Parotid gland
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks with excellent images. Here is the complete response:
Parotid Gland
Overview
The parotid gland is the largest of the three paired major salivary glands. It is ectodermal in origin (unlike the submandibular and sublingual glands, which are endodermal) and develops in the sixth week of gestation from epithelial buds invaginating from the oral mucosa into the surrounding mesenchyme.
Anatomy and Location
The gland occupies the preauricular region and is wedged in a recess bounded by:
- Anterior border: masseter muscle and ramus of the mandible
- Superior border: zygomatic arch
- Posterior border: tragal cartilage and sternocleidomastoid muscle
- Deep border: pretyloid compartment of the parapharyngeal space
The gland extends anteriorly over the masseter and inferiorly over the posterior belly of the digastric muscle. It is irregular in shape because it does not become encapsulated early - nearby vessels, nerves, and lymphatics develop before encapsulation occurs.
The gland is covered by the parotidomasseteric fascia, which attaches to the zygomatic arch superiorly, the mastoid process posteriorly, and blends with the superficial musculoaponeurotic system (SMAS).
Lobes
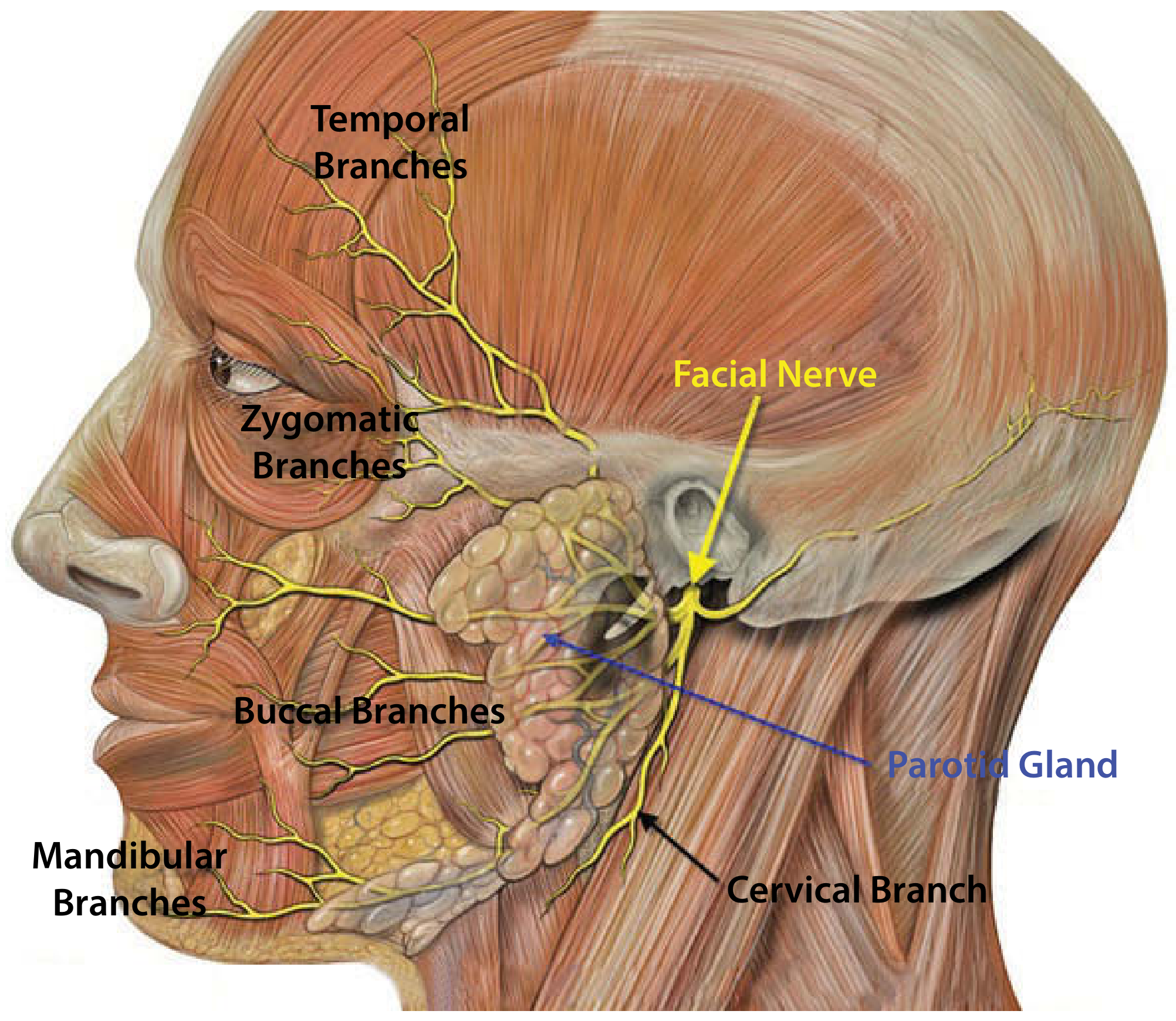
The parotid is arbitrarily divided into two lobes by the facial nerve:
- Superficial lobe - ~80% of the gland parenchyma
- Deep lobe - ~20%; deep parotid tumors can extend into the pretyloid compartment of the parapharyngeal space
Contents Within the Gland
