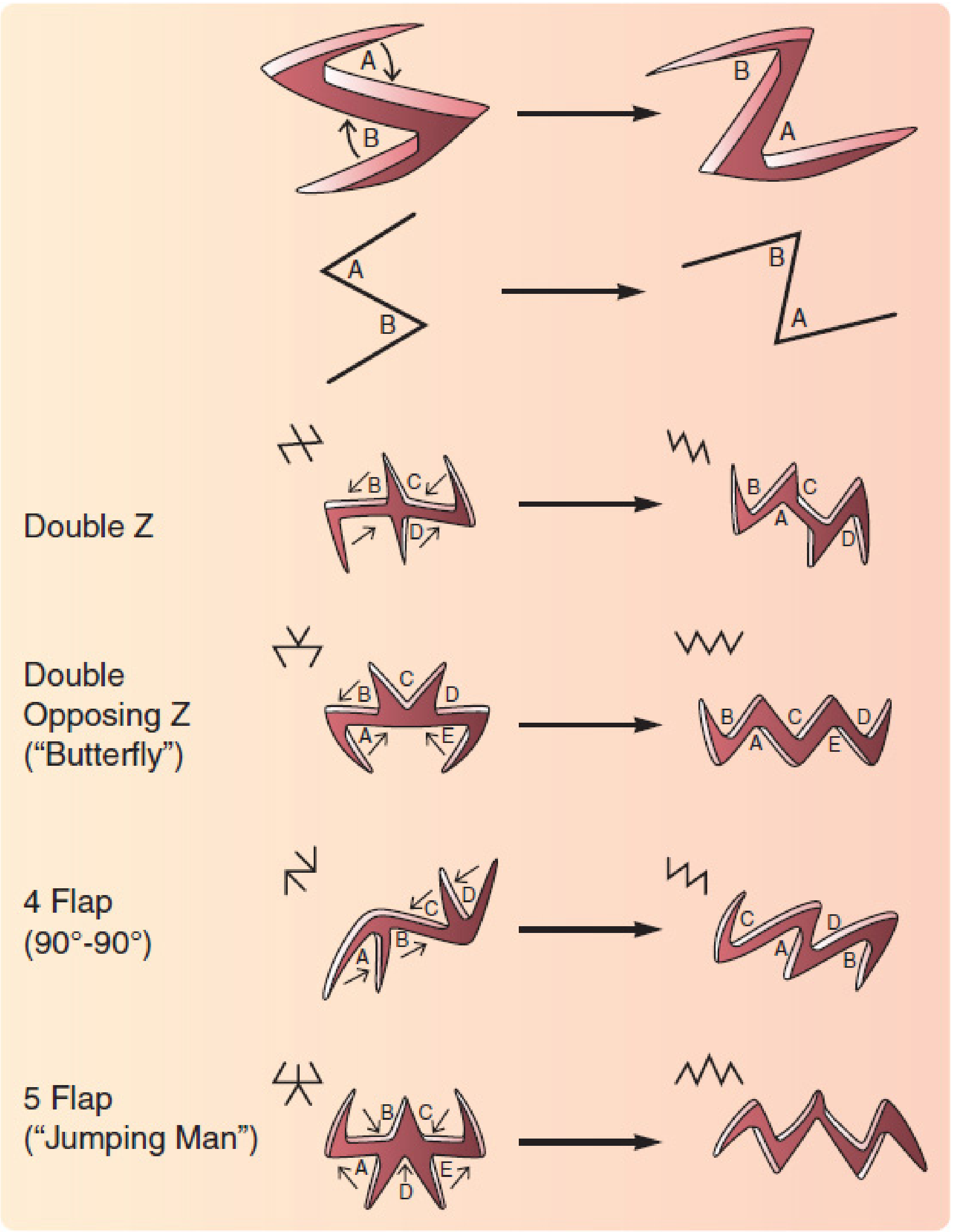
Variants for larger areas
- Multiple serial Z-plasties: designed end-to-end along a long contracted scar - each unit provides incremental lengthening
- Double Z / Double opposing Z ("Butterfly"): used when more lengthening is needed without a single large transposition
- 4-flap Z-plasty (90°-90°) and 5-flap ("Jumping Man"): for extensive contractures, provide greater length gain with lower individual flap tension
Advantages
- Uses local tissue (best color and texture match)
- No donor site scar elsewhere on the face
- Single-stage procedure
Disadvantage
- Increases total incision length (the new zigzag lines can be harder to camouflage than a linear scar)
2. Local Transposition / Rotation Flaps (Moderate Cases)
When the defect is too large for Z-plasty alone, local flaps borrow tissue from adjacent areas:
Rhombic (Limberg) Transposition Flap
- A rhomboid-shaped flap is designed adjacent to the scar defect
- The flap is elevated and transposed over the intervening tissue into the primary defect
- The key suture closes the secondary defect; the flap is then inset into the primary defect
- Useful for moderate-sized localized defects near the lower lid
Cheek Rotation-Advancement Flap
- For larger periorbital defects following tumor excision
- Tissue is recruited from the cheek, which has good color and contour match to the lower eyelid skin
- Incisions are camouflaged along the nasolabial fold and infraorbital rim
- Risk: if flap is too small or contracts, it may itself cause recurrent ectropion - careful vector planning is essential
V-Y Advancement Flap
- Useful when healthy tissue surrounds the scar and can be advanced into the contracture release area
- Lengthens in the direction of the V-Y conversion without the added incisions of a Z-plasty
3. Free Skin Grafts (Severe or Generalized Cases)
When local tissue is insufficient (e.g., extensive burns, widespread dermatitis, ichthyosis), free skin grafts are required.