The gland encloses several important structures (from superficial to deep):
| Structure | Details |
|---|---|
| Facial nerve (CN VII) | Divides within the gland forming the pes anserinus |
| Retromandibular vein | Formed by union of maxillary + superficial temporal veins |
| External carotid artery | Divides into maxillary and superficial temporal arteries within the gland |
| Lymph nodes | ~10-20 intraglandular + periglandular nodes (unique to parotid) |
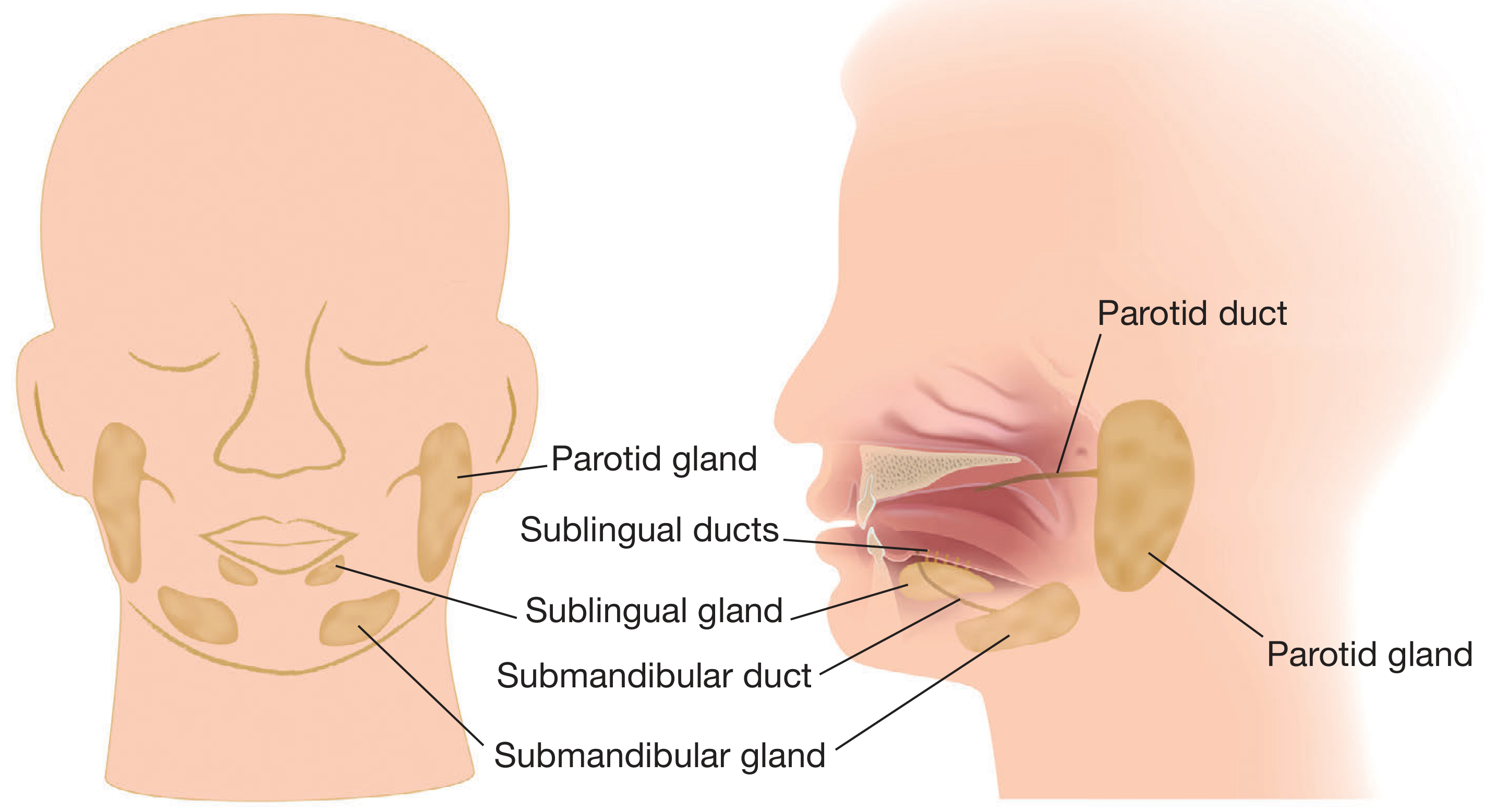
Stensen's Duct (Parotid Duct)
- Traverses anteriorly over the external surface of the masseter muscle
- Turns medially to pierce the buccinator muscle
- Opens into the oral cavity at the parotid papilla, adjacent to the crown of the upper second molar tooth
- An accessory parotid gland (incidence 21-61% in autopsy studies) may lie on the masseter muscle along the duct's course, with a secondary duct joining Stensen's duct
Nerve Supply
| Type | Nerve | Details |
|---|---|---|
| Parasympathetic (secretomotor) | Glossopharyngeal nerve (CN IX) | Via tympanic nerve → lesser petrosal nerve → auriculotemporal nerve |
| Sympathetic | Superior cervical ganglion | Vasomotor innervation |
| Sensory | Auriculotemporal nerve (V3) | Also conveys post-ganglionic parasympathetic fibers |
| Sensory (skin) | Great auricular nerve (C2, C3) | Lower 2/3 of pinna and parotid fascia; can often be preserved during surgery |
The facial nerve exits the stylomastoid foramen (posterolateral to the styloid process, anteromedial to the mastoid process), then enters the posteromedial surface of the parotid and branches. Surgical landmarks to identify the facial nerve include:
- Tympanomastoid suture line
- Posterior belly of the digastric (marks depth)
- Tragal pointer
- Retrograde identification from a peripheral branch
Histology and Secretion
The parotid gland produces almost exclusively serous secretion:
- Serous acini: rounded/polygonal cells with abundant blue cytoplasmic granules (PAS positive)
- Striated ducts and interlobular ducts: cuboidal to columnar lining with eosinophilic cytoplasm
- Myoepithelial cells: line the periphery of both acini and ducts
The fluid is predominantly serous (contrast: sublingual = mucous; submandibular = mixed serous + mucous).
Lymph Nodes
A clinically important feature: the parotid contains 10-20 intraglandular lymph nodes (the submandibular and sublingual glands have no intraglandular nodes). This means many parotid "masses" are actually lymph node metastases from skin cancers (e.g., squamous cell carcinoma, melanoma) of the scalp and face.
Clinical Conditions
Parotitis
- Acute suppurative: usually Staphylococcus aureus; seen in dehydrated/postoperative patients
- Viral (mumps): paramyxovirus; bilateral painful swelling
- Chronic: associated with strictures, sialolithiasis, autoimmune disease (Sjögren syndrome, sarcoidosis)
Tumors
The parotid accounts for the majority of salivary gland neoplasms. An important rule: the smaller the gland, the higher the proportion of malignant tumors (parotid ~25% malignant, submandibular ~50%, sublingual/minor ~75-80%).