Full-Thickness Skin Graft (FTSG) - Preferred
Why FTSG over split-thickness?
- FTSG contracts significantly less than split-thickness grafts (STSGs)
- Less secondary contracture = lower risk of recurrent ectropion
- Better color, texture, and thickness match for the thin eyelid skin
- Particularly important near free margins (eyelid, lip) where contracture causes functional problems
Donor sites (in order of preference for eyelid reconstruction):
| Donor Site | Notes |
|---|---|
| Contralateral upper eyelid | Best color + thickness match; surplus skin often available in older patients |
| Retroauricular (post-auricular) | Thin, pliable; excellent color match; concealed scar |
| Preauricular | Good match; slightly thicker than post-auricular |
| Supraclavicular | For larger grafts; slightly thicker |
Technique overview:
- Release the cicatricial scar completely (excise or widely undermine) until the eyelid returns to its natural position against the globe
- Measure the resulting skin deficit carefully with the eyelid held in correct position
- Harvest the full-thickness graft from the donor site (including dermis, excluding subcutaneous fat)
- Defat the graft, trim to size
- Suture into the defect under slight tension to account for some primary contraction
- Apply a firm bolster dressing to maximize graft-bed contact and prevent seroma/hematoma
- Leave bolster for 5-7 days
Split-Thickness Skin Graft (STSG) - Less Preferred
- Technically easier to harvest (dermatome)
- Larger surface areas possible
- However, STSGs contract more, risking recurrent ectropion
- Some authors accept STSG for the upper lid (where thin pliable skin can be better matched) but FTSG is still preferred for the lower lid
- The high rate of graft contracture following STSG reconstruction is a well-documented complication of eyelid burns reconstruction
4. Cicatrix Release + Spacer Grafts (Middle Lamellar Involvement)
When scarring involves the middle lamella (orbital septum / subconjunctival plane) rather than just the anterior lamella - as may occur after blepharoplasty or deep burns:
- The cicatricial adhesions are lysed (released)
- A spacer graft is placed to prevent re-adhesion: hard palate mucosal graft or acellular dermal allograft substitute
- This corrects lower eyelid retraction with ectropion where the septum is the contracted structure
Key Surgical Principles (Summary)
- Always correct the vertical deficit - horizontal tightening will fail and may worsen things
- FTSG > STSG for eyelids due to lower contracture risk
- Contralateral upper lid and retroauricular skin are the gold-standard donor sites for periocular FTSG
- Bolster dressing is mandatory after skin grafting to the eyelid
- Z-plasty is first-line for mild localized scars - it uses local tissue and avoids a donor site
- Serial Z-plasties extend the technique to longer contracted scars
- If posterior lamellar or middle lamellar scarring coexists, mucosal or dermal spacer grafts address that layer separately
- Allow 3-6 months for scar maturation before definitive reconstruction in post-surgical or post-burn cases (unless corneal exposure demands earlier intervention)
Sources: Kanski's Clinical Ophthalmology, 10th ed., p. 84; Andrews' Diseases of the Skin, p. 1030; Mulholland & Greenfield's Surgery, 7th ed., p. 762-765; Cummings Otolaryngology, pp. 385, 532-534; Scott-Brown's Otorhinolaryngology, p. 1323
This is a shared conversation. Sign in to Orris to start your own chat.