| Tumor | Notes |
|---|---|
| Pleomorphic adenoma | Most common benign tumor (65% of all salivary tumors); ductal + myoepithelial cells in cartilage-like stroma; risk of carcinoma ex pleomorphic adenoma if long-standing |
| Warthin tumor | Second most common benign; bilateral in 10%; exclusively in parotid; oncocytic epithelium + lymphoid stroma |
| Mucoepidermoid carcinoma | Most common malignant tumor overall in salivary glands |
| Adenoid cystic carcinoma | Perineural invasion; slow-growing but distant metastases; cribriform pattern |
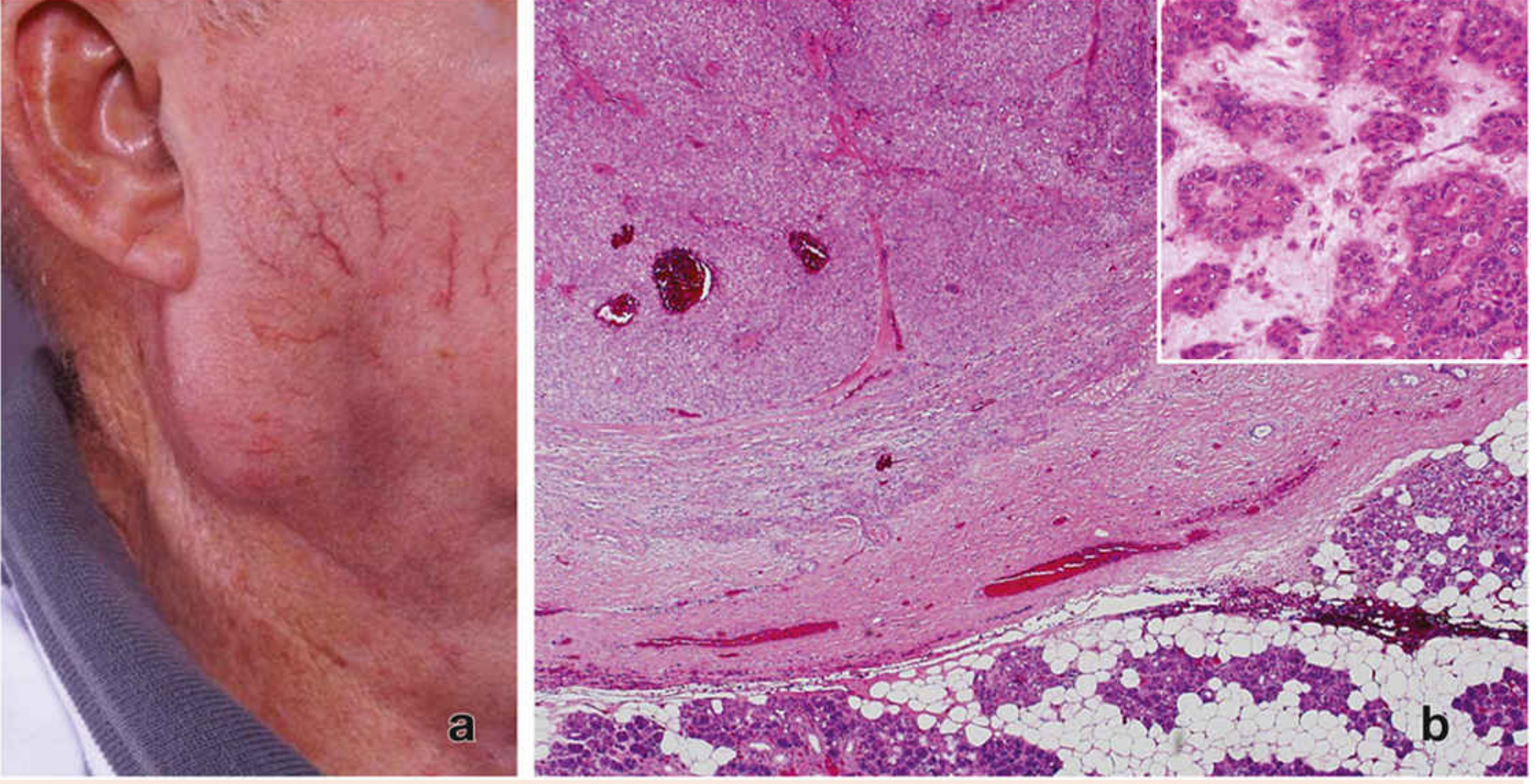
Frey Syndrome (Auriculotemporal Syndrome / Gustatory Sweating)
A complication of parotidectomy. After injury to auriculotemporal nerve fibers, aberrant regeneration causes parasympathetic fibers to reinnervate sweat glands of overlying skin. This results in flushing and sweating of the cheek during eating. Treated with botulinum toxin injection.
Surgery
Superficial parotidectomy (removal of superficial lobe) is the standard operation for most parotid tumors. Total parotidectomy is required for deep lobe tumors or malignancy. The key surgical principle is identification and preservation of the facial nerve. Complications include:
- Facial nerve palsy (temporary > permanent)
- Frey syndrome
- Great auricular nerve numbness
- Salivary fistula
Sources: K.J. Lee's Essential Otolaryngology, p. 642-643; Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Bailey and Love's Short Practice of Surgery 28th Ed., p. 853; Gray's Anatomy for Students; Cummings Otolaryngology; Histology: A Text and Atlas, p. 1487
This is a shared conversation. Sign in to Orris to start your own chat